You might also like
- Radiography of The Cervical Spine in Trauma. Authors Thad Jackson & Deborah Blades (2002)Document21 pagesRadiography of The Cervical Spine in Trauma. Authors Thad Jackson & Deborah Blades (2002)Sean R. SmithNo ratings yet
- Cervical Spine InjuryDocument18 pagesCervical Spine InjuryGabriel KlemensNo ratings yet
- Dasilva 2020Document4 pagesDasilva 2020Nazmi ZegarraNo ratings yet
- Clavicle FractureDocument6 pagesClavicle FractureYbis LizarzaburuNo ratings yet
- Evaluation and Management of Acute Cervical Spine Trauma-RKY-finalDocument84 pagesEvaluation and Management of Acute Cervical Spine Trauma-RKY-finalRickky MDNo ratings yet
- Cervical Spine Injury: Julie C. LeonardDocument15 pagesCervical Spine Injury: Julie C. LeonardCamilla CristinaNo ratings yet
- Jurnal 5Document16 pagesJurnal 5Melinia Almha RamadhaniNo ratings yet
- Nur 111 Session 17 Sas 1Document8 pagesNur 111 Session 17 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Complete - Medullacervical - Spinal - Cord - Transection - A Case ReportDocument8 pagesComplete - Medullacervical - Spinal - Cord - Transection - A Case Reportkarisman kadirNo ratings yet
- DD Lumbalgia PDFDocument22 pagesDD Lumbalgia PDFJose Antonio Giron MombielaNo ratings yet
- IntroductionDocument41 pagesIntroductionajsealsNo ratings yet
- Decision en FX CervicalesDocument7 pagesDecision en FX CervicalesM Joaquin Robles OrtizNo ratings yet
- Enlsv3.0 Tsi FinalDocument11 pagesEnlsv3.0 Tsi FinalGustavo HenrikeNo ratings yet
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDocument9 pagesMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusNo ratings yet
- Update On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007Document38 pagesUpdate On Traumatic Acute Spinal Cord Injury.: DOI: 10.1016/j.medine.2016.11.007witwiiwNo ratings yet
- Incidence of Cervical Spine Fractures On CT: A Study in A Large Level I Trauma CenterDocument8 pagesIncidence of Cervical Spine Fractures On CT: A Study in A Large Level I Trauma CenterSubarna PaudelNo ratings yet
- Chilean Radiology MagazineDocument34 pagesChilean Radiology MagazineJorge A. Prado BrangoNo ratings yet
- Femur FractureDocument16 pagesFemur FractureM Pino HakimNo ratings yet
- Manejo Inicial Trauma EspinalDocument7 pagesManejo Inicial Trauma EspinalJuan MVNo ratings yet
- 2011 Article 9218Document8 pages2011 Article 9218E=MC2No ratings yet
- Overview of Spinal Cord Injuries - PhysiopediaDocument20 pagesOverview of Spinal Cord Injuries - PhysiopediaRaina Ginella DsouzaNo ratings yet
- Management of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative ManagementDocument12 pagesManagement of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative Managementzee zeeNo ratings yet
- Rachis Cervical GraveDocument5 pagesRachis Cervical GraveCelebre MualabaNo ratings yet
- Bilateral Radial Neck Fracture - Rare Case ReportDocument2 pagesBilateral Radial Neck Fracture - Rare Case ReportIOSRjournalNo ratings yet
- 266 Full PDFDocument7 pages266 Full PDFannisaNo ratings yet
- Vertebral Fractures: Clinical PracticeDocument9 pagesVertebral Fractures: Clinical PracticeIndraYudhiNo ratings yet
- Evaluation and Management of Acute Cervical Spine TraumaDocument20 pagesEvaluation and Management of Acute Cervical Spine TraumasukhmeetphysioNo ratings yet
- ODONTOIDESDocument11 pagesODONTOIDESElianaNo ratings yet
- Dr. Yoyos - Acute Cervical Injury FinalDocument30 pagesDr. Yoyos - Acute Cervical Injury FinalRsud Malinau Ppk BludNo ratings yet
- Spinal Cord Injury (SCI)Document14 pagesSpinal Cord Injury (SCI)Joanna TaylanNo ratings yet
- Spinal Cord InjuryDocument27 pagesSpinal Cord InjuryGargi MP0% (1)
- (10920684 - Neurosurgical Focus) Radiological Evaluation of Cervical Spine Involvement in Rheumatoid ArthritisDocument7 pages(10920684 - Neurosurgical Focus) Radiological Evaluation of Cervical Spine Involvement in Rheumatoid ArthritisPriyank OzaNo ratings yet
- CotoveloDocument7 pagesCotovelorewassallfotosNo ratings yet
- Principles of Spine Trauma and Spinal Deformities PDFDocument34 pagesPrinciples of Spine Trauma and Spinal Deformities PDFVirlan Vasile CatalinNo ratings yet
- AANHS Journal: Comparative Between Syndromic and Non Syndromic Craniosynostosis: A Literature ReviewDocument28 pagesAANHS Journal: Comparative Between Syndromic and Non Syndromic Craniosynostosis: A Literature ReviewHermawan Pramudya IINo ratings yet
- Asuhan Keperawatan Pada Pasien Dengan Trauma Spinal: EssayDocument14 pagesAsuhan Keperawatan Pada Pasien Dengan Trauma Spinal: EssayWina AndiniNo ratings yet
- Neu 2021 0351Document9 pagesNeu 2021 0351divinechp07No ratings yet
- Anky Losing SpondylitisDocument5 pagesAnky Losing SpondylitisdevanbalukhNo ratings yet
- OOI Cervical Spine IniuriesDocument7 pagesOOI Cervical Spine IniurieskeanshengNo ratings yet
- Spinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VDocument79 pagesSpinal Cord Injury: Presented By: Feliciano, Jenard R. Flores, Arliah Q. Gaspar, Danica VPam RomeroNo ratings yet
- Fractures of Clavicle AserDocument44 pagesFractures of Clavicle AserHeba ElgoharyNo ratings yet
- European Journal of Radiology: Roberto Izzo, Gianluigi Guarnieri, Giuseppe Guglielmi, Mario MutoDocument12 pagesEuropean Journal of Radiology: Roberto Izzo, Gianluigi Guarnieri, Giuseppe Guglielmi, Mario MutoEliza LihuNo ratings yet
- Asj 2016 10 6 1058Document7 pagesAsj 2016 10 6 1058Trina ViskhawatNo ratings yet
- Broken Neck (Hangman's Fracture) : DescriptionDocument5 pagesBroken Neck (Hangman's Fracture) : DescriptionFatima RizwanNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- Trauma CervicalDocument36 pagesTrauma CervicalesterhsNo ratings yet
- Diagnosis Dan Tatalaksana Cedera Medula Spinalis Traumatik: Diagnosis and Treatment of Traumatic Spinal Cord InjuryDocument11 pagesDiagnosis Dan Tatalaksana Cedera Medula Spinalis Traumatik: Diagnosis and Treatment of Traumatic Spinal Cord InjuryAna Raniri UtariNo ratings yet
- Cervical RadiculopathyDocument7 pagesCervical Radiculopathyrhymescsf100% (1)
- Asuhan Keperawatan Trauma KapitisDocument38 pagesAsuhan Keperawatan Trauma KapitisRina CantikNo ratings yet
- Contoh LR GADAR CKBDocument13 pagesContoh LR GADAR CKBIntan novia IdNo ratings yet
- DL TPSFDocument5 pagesDL TPSFPramod N KNo ratings yet
- Neck PDFDocument20 pagesNeck PDFManisha KarnaniNo ratings yet
- Spine and Spinal TraumaDocument47 pagesSpine and Spinal TraumaAde Zulfiah100% (1)
- 7015-Article Text-24179-2-10-20180119Document13 pages7015-Article Text-24179-2-10-20180119laizaintanpNo ratings yet
- Complications of Upper Cervical Spine Trauma in Elderly Subjects. A Systematic Review of The LiteratureDocument12 pagesComplications of Upper Cervical Spine Trauma in Elderly Subjects. A Systematic Review of The Literaturebec medNo ratings yet
- Fractures of The Cervical Spine: ReviewDocument7 pagesFractures of The Cervical Spine: ReviewMeri Fitria HandayaniNo ratings yet
- 1 s2.0 S100812752200044X MainDocument7 pages1 s2.0 S100812752200044X MainJuan David Hernández CifuentesNo ratings yet
- Lesion Del Tracto Cortico - Espinal InglesDocument14 pagesLesion Del Tracto Cortico - Espinal InglesCarolina Andrea Daza CharrisNo ratings yet
- Safe Management of Acute Cervical Spine Injuries: Instructional Lecture: TraumaDocument11 pagesSafe Management of Acute Cervical Spine Injuries: Instructional Lecture: TraumaDonate 049No ratings yet
- Hangman's Fracture With Concomitant Atlantoaxial DislocationDocument6 pagesHangman's Fracture With Concomitant Atlantoaxial DislocationPeko PekoNo ratings yet
- Takahata 2015Document5 pagesTakahata 2015Peko PekoNo ratings yet
- Journals J-Neurosurg 22 2 Article-p141-Preview 2Document2 pagesJournals J-Neurosurg 22 2 Article-p141-Preview 2Peko PekoNo ratings yet
- Scarf Related Hangmans Fracture A CaseDocument4 pagesScarf Related Hangmans Fracture A CasePeko PekoNo ratings yet
- Double Hangman's Fracture: ASE EportDocument4 pagesDouble Hangman's Fracture: ASE EportPeko PekoNo ratings yet
- Cervical Fracture With Posterior Ligamentous Injury While SkydivingDocument1 pageCervical Fracture With Posterior Ligamentous Injury While SkydivingPeko PekoNo ratings yet
- Reynolds 2016Document20 pagesReynolds 2016Peko PekoNo ratings yet
- Cervical Spine Hangman Fracture Secondary To A Gelastic SeizureDocument3 pagesCervical Spine Hangman Fracture Secondary To A Gelastic SeizurePeko PekoNo ratings yet
- Hangman's Fracture With Concomitant Atlantoaxial DislocationDocument6 pagesHangman's Fracture With Concomitant Atlantoaxial DislocationPeko PekoNo ratings yet
- Idcases: Case ReportDocument3 pagesIdcases: Case ReportPeko PekoNo ratings yet
- Fracture Dislocation of The Cervical Spine With Gross DisplacementDocument3 pagesFracture Dislocation of The Cervical Spine With Gross DisplacementPeko PekoNo ratings yet
- 7 8 PBDocument42 pages7 8 PBdewi nurhayatiNo ratings yet
- Journals J-Neurosurg 22 2 Article-p141-Preview 2Document2 pagesJournals J-Neurosurg 22 2 Article-p141-Preview 2Peko PekoNo ratings yet
- Integrating Pathology and Radiology Disciplines: An Emerging Opportunity?Document7 pagesIntegrating Pathology and Radiology Disciplines: An Emerging Opportunity?Peko PekoNo ratings yet
- Treatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisDocument5 pagesTreatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisPeko PekoNo ratings yet
- Kesulitan "Weaning" Pada Kasus Flail Chest Akibat Fraktur Sternum Yang Tidak TeridentifikasiDocument9 pagesKesulitan "Weaning" Pada Kasus Flail Chest Akibat Fraktur Sternum Yang Tidak Teridentifikasifaridatul hasanahNo ratings yet
- JRI 13 Full PDFDocument76 pagesJRI 13 Full PDFAGNES TRIANA BASJANo ratings yet
- 10 13 PBDocument72 pages10 13 PBViandra DewiNo ratings yet
- Fractures of The Cervical Spine: ReviewDocument7 pagesFractures of The Cervical Spine: ReviewMeri Fitria HandayaniNo ratings yet
- 8 12 PB PDFDocument39 pages8 12 PB PDFrafiq supriadiNo ratings yet
- Penegakan Diagnosis Dan Penanggulangan Cervicalys Herniated: Nucleus PulposusDocument12 pagesPenegakan Diagnosis Dan Penanggulangan Cervicalys Herniated: Nucleus PulposusMuhammad Rizki Mardiansyah MardiansyahNo ratings yet
- 1 1 PBDocument59 pages1 1 PBPeko PekoNo ratings yet
- 4 5 PBDocument39 pages4 5 PBPeko PekoNo ratings yet
- Jurnal Aceh MedikaDocument5 pagesJurnal Aceh MedikaNabil Sangga BuanaNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFPeko PekoNo ratings yet
- Ipi17959 PDFDocument6 pagesIpi17959 PDFHardiansha WikanNo ratings yet
- Cervical Fracture With Posterior Ligamentous Injury While SkydivingDocument1 pageCervical Fracture With Posterior Ligamentous Injury While SkydivingPeko PekoNo ratings yet
- Reynolds 2016Document20 pagesReynolds 2016Peko PekoNo ratings yet
- Takahata 2015Document5 pagesTakahata 2015Peko PekoNo ratings yet
- Gdlhub GDL s1 2010 Hasdwifaqi 12585 fkm890 KDocument3 pagesGdlhub GDL s1 2010 Hasdwifaqi 12585 fkm890 KPeko PekoNo ratings yet
- PMDC Community Medicine Mcqs PDFDocument280 pagesPMDC Community Medicine Mcqs PDFJay KNo ratings yet
- Foundation of Professional Nursing PracticeDocument5 pagesFoundation of Professional Nursing PracticeIvan LouiseNo ratings yet
- Muet EssaysDocument29 pagesMuet EssaysBabasChongNo ratings yet
- Cannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientDocument7 pagesCannabis-Infused Food and Canadian Consumers' Willingness To Consider "Recreational" Cannabis As A Food IngredientCTV CalgaryNo ratings yet
- Valid RRR Application 2013 - 2017 PDFDocument22,467 pagesValid RRR Application 2013 - 2017 PDFAyub NaveedNo ratings yet
- Nuevas Patologias Cie 10Document281 pagesNuevas Patologias Cie 10Ana guely santivañez mitmaNo ratings yet
- Dheeraj DumirDocument11 pagesDheeraj DumirAnonymous CR8v7xb0No ratings yet
- Hba1C: Quality System CertifiedDocument4 pagesHba1C: Quality System CertifiedNonameNo ratings yet
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Drugs of Autonomic Nervous SystemDocument34 pagesDrugs of Autonomic Nervous SystemWyz Class100% (1)
- Psychological Communication Barriers PosterDocument1 pagePsychological Communication Barriers PostereliyaziyaNo ratings yet
- Michael Simonov CVDocument2 pagesMichael Simonov CVAnonymous QioCrCEVNo ratings yet
- Curriculum Vitae - Aditya Pratama PutraDocument3 pagesCurriculum Vitae - Aditya Pratama PutraIan SeptiantoNo ratings yet
- TermDocument3 pagesTermapi-308717184No ratings yet
- Generic PharmacyDocument20 pagesGeneric PharmacyYna Peregrino38% (8)
- Dental Informatics PlusDocument1 pageDental Informatics PlusNagendra TyagiNo ratings yet
- Assessment of PersonalityDocument3 pagesAssessment of PersonalityRahman ButtNo ratings yet
- Feline Injection-Site Sarcoma - Todays Veterinary PracticeDocument12 pagesFeline Injection-Site Sarcoma - Todays Veterinary PracticeBla bla BlaNo ratings yet
- Bahasa Inggris Swot Madam Gie Sweet Cheek BlushedDocument8 pagesBahasa Inggris Swot Madam Gie Sweet Cheek Blushedanon_681594518No ratings yet
- Sarika RobinsonDocument5 pagesSarika Robinsonapi-355030459No ratings yet
- Learners With Difficulty CommunicatingDocument15 pagesLearners With Difficulty CommunicatingVhong ValleserNo ratings yet
- Flygt IOM 3152-181Document56 pagesFlygt IOM 3152-181veromesa0% (1)
- Eritro Papulo Skuamosa 2021Document47 pagesEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Levels of PreventionDocument23 pagesLevels of Preventionkuruvagadda sagar100% (1)
- Chapter 2 Fire Fighter SafetyDocument2 pagesChapter 2 Fire Fighter SafetyMuhammad Alshikh100% (1)
- 02 2020 Tuaha Adil and Dr. Faisal JamilDocument39 pages02 2020 Tuaha Adil and Dr. Faisal JamilKhadijaNo ratings yet
- House Bill 15-1043Document19 pagesHouse Bill 15-1043Michael_Lee_RobertsNo ratings yet
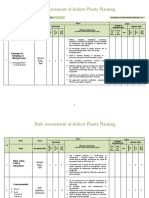
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet
- Are You Planning To Buy or Rent A Home Built Before 1978?Document60 pagesAre You Planning To Buy or Rent A Home Built Before 1978?Maria FloresNo ratings yet
- Antifoam Oh Conz - GHS EngDocument11 pagesAntifoam Oh Conz - GHS EngOUSMAN SEIDNo ratings yet