You might also like
- Is Your: WritingDocument84 pagesIs Your: WritingVito a sapada Arung wetteNo ratings yet
- Sentence Transformation - Perfect TensesDocument3 pagesSentence Transformation - Perfect TensesMaría Esperanza Velázquez Castillo100% (2)
- Design of Steel TowerDocument31 pagesDesign of Steel Towerudara89% (9)
- Piano 2023 2024 Grade 6Document13 pagesPiano 2023 2024 Grade 6Lucas Moreira0% (1)
- WILDVALLEY SHIPPING CO V CaDocument2 pagesWILDVALLEY SHIPPING CO V CaChariNo ratings yet
- Judicial & Bar CouncilDocument3 pagesJudicial & Bar Councilmitch galaxNo ratings yet
- Ucsp LM PDFDocument124 pagesUcsp LM PDFAivonny Peñaranda CorbitaNo ratings yet
- 1977 Bread UprisingDocument10 pages1977 Bread UprisingHossam el-Hamalawy100% (5)
- Awareness, Knowledge, and Practice For Hepatitis B Infection in Southeast Asia: A Cross-Sectional StudyDocument15 pagesAwareness, Knowledge, and Practice For Hepatitis B Infection in Southeast Asia: A Cross-Sectional StudyAhamed AbdalmajidNo ratings yet
- Wolf Et Al - 2007 - Literacy, Self-Efficacy, and HIV Medication AdherenceDocument8 pagesWolf Et Al - 2007 - Literacy, Self-Efficacy, and HIV Medication Adherencedolf78No ratings yet
- Chapter 2 (Abeleda)Document2 pagesChapter 2 (Abeleda)John Patrick AbeledaNo ratings yet
- Hls 11 s1 11179Document4 pagesHls 11 s1 11179mutiaNo ratings yet
- MMSC Thesis 4Document7 pagesMMSC Thesis 4Matin Ahmad KhanNo ratings yet
- Blocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaDocument8 pagesBlocking The Benefit of Group Based HIV Prevention Efforts During Adolescence - StigmaAMALIA PEBRIYANTINo ratings yet
- Galang Et Al.Document26 pagesGalang Et Al.Angelo BiluanNo ratings yet
- Knowledge, Attitudes and Practice of Nurses Working With HIV/AIDS PatientsDocument14 pagesKnowledge, Attitudes and Practice of Nurses Working With HIV/AIDS PatientsHussein MagdiNo ratings yet
- The Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaDocument11 pagesThe Role of a Pharmacist in the Analysis of Adherence Rates and Associated Factors in HIV-Patients Registered on Centralized Chronic Medicines Dispensing and Distribution (CCMDD) Programme in the Public Sector in South AfricaSabrina JonesNo ratings yet
- Public Health - Vol 2 - Issue 4 - Article 5Document44 pagesPublic Health - Vol 2 - Issue 4 - Article 5kaisamerno2003No ratings yet
- Dickson2016 PDFDocument11 pagesDickson2016 PDFDian MelasariNo ratings yet
- Preventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberDocument9 pagesPreventive Medicine Reports: Samuel R. Bunting, Brian A. Feinstein, Aniruddha Hazra, Neeral K. Sheth, Sarah S. GarberKnowledge PepalaNo ratings yet
- Factors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDocument12 pagesFactors Impacting Antiretroviral Therapy Adherence Among Human Immunodeficiency Virus-Positive Adolescents in Sub-Saharan AfricaDouglas ChukwuNo ratings yet
- Nihms 446239Document9 pagesNihms 446239Aklile TsegaNo ratings yet
- Factors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisDocument16 pagesFactors Influencing HIV Disclosure Among People Living With HIV/AIDS in Nigeria: A Systematic Review Using Narrative Synthesis and Meta-AnalysisTrisna SariNo ratings yet
- Ppa 11 221Document8 pagesPpa 11 221Riska Resty WasitaNo ratings yet
- E20201433 FullDocument15 pagesE20201433 FullcdsaludNo ratings yet
- Tropical Med Int Health - 2023 - Daltro - Virological Failure and Adherence To Antiretroviral Therapy in Adolescents andDocument13 pagesTropical Med Int Health - 2023 - Daltro - Virological Failure and Adherence To Antiretroviral Therapy in Adolescents andCliff Daniel DIANZOLE MOUNKANANo ratings yet
- What Puts Heart Failure Patients at Risk For Poor Medication Adherence?Document12 pagesWhat Puts Heart Failure Patients at Risk For Poor Medication Adherence?ElfiaNeswitaNo ratings yet
- Jkon 11 171Document8 pagesJkon 11 171pangaribuansantaNo ratings yet
- Mansfield 2021Document17 pagesMansfield 2021Adam HafizNo ratings yet
- HIV Knowledge and Perceptions of Risk in A Young, Urban, Drug-Using PopulationDocument6 pagesHIV Knowledge and Perceptions of Risk in A Young, Urban, Drug-Using PopulationEkiNo ratings yet
- Prevalence of Self-Medication and Associated Factors in An Elderly Population: A Systematic ReviewDocument14 pagesPrevalence of Self-Medication and Associated Factors in An Elderly Population: A Systematic ReviewRomário CerqueiraNo ratings yet
- Rapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Document5 pagesRapid Routine Hiv Testing For Psychiatric Inpatients 2155 6113 1000555Elisa BaronNo ratings yet
- Evaluating HIV/AIDS Knowledge and Awareness Dynamics: Insights From Adult Populations in IndiaDocument5 pagesEvaluating HIV/AIDS Knowledge and Awareness Dynamics: Insights From Adult Populations in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Preventive Medicine: SciencedirectDocument11 pagesPreventive Medicine: SciencedirectDewi SunnnNo ratings yet
- 1 s2.0 S1836955319300578 MainDocument12 pages1 s2.0 S1836955319300578 MainSairam PhysioNo ratings yet
- HERO Results From The HERO Study - Treatment-Related Characteristics of The PopulationDocument14 pagesHERO Results From The HERO Study - Treatment-Related Characteristics of The PopulationLaboriusNo ratings yet
- Adherence To HIV Care and Associated Health Functioning Among Youth Living With HIV in Sub-Saharan AfricaDocument15 pagesAdherence To HIV Care and Associated Health Functioning Among Youth Living With HIV in Sub-Saharan AfricaDouglas ChukwuNo ratings yet
- Sandeep Sachdeva Jagbir S. Malik Ruchi Sachdeva Tilak R. SachdevDocument5 pagesSandeep Sachdeva Jagbir S. Malik Ruchi Sachdeva Tilak R. SachdevMatin Ahmad KhanNo ratings yet
- 1 s2.0 S2214139123000203 MainDocument9 pages1 s2.0 S2214139123000203 MainAziza AzizaNo ratings yet
- Harding Brits Sunflower 2009Document4 pagesHarding Brits Sunflower 2009Natalia MutahangNo ratings yet
- Pediatric Adherence To HIV Antiretroviral TherapyDocument13 pagesPediatric Adherence To HIV Antiretroviral Therapyfezia TiffaniNo ratings yet
- Health Literacy For People Living With HIV/Aids: An Integrative ReviewDocument9 pagesHealth Literacy For People Living With HIV/Aids: An Integrative ReviewCyril Jane Caanyagan AcutNo ratings yet
- Tutor - Critical AppraisalDocument8 pagesTutor - Critical AppraisalPriyanka TanwarNo ratings yet
- NIH Public Access: Author ManuscriptDocument11 pagesNIH Public Access: Author ManuscriptmartingomezrNo ratings yet
- 2019 Wagahta Semere - Caregiving For Older Adults With Limited English PDocument7 pages2019 Wagahta Semere - Caregiving For Older Adults With Limited English PAlthea ReyesNo ratings yet
- Real-World Adherence To Antiretroviral Therapy-Gak AdaDocument14 pagesReal-World Adherence To Antiretroviral Therapy-Gak AdaririsNo ratings yet
- HHS Public Access: Nurse Communication Challenges With Health Literacy SupportDocument17 pagesHHS Public Access: Nurse Communication Challenges With Health Literacy SupportRatih puspita DewiNo ratings yet
- Igx004 2993Document1 pageIgx004 2993Arifah Budiarti NurfitriNo ratings yet
- 6371 Measuring Stigma and Discrimination Towards People Living With Hiv Among Health Care Workers in A Tertiary Government Teaching Hospital in The PhilippinesDocument9 pages6371 Measuring Stigma and Discrimination Towards People Living With Hiv Among Health Care Workers in A Tertiary Government Teaching Hospital in The PhilippinesCamia SinagdaNo ratings yet
- Clinical CareDocument8 pagesClinical CareDalilaNo ratings yet
- HIV and TuberculosisDocument9 pagesHIV and TuberculosisDian NinaNo ratings yet
- HIV-related Stigma and Discrimination: A Study of Health Care Workers in Banda Aceh, IndonesiaDocument8 pagesHIV-related Stigma and Discrimination: A Study of Health Care Workers in Banda Aceh, Indonesiasiska khairNo ratings yet
- Economic and Survival Burden of Dysphagia Among Inpatients in The United StatesDocument7 pagesEconomic and Survival Burden of Dysphagia Among Inpatients in The United StatesClaudia Lorena MedinaNo ratings yet
- Hepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesDocument12 pagesHepatitis B Vaccination Coverage Among Health-Care Personnel in The United StatesRio MulyaNo ratings yet
- Ealth Cience Ournal: HIV / AIDS Knowledge, Attitudes and Behaviours of Student NursesDocument22 pagesEalth Cience Ournal: HIV / AIDS Knowledge, Attitudes and Behaviours of Student NursesMark GutierrezNo ratings yet
- Growth in HIV-infected Children On Long-Term Antiretroviral TherapyDocument11 pagesGrowth in HIV-infected Children On Long-Term Antiretroviral TherapyChristian Alexis Loza CorderoNo ratings yet
- UntitledDocument11 pagesUntitledhitesh9876No ratings yet
- 21 25 2 PBDocument8 pages21 25 2 PBAndalis MANo ratings yet
- ProposalDocument14 pagesProposalapi-418780105No ratings yet
- Nihms 1689349Document26 pagesNihms 1689349Dayanne SilvaNo ratings yet
- Patient-Reported Barriers and Facilitators To Antiretroviral Adherence in Sub-Saharan AfricaDocument13 pagesPatient-Reported Barriers and Facilitators To Antiretroviral Adherence in Sub-Saharan AfricaAhmad Ligar SuhermanNo ratings yet
- Factors Associated With Complementary Therapy Use in People Living With HIV/AIDS Receiving Antiretroviral TherapyDocument16 pagesFactors Associated With Complementary Therapy Use in People Living With HIV/AIDS Receiving Antiretroviral TherapyUmiyanti AzizahNo ratings yet
- VIHDocument34 pagesVIHAndres Felipe Iglesias RealesNo ratings yet
- Morbidity and Mortality Weekly Report 2018Document32 pagesMorbidity and Mortality Weekly Report 2018krisNo ratings yet
- Months After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18Document11 pagesMonths After Licensure Human Papillomavirus Vaccination Practices: A Survey of US Physicians 18api-30279712No ratings yet
- Aids 35 463Document13 pagesAids 35 463apatassiNo ratings yet
- Knowledge of HIV-AIDS A Dominant Factor of Antiretroviral Therapeutic Adherence inDocument9 pagesKnowledge of HIV-AIDS A Dominant Factor of Antiretroviral Therapeutic Adherence inArtha RiniNo ratings yet
- Patient Queue Management System: Supriya Burungale, Komal Kurane, Sakshe Mhatre Prof - Deepali VoraDocument3 pagesPatient Queue Management System: Supriya Burungale, Komal Kurane, Sakshe Mhatre Prof - Deepali VoraRiska Resty WasitaNo ratings yet
- Erlini Harmein YeniDocument9 pagesErlini Harmein YeniRiska Resty WasitaNo ratings yet
- Quality-Of-Life Predictor Factors in Patients With SLE and Their Modification After Cognitive Behavioural TherapyDocument8 pagesQuality-Of-Life Predictor Factors in Patients With SLE and Their Modification After Cognitive Behavioural TherapyRiska Resty WasitaNo ratings yet
- (Let's Get Defensive) : Presented by Shruti Sharma, Pharmacology, 2 SemDocument46 pages(Let's Get Defensive) : Presented by Shruti Sharma, Pharmacology, 2 SemRiska Resty WasitaNo ratings yet
- Original Paper: Electronic Supplementary MaterialDocument14 pagesOriginal Paper: Electronic Supplementary MaterialRiska Resty WasitaNo ratings yet
- Pemanfaatan Reminder Tools "Adherence Support System (Ads) " Dalam Terapi Arv (Anti Retroviral)Document7 pagesPemanfaatan Reminder Tools "Adherence Support System (Ads) " Dalam Terapi Arv (Anti Retroviral)Riska Resty WasitaNo ratings yet
- J-REMI: Jurnal Rekam Medik Dan Informasi Kesehatan: E-ISSN: 2721-866X Vol. 2 No. 1 Desember 2020Document10 pagesJ-REMI: Jurnal Rekam Medik Dan Informasi Kesehatan: E-ISSN: 2721-866X Vol. 2 No. 1 Desember 2020Riska Resty WasitaNo ratings yet
- Living With HIV/AIDS: Stigma and Social Discrimination Hidup Dengan HIV/AIDS: Stigma Dan Diskriminasi SosialDocument8 pagesLiving With HIV/AIDS: Stigma and Social Discrimination Hidup Dengan HIV/AIDS: Stigma Dan Diskriminasi SosialRiska Resty WasitaNo ratings yet
- Lester 2010Document8 pagesLester 2010Riska Resty WasitaNo ratings yet
- Conceptualizations of Big Data and Their Epistemological Claims in Healthcare: A Discourse AnalysisDocument21 pagesConceptualizations of Big Data and Their Epistemological Claims in Healthcare: A Discourse AnalysisRiska Resty WasitaNo ratings yet
- HHS Public AccessDocument17 pagesHHS Public AccessRiska Resty WasitaNo ratings yet
- NIH Public Access: Treating Human Autoimmunity: Current Practice and Future ProspectsDocument20 pagesNIH Public Access: Treating Human Autoimmunity: Current Practice and Future ProspectsRiska Resty WasitaNo ratings yet
- Omj D 17 00061Document8 pagesOmj D 17 00061Riska Resty WasitaNo ratings yet
- M.Prasad Naidu: MSC Medical Biochemistry, Ph.D.Research ScholarDocument39 pagesM.Prasad Naidu: MSC Medical Biochemistry, Ph.D.Research ScholarRiska Resty WasitaNo ratings yet
- HHS Public AccessDocument25 pagesHHS Public AccessRiska Resty WasitaNo ratings yet
- Ppa 11 221Document8 pagesPpa 11 221Riska Resty WasitaNo ratings yet
- FDA Regulation of Mobile Health Technologies: Health Law, Ethics, and Human RightsDocument8 pagesFDA Regulation of Mobile Health Technologies: Health Law, Ethics, and Human RightsRiska Resty WasitaNo ratings yet
- Adherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaDocument7 pagesAdherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaRiska Resty WasitaNo ratings yet
- Predicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelDocument10 pagesPredicting Adherence To Antiretroviral Therapy Among Pregnant Women in Guyana: Utility of The Health Belief ModelRiska Resty WasitaNo ratings yet
- Integrative Self-Knowledge and The Harmony of Purpose Model in Iranian Autoimmune PatientsDocument8 pagesIntegrative Self-Knowledge and The Harmony of Purpose Model in Iranian Autoimmune PatientsRiska Resty WasitaNo ratings yet
- Switching of Primary Health Care Providers Among Self-Paid Health Insurance Participants in Denpasar, Bali, IndonesiaDocument8 pagesSwitching of Primary Health Care Providers Among Self-Paid Health Insurance Participants in Denpasar, Bali, IndonesiaRiska Resty WasitaNo ratings yet
- Ishaque PK Pondicherry UniversityDocument34 pagesIshaque PK Pondicherry UniversityRiska Resty WasitaNo ratings yet
- Consumer Switching Behaviour A TheoreticDocument9 pagesConsumer Switching Behaviour A TheoreticRiska Resty WasitaNo ratings yet
- Study of AdulterantsDocument15 pagesStudy of Adulterantsmanonepunch066No ratings yet
- C-Line Drives Engineering Guide 11-2006-EnDocument568 pagesC-Line Drives Engineering Guide 11-2006-EnysaadanyNo ratings yet
- Predestination Vs Free WillDocument4 pagesPredestination Vs Free WillFrancis Heckman100% (2)
- Advanced Fabric Structure and ProductionDocument15 pagesAdvanced Fabric Structure and ProductionmohsinNo ratings yet
- Water Resources Engineering II DamsDocument86 pagesWater Resources Engineering II DamsAdyasha Swayamsiddha AmantaNo ratings yet
- Clybourne Apartments Final ScriptDocument25 pagesClybourne Apartments Final Scriptnasmith55No ratings yet
- FPGA and PLD SurveyDocument29 pagesFPGA and PLD SurveykavitaNo ratings yet
- 2 Obstacle Avoiding Robot PDFDocument7 pages2 Obstacle Avoiding Robot PDFRaj AryanNo ratings yet
- LESSON PLAN World Religion Week 6Document3 pagesLESSON PLAN World Religion Week 6VIRGILIO JR FABINo ratings yet
- Why Should We Cast Vote in IndiaDocument3 pagesWhy Should We Cast Vote in IndiaKrishna Prince M MNo ratings yet
- Mckenzie Ross Resume 3 12 15Document1 pageMckenzie Ross Resume 3 12 15api-281264881No ratings yet
- Rules and Reminders For Online Classes 2Document14 pagesRules and Reminders For Online Classes 2api-220703221No ratings yet
- IIM Indore US Pathway BrochureDocument20 pagesIIM Indore US Pathway Brochurecinofi7972No ratings yet
- MITC Employee Handbook: A Reference Guide For MITC Solutions Most Commonly Used by EmployeesDocument24 pagesMITC Employee Handbook: A Reference Guide For MITC Solutions Most Commonly Used by EmployeesDerek StarkNo ratings yet
- L 8 UniDocument3 pagesL 8 Unidaina AaAaNo ratings yet
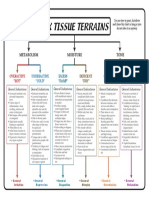
- 6 Tissue Terrains ColorDocument1 page6 Tissue Terrains Colorஆ.க.கோ. இராஜேஷ்வரக் கோன்No ratings yet
- 3306 Mayfair ST.: RFI'sDocument9 pages3306 Mayfair ST.: RFI'sRobbieMaxwellNo ratings yet
- S7-300 and M7-300 Module SpecificationsDocument378 pagesS7-300 and M7-300 Module SpecificationsfayezramadanNo ratings yet
- Psi Engine GM 3 0l Parts ManualDocument22 pagesPsi Engine GM 3 0l Parts Manualchristopherdeanmd190795oad99% (115)
- Core3 SyllabusDocument2 pagesCore3 Syllabusapi-288048801No ratings yet
- Budget Preparation: Lesson 3.2Document24 pagesBudget Preparation: Lesson 3.2JOSHUA GABATERONo ratings yet