You might also like
- Hard Bound Osteoporosis Case Report Group 3Document21 pagesHard Bound Osteoporosis Case Report Group 3Jewenson SalvadorNo ratings yet
- Management of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoDocument15 pagesManagement of Patients With Dysrhythmias and Conduction Problems Dr. SydioncoRoyce Vincent Tizon100% (1)
- Lecture 3:osteoarthritis (2007 Powerpoint)Document54 pagesLecture 3:osteoarthritis (2007 Powerpoint)j.doe.hex_87100% (1)
- POTT's DISEASEDocument33 pagesPOTT's DISEASEJemimah A. Mangalindan100% (4)
- Paget's Disease of The Mandible - A Review and Report of A CaseDocument5 pagesPaget's Disease of The Mandible - A Review and Report of A CaseFlorin IonescuNo ratings yet
- Final - Bme 298 Final Project SkeletonDocument22 pagesFinal - Bme 298 Final Project Skeletonapi-522861974No ratings yet
- MSK Study Schedule 2Document12 pagesMSK Study Schedule 2Aashish GiriNo ratings yet
- حل اسئلة العملي-1Document91 pagesحل اسئلة العملي-1حسام الوجيهNo ratings yet
- Paget's Disease in Service TrainingDocument4 pagesPaget's Disease in Service TrainingrinninNo ratings yet
- ResearchDocument3 pagesResearchDr Sreeja KSNo ratings yet
- Pott's Disease MEDICAL MANAGEMENTDocument3 pagesPott's Disease MEDICAL MANAGEMENTRuby Anna BorceNo ratings yet
- Fraktur PatologisDocument4 pagesFraktur PatologisPinka ChairulNo ratings yet
- Musculoskeletal Disorders: Assessment and Diagnostic Test AssessmentDocument10 pagesMusculoskeletal Disorders: Assessment and Diagnostic Test AssessmentAl-Mansor MoayadNo ratings yet
- Osteoarthritis AapmrDocument5 pagesOsteoarthritis AapmrBiandaNo ratings yet
- Case Report OsteochondromaDocument43 pagesCase Report OsteochondromaFidesha Nurganiah SiregarNo ratings yet
- Paget's Disease of The BoneDocument9 pagesPaget's Disease of The BonePam RomeroNo ratings yet
- Case ReportDocument3 pagesCase Reportandrul556723No ratings yet
- Spondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesDocument4 pagesSpondylosis, Degeneration of Intervertebral Disc Diagnosis/Condition: ICD-9 CodesAloysius DicodemusNo ratings yet
- Perthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore PakistanDocument68 pagesPerthes Disease: by Dr. Abdul Karim Postgraduate Resident Orthopedic Surgery Pgmi/Lgh. Lahore Pakistandrakkashmiri50% (2)
- JurnalDocument5 pagesJurnalQorin Diin ArifniNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportspecheniqNo ratings yet
- A. Congenital Radioulnar Synostosis: Self-Directed LearningDocument6 pagesA. Congenital Radioulnar Synostosis: Self-Directed Learningapi-477982644No ratings yet
- Ankylosing Apondylitis of Temporomandibular Joint (TMJ) : February 2012Document13 pagesAnkylosing Apondylitis of Temporomandibular Joint (TMJ) : February 2012Billy PeterNo ratings yet
- Trauma - Intertrochanteric Fracture - RustiniDocument7 pagesTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08No ratings yet
- Knee Osteoarthritis: DefinitionDocument19 pagesKnee Osteoarthritis: DefinitionShrouq BadrNo ratings yet
- Protrusio Acetabuli Diagnosis and TreatmentDocument10 pagesProtrusio Acetabuli Diagnosis and TreatmentFerney Leon BalceroNo ratings yet
- Delayed Union 0 Nonunion - Management PrincipleDocument50 pagesDelayed Union 0 Nonunion - Management PrincipleBimnilson SinghNo ratings yet
- ARTHRITIS LectureDocument5 pagesARTHRITIS LectureMacDonald KarikariNo ratings yet
- Clinical Manifestations, Diagnosis, and Treatment of OsteomalaciaDocument21 pagesClinical Manifestations, Diagnosis, and Treatment of Osteomalaciacvillafane1483100% (2)
- Sarver PDFDocument8 pagesSarver PDFanon_768201406No ratings yet
- Degenerative Joint DiseasesDocument30 pagesDegenerative Joint DiseasesBahaa ShaabanNo ratings yet
- Osteoporosis SarveshDocument41 pagesOsteoporosis Sarveshdrsarvesh100% (1)
- Nitesh Kumar Rheumatoid ArthritisDocument8 pagesNitesh Kumar Rheumatoid Arthritisnitesh kumarNo ratings yet
- Osteoarthritis of HipDocument3 pagesOsteoarthritis of Hipjcachica21No ratings yet
- POTT's DiseaseDocument3 pagesPOTT's DiseaseFema Jill AtrejenioNo ratings yet
- Typical Clinical Symptoms Are Pain, Particularly After ProlongedDocument12 pagesTypical Clinical Symptoms Are Pain, Particularly After Prolongedifa afifahNo ratings yet
- Case Series OIDocument6 pagesCase Series OIJulius JuliusNo ratings yet
- Non Neoplastic Bone DiseasesDocument73 pagesNon Neoplastic Bone DiseasesRubyrose TagumNo ratings yet
- Killinger 2010Document8 pagesKillinger 2010Andrea TixeNo ratings yet
- BMJ 2006 p639Document5 pagesBMJ 2006 p639Wahab RasyidNo ratings yet
- DsdfdfsDocument33 pagesDsdfdfsmayliaNo ratings yet
- Osteoarthritis: OsteoartriteDocument9 pagesOsteoarthritis: OsteoartriteSofia Cerezo MuñozNo ratings yet
- Rheumatoid Disorder Imaging - Refarat Radiologi IkramDocument18 pagesRheumatoid Disorder Imaging - Refarat Radiologi Ikramikram hanafiNo ratings yet
- Osteoid OsteomaDocument6 pagesOsteoid OsteomadrkaushikduttaNo ratings yet
- Medscape Knee OCDDocument16 pagesMedscape Knee OCDDita Ambarsari SyafruddinNo ratings yet
- Case Report (Ola)Document44 pagesCase Report (Ola)amel015No ratings yet
- Case Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewDocument4 pagesCase Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewOBLIVION_29No ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- JCRMHS 1286Document3 pagesJCRMHS 1286Juan Jose SantivañezNo ratings yet
- Unusual Cause of Shoulder PainDocument3 pagesUnusual Cause of Shoulder PainElias Oktovianus HaulussyNo ratings yet
- Lecture 40 March 14th-MSKDocument5 pagesLecture 40 March 14th-MSKapi-26938624No ratings yet
- 05.15.17 Bone Pathology (Atkinson) - NotesDocument8 pages05.15.17 Bone Pathology (Atkinson) - NotesDan WuiytNo ratings yet
- Evan, MD Orthopaedic and Traumatology University of Kristen Krida WacanaDocument39 pagesEvan, MD Orthopaedic and Traumatology University of Kristen Krida WacanaIyannyanNo ratings yet
- Nelson EWDocument6 pagesNelson EWDewidewidewi Madridista Part IINo ratings yet
- Total Knee Replacement: Done By: Sajeda Moha'dDocument27 pagesTotal Knee Replacement: Done By: Sajeda Moha'dlolo223No ratings yet
- Slides by Dan Mandel, MD UC Irvine School of MedicineDocument45 pagesSlides by Dan Mandel, MD UC Irvine School of Medicineaddison wood100% (4)
- PanosteitisDocument5 pagesPanosteitisElEffe100% (1)
- Low Grade Central Osteosarcoma Arising From Bone Infarct A Case ReportDocument3 pagesLow Grade Central Osteosarcoma Arising From Bone Infarct A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 1952 - Murphy - Musculotendinous Injuries in Sporting DogsDocument5 pages1952 - Murphy - Musculotendinous Injuries in Sporting DogsYaiza Garcia CasadoNo ratings yet
- Polymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandPolymyalgia Rheumatica, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (2)
- Moodule 12Document14 pagesMoodule 12camille nina jane navarroNo ratings yet
- Module 14Document5 pagesModule 14camille nina jane navarroNo ratings yet
- Module 13Document11 pagesModule 13camille nina jane navarroNo ratings yet
- Module 11Document35 pagesModule 11camille nina jane navarroNo ratings yet
- Control of Noncommunicab Le DiseasesDocument14 pagesControl of Noncommunicab Le Diseasescamille nina jane navarroNo ratings yet
- Topic 1: Implementing Family Nursing Care PlanDocument28 pagesTopic 1: Implementing Family Nursing Care Plancamille nina jane navarroNo ratings yet
- 10-Month-Old Patient With Severe Abdominal Distention and LethargyDocument7 pages10-Month-Old Patient With Severe Abdominal Distention and Lethargycamille nina jane navarroNo ratings yet
- Case Presentation 3Document5 pagesCase Presentation 3camille nina jane navarroNo ratings yet
- 18-Month-Old Boy With Abdominal Pain and Rectal Bleeding BackgroundDocument5 pages18-Month-Old Boy With Abdominal Pain and Rectal Bleeding Backgroundcamille nina jane navarroNo ratings yet
- Module 5Document9 pagesModule 5camille nina jane navarroNo ratings yet
- Module 5 104Document17 pagesModule 5 104camille nina jane navarroNo ratings yet
- Module 4: The Family (2 Hours)Document17 pagesModule 4: The Family (2 Hours)camille nina jane navarroNo ratings yet
- Module 6Document13 pagesModule 6camille nina jane navarroNo ratings yet
- Module 3Document19 pagesModule 3camille nina jane navarroNo ratings yet
- Toksikologi: Vidi Ika Hastari Stikes Harapan Bangsa Jember 2020Document167 pagesToksikologi: Vidi Ika Hastari Stikes Harapan Bangsa Jember 2020Akhmad.Arief.NofiantoNo ratings yet
- Lipiodol Quality 2Document6 pagesLipiodol Quality 2munnaunicorn10No ratings yet
- Module 1: Classification of Herbal Medicines: RetusaDocument2 pagesModule 1: Classification of Herbal Medicines: RetusaMaya Audrey KanekoNo ratings yet
- Good Manufacturing Practice (GMP)Document31 pagesGood Manufacturing Practice (GMP)anandaiprNo ratings yet
- Workshop 8. Badac Plan of ActionDocument1 pageWorkshop 8. Badac Plan of Actionjudy mar delacruzNo ratings yet
- Info AconiteDocument8 pagesInfo AconiteAndreea Cúrea100% (1)
- An Organizational Chart of A Typical Manufacturing CompanyDocument4 pagesAn Organizational Chart of A Typical Manufacturing Companyheyyo ggNo ratings yet
- Autonomic Dysfunction and Hypotension: Christopher J. MathiasDocument28 pagesAutonomic Dysfunction and Hypotension: Christopher J. MathiaswaltercarvalhoNo ratings yet
- Om Health Campus Affiliated To Purbanchal University Gopikrishnanagar, KathmanduDocument107 pagesOm Health Campus Affiliated To Purbanchal University Gopikrishnanagar, KathmanduAdditi SatyalNo ratings yet
- Pedia Tickler 2 1 2Document106 pagesPedia Tickler 2 1 2Ma. Bernadette PinedaNo ratings yet
- Neurotransmitter Chart-1Document1 pageNeurotransmitter Chart-1Amanda CovertNo ratings yet
- Allopregnanolone (3r-Hydroxy-5r-Pregnan-20-One) Derivatives With A Polar Chain in Position 16r: Synthesis and ActivityDocument7 pagesAllopregnanolone (3r-Hydroxy-5r-Pregnan-20-One) Derivatives With A Polar Chain in Position 16r: Synthesis and ActivityBianca AlinaNo ratings yet
- Tugas Farmasi Klinik - Ebm - Kelompok 4Document8 pagesTugas Farmasi Klinik - Ebm - Kelompok 4verra nurmaylindhaNo ratings yet
- JNC 8 2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsDocument40 pagesJNC 8 2014 Evidence-Based Guidelines For The Management of High Blood Pressure in AdultsArum Nadia HafifiNo ratings yet
- Must Know CorrectionsDocument1 pageMust Know CorrectionsJaneNo ratings yet
- Article WJPR 1504835895 PDFDocument11 pagesArticle WJPR 1504835895 PDFQUALITY12No ratings yet
- Pathological Mechanisms and Therapeutic Strategies For ADDocument24 pagesPathological Mechanisms and Therapeutic Strategies For ADShuaib AhmadNo ratings yet
- 2011 Article 151Document5 pages2011 Article 151dgracereid_693082078No ratings yet
- 2013 Kamatou - Menthol A Simple Monoterpene With Remarkable Biological PropertiesDocument11 pages2013 Kamatou - Menthol A Simple Monoterpene With Remarkable Biological PropertiesDouimni AyoubNo ratings yet
- Drug StudyDocument8 pagesDrug StudyAysaaa DCNo ratings yet
- Belanja ObatDocument5 pagesBelanja ObatginanjarNo ratings yet
- A Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and ColchicineDocument4 pagesA Case of Ulcerative Livedoid Vasculopathy Treated Successfully With Pentoxifylline and Colchicinekahkashanahmed065No ratings yet
- ProductsDocument106 pagesProductsbochieng404No ratings yet
- TDM335782 111022101613 InvoiceDocument1 pageTDM335782 111022101613 InvoiceBalayya PattapuNo ratings yet
- Drug StudyDocument32 pagesDrug StudyJoanne Bernadette Aguilar100% (1)
- 646-Article Text-1253-1-10-20190510Document2 pages646-Article Text-1253-1-10-20190510Tara acharyaNo ratings yet
- Pharmacological Profile of Cassia Occidentalis L - A ReviewDocument6 pagesPharmacological Profile of Cassia Occidentalis L - A ReviewjaswantNo ratings yet
- 1 4927329208029413644 PDFDocument578 pages1 4927329208029413644 PDFWaseem UllahNo ratings yet
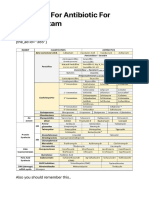
- Summary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study DataDocument5 pagesSummary For Antibiotic For USMLE Exam - USMLE MATERIALS - Updated USMLE Study Dataomy yadavNo ratings yet