You might also like
- Standard Welding Procedure SpecificationsDocument2 pagesStandard Welding Procedure SpecificationsAnonymous dh6DITNo ratings yet
- 974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Document64 pages974-0753 Onan RDJC RDJF Diesel Engine Service Manual (09-1984)Leo BurnsNo ratings yet
- Understanding Blow Molding: Norman C. LeeDocument11 pagesUnderstanding Blow Molding: Norman C. LeeKiran ModakNo ratings yet
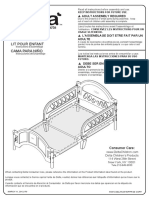
- BB204-Toddler Bed Assembly InstructionsDocument10 pagesBB204-Toddler Bed Assembly InstructionsCaloi PastorfideNo ratings yet
- Transcranial Ultrasound Doppler Parameters in CereDocument7 pagesTranscranial Ultrasound Doppler Parameters in CereImin BuntaraNo ratings yet
- Transcranial Ultrasound Doppler Parameters in Cerebral Vessels May Predict Intracerebral Hemorrhage in Preterm NewbornsDocument7 pagesTranscranial Ultrasound Doppler Parameters in Cerebral Vessels May Predict Intracerebral Hemorrhage in Preterm Newbornsrezza mochamadNo ratings yet
- Inferior Vena Cava Index in Edematous PatientsDocument4 pagesInferior Vena Cava Index in Edematous PatientsfillygogoNo ratings yet
- Ahemd, 2015Document9 pagesAhemd, 2015yosefNo ratings yet
- Estudio de MariDocument6 pagesEstudio de MarianjidisNo ratings yet
- Article 7Document5 pagesArticle 7Kamal SaleemNo ratings yet
- 1 s2.0 S0002914916305574 MainDocument6 pages1 s2.0 S0002914916305574 MainDavid Jimmy Kurniawan RejosaputroNo ratings yet
- Marucci2008 2Document7 pagesMarucci2008 2mjaNo ratings yet
- DMV Cipe Di AtriaDocument6 pagesDMV Cipe Di AtriaAngélica ContrerasNo ratings yet
- Guideline HypoglycemiaDocument6 pagesGuideline HypoglycemialeslyjanetNo ratings yet
- JPM 2005 030Document4 pagesJPM 2005 030Noon ChaiNo ratings yet
- Nirs Preterm ScreeenDocument6 pagesNirs Preterm ScreeenLissaberti AmaliahNo ratings yet
- AcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedDocument6 pagesAcNch05-The Risk of Rebleeding After External Lumbar Drainage in Patients With Untreated RupturedWaldemar PiñaNo ratings yet
- Ductus Venosus Blood Velocity and The Umbilical Artery Circulation in The Seriously Growth Retarded FoetusDocument6 pagesDuctus Venosus Blood Velocity and The Umbilical Artery Circulation in The Seriously Growth Retarded FoetusSaikatBanerjeeNo ratings yet
- Baker 2013Document6 pagesBaker 2013Moni-k GuarnerosNo ratings yet
- PCVS Nirs Pro 2010Document7 pagesPCVS Nirs Pro 2010Maximiliano OliveraNo ratings yet
- Ultrasonido Doppler Temprano AMSDocument7 pagesUltrasonido Doppler Temprano AMSKaren Marbelly OrozcoNo ratings yet
- The Relationship Between Hypoalbuminemia and Intradialytic Hypotension in Haemodialysis Patients 2472 1220 1000165 2Document5 pagesThe Relationship Between Hypoalbuminemia and Intradialytic Hypotension in Haemodialysis Patients 2472 1220 1000165 2melda lestari haidirNo ratings yet
- Placental Pathology and Blood PressureDocument12 pagesPlacental Pathology and Blood PressureEka PutraNo ratings yet
- 10.1097 01.ccm.0000474847.93776.f4Document2 pages10.1097 01.ccm.0000474847.93776.f4nermeen ahmedNo ratings yet
- Postoperative Care in Thoracic SurgeryDocument8 pagesPostoperative Care in Thoracic SurgeryAngélica ContrerasNo ratings yet
- Assessment and Management of Fluid Overload in Children On DialysisDocument10 pagesAssessment and Management of Fluid Overload in Children On DialysisAnneCanapiNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyAlif ZainalNo ratings yet
- Fluid Volume Management inHD - KidInt2023 - 240109 - 095420Document4 pagesFluid Volume Management inHD - KidInt2023 - 240109 - 095420AnaNo ratings yet
- Cardio EstudantesDocument5 pagesCardio EstudantesNestor Torres MarinaNo ratings yet
- Hemodialysis in ChildrenDocument5 pagesHemodialysis in ChildrenEileen del RosarioNo ratings yet
- SaudiJKidneyDisTranspl252438-4286359 115423Document6 pagesSaudiJKidneyDisTranspl252438-4286359 115423yosefNo ratings yet
- The Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsDocument5 pagesThe Long-Term Effects of Arteriovenous Fistula Creation On The Development of Pulmonary Hypertension in Hemodialysis PatientsSaskiaaNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleMiguelNo ratings yet
- Webinar1 Presentation HMforNEXTDocument130 pagesWebinar1 Presentation HMforNEXTAdrian BălanNo ratings yet
- Aaron 2014Document6 pagesAaron 2014Pamela Carvajal AguirreNo ratings yet
- Traducir NeurologiaDocument23 pagesTraducir Neurologiaclara aquino mayangaNo ratings yet
- HD 1Document7 pagesHD 1Arista RachmaNo ratings yet
- Right Ventricular Systolic-to-Diastolic Time Index: Hypoplastic Left Heart Fetuses Differ Significantly From Normal FetusesDocument7 pagesRight Ventricular Systolic-to-Diastolic Time Index: Hypoplastic Left Heart Fetuses Differ Significantly From Normal FetusesLis Borda MuñozNo ratings yet
- Effect of Patient-Triggered Ventilation On RespiratoryDocument7 pagesEffect of Patient-Triggered Ventilation On RespiratoryBryan MaldonadoNo ratings yet
- 416 FullDocument10 pages416 FullKarla HernandezNo ratings yet
- Acta Anaesthesiol Scand - 2022 - JessenDocument10 pagesActa Anaesthesiol Scand - 2022 - Jessenนิ่ม มมNo ratings yet
- Early Extubation After Surgical Repair of Tetralogy of FallotDocument3 pagesEarly Extubation After Surgical Repair of Tetralogy of FallotResiden KardiologiNo ratings yet
- Elevacion Pasiva de Miembros Inferiores Como Predictor de Respuesta A FluidosDocument10 pagesElevacion Pasiva de Miembros Inferiores Como Predictor de Respuesta A Fluidosalejandro montesNo ratings yet
- Original Article: Saudi Journal of Kidney Diseases and TransplantationDocument8 pagesOriginal Article: Saudi Journal of Kidney Diseases and TransplantationAgun FauziNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- Bleeding and Infection With External Ventricular.8 PDFDocument11 pagesBleeding and Infection With External Ventricular.8 PDFAriel Aldo BravoNo ratings yet
- Predictors of Cardio Pulmonary Resuscitation Outcome in Postoperative Cardiac ChildrenDocument5 pagesPredictors of Cardio Pulmonary Resuscitation Outcome in Postoperative Cardiac Childrenhendra pranataNo ratings yet
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 pagesRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNo ratings yet
- CKD5 HDDocument10 pagesCKD5 HDsari murnaniNo ratings yet
- Ircmj 17 06 20705 PDFDocument7 pagesIrcmj 17 06 20705 PDFUchi SuhermanNo ratings yet
- Jurnal 2Document9 pagesJurnal 2Syanindita MaharaniNo ratings yet
- Wu 2018Document8 pagesWu 2018Karel ZertucheNo ratings yet
- Academic Emergency Medicine - 2022 - Jessen - Restrictive Fluids Versus Standard Care in Adults With Sepsis in TheDocument32 pagesAcademic Emergency Medicine - 2022 - Jessen - Restrictive Fluids Versus Standard Care in Adults With Sepsis in TheLenin BlancasNo ratings yet
- Exercise Is Feasible in Patients Receiving Vasoactive Medication in A Cardiac Surgical Intensive Care Unit - A Prospective Observational StudyDocument6 pagesExercise Is Feasible in Patients Receiving Vasoactive Medication in A Cardiac Surgical Intensive Care Unit - A Prospective Observational Studyrayanna dornelesNo ratings yet
- Ucm 439476Document1 pageUcm 439476Fadel BilondatuNo ratings yet
- Vascular Pedicle Width On Chest Radiograph As A MeDocument8 pagesVascular Pedicle Width On Chest Radiograph As A MeSoftwarebolivia EnriqueNo ratings yet
- Hemodynamic Parameters To Guide Fluid Therapy: Review Open AccessDocument9 pagesHemodynamic Parameters To Guide Fluid Therapy: Review Open AccessClaudioValdiviaNo ratings yet
- Intracranial Cerebrospinal FluDocument4 pagesIntracranial Cerebrospinal FluAffan AdibNo ratings yet
- Poor Correlation Between Head Circumference and Cranial Intraventricular HemorrhageDocument6 pagesPoor Correlation Between Head Circumference and Cranial Intraventricular HemorrhageJ Alfonso FJNo ratings yet
- Respiratory Variations in Arterial Pressure For Guiding Fluid Management in Mechanically VDocument8 pagesRespiratory Variations in Arterial Pressure For Guiding Fluid Management in Mechanically VThászk AstrosaNo ratings yet
- Evaluation of Intraventricular Hemorrhage Assessment Methods For Predicting Outcome Following Intracerebral HemorrhageDocument8 pagesEvaluation of Intraventricular Hemorrhage Assessment Methods For Predicting Outcome Following Intracerebral HemorrhageNurul FajriNo ratings yet
- 4 I PDFDocument6 pages4 I PDFDaniel Fernando Mendez CarbajalNo ratings yet
- Pulse Wave Velocity and Its Usefulness in Estimation of HypertensionDocument7 pagesPulse Wave Velocity and Its Usefulness in Estimation of HypertensionJayanthi ThiruvengadamNo ratings yet
- Dialysis Access ManagementFrom EverandDialysis Access ManagementSteven WuNo ratings yet
- Impact of COVID-19 Infection On The Outcome of Patients With Ischemic StrokeDocument10 pagesImpact of COVID-19 Infection On The Outcome of Patients With Ischemic StrokemalisalukmanNo ratings yet
- Fitria Cs Structure NoteDocument6 pagesFitria Cs Structure NotemalisalukmanNo ratings yet
- Form 3 DDD 2019 BaruDocument12 pagesForm 3 DDD 2019 BarumalisalukmanNo ratings yet
- Template Nilai Harian-X.MIPA.1-FisikaDocument90 pagesTemplate Nilai Harian-X.MIPA.1-FisikamalisalukmanNo ratings yet
- Tugas DDD Audit KuantitatifDocument26 pagesTugas DDD Audit KuantitatifmalisalukmanNo ratings yet
- Determination of Intravascular Volume Status byDocument6 pagesDetermination of Intravascular Volume Status bymalisalukmanNo ratings yet
- Which Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsDocument7 pagesWhich Echocardiographic Parameter Is A Better Marker of Volume Status in Hemodialysis PatientsmalisalukmanNo ratings yet
- Evaluating Volume Status in Hem, Odialysis Patients: Dialysis Technical NoteDocument11 pagesEvaluating Volume Status in Hem, Odialysis Patients: Dialysis Technical NotemalisalukmanNo ratings yet
- Inferior Vena Cava Diameter and Collapsibility IndexDocument9 pagesInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanNo ratings yet
- Case Report Heparin-Induced Thrombocytopenia in ADocument7 pagesCase Report Heparin-Induced Thrombocytopenia in AmalisalukmanNo ratings yet
- Physiology CNSDocument125 pagesPhysiology CNSmalisalukmanNo ratings yet
- Board Certification in Vascular and Endovascular MedicineDocument3 pagesBoard Certification in Vascular and Endovascular MedicinemalisalukmanNo ratings yet
- 7th Chemistry DLP Study Package FinalDocument101 pages7th Chemistry DLP Study Package FinalAdityaNo ratings yet
- TransportationDocument4 pagesTransportationShrinidhi Priyankaa 1912985630No ratings yet
- Datasheet - 74LS283 - Somador Binário Completo de 4 BitsDocument7 pagesDatasheet - 74LS283 - Somador Binário Completo de 4 BitsLucas CarvalhoNo ratings yet
- Mono and DicotDocument3 pagesMono and Dicotlady chaseNo ratings yet
- PAMDocument14 pagesPAMRashed IslamNo ratings yet
- Queueing TheoryDocument6 pagesQueueing TheoryElmer BabaloNo ratings yet
- Recognizing and Classifying Daily Human Activities: Group-22Document23 pagesRecognizing and Classifying Daily Human Activities: Group-22Divyam GuptaNo ratings yet
- BHHHJDocument10 pagesBHHHJAnonymous vLerKYANo ratings yet
- Concept Paper Group 1Document9 pagesConcept Paper Group 1Kaime KeilarNo ratings yet
- Car Frontal ImpactDocument25 pagesCar Frontal Impactapi-3762972100% (1)
- 1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroDocument80 pages1 Stack Testing Source Policy - RA 8749 Legal Oct 2019 Updates - Engr. Jundy Del SocorroJayson ResultayNo ratings yet
- The National TerritoryDocument39 pagesThe National TerritoryRan RanNo ratings yet
- Falsework For Concrete Structures - Guidelines: Indian StandardDocument24 pagesFalsework For Concrete Structures - Guidelines: Indian StandardLivinston JosephNo ratings yet
- Optoelectronics Circuit CollectionDocument18 pagesOptoelectronics Circuit CollectionSergiu CristianNo ratings yet
- Lecture-I Introduction To Concrete TechnologyDocument102 pagesLecture-I Introduction To Concrete Technologyjs kalyana rama100% (4)
- Bubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. WilsonDocument14 pagesBubble Growth in A Two-Dimensional Viscoelastic Foam: S.L. Everitt, O.G. Harlen, H.J. Wilsonliviagoncalves197271No ratings yet
- January 2005 6677 Mechanics M1: Mark SchemeDocument7 pagesJanuary 2005 6677 Mechanics M1: Mark SchemeWael TareqNo ratings yet
- 2005 Removing Aland RegeneratingDocument6 pages2005 Removing Aland RegeneratingHebron DawitNo ratings yet
- GD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0Document13 pagesGD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0AbbasNo ratings yet
- Roberto Del RosarioDocument19 pagesRoberto Del RosarioCarl llamasNo ratings yet
- Op CdmaDocument19 pagesOp Cdmarosev15No ratings yet
- Heat Shrink CoatingDocument5 pagesHeat Shrink CoatingMekhmanNo ratings yet
- S800 SCL SR - 2CCC413009B0201 PDFDocument16 pagesS800 SCL SR - 2CCC413009B0201 PDFBalan PalaniappanNo ratings yet
- Training Matrix Competency 4 Organic ConcoctionsDocument3 pagesTraining Matrix Competency 4 Organic ConcoctionsST. ISIDORE THE FARMERNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- Língua Inglesa: Reported SpeechDocument3 pagesLíngua Inglesa: Reported SpeechPatrick AlmeidaNo ratings yet