You might also like
- Trainee's Performance Appraisal FormDocument4 pagesTrainee's Performance Appraisal Formazrulfadjri67% (3)
- IDP SampleDocument8 pagesIDP SampleRussel Saracho100% (1)
- Flanagan Industrial TestsDocument3 pagesFlanagan Industrial TestsshaelNo ratings yet
- Prime-Hrm Assessment CheckllistDocument9 pagesPrime-Hrm Assessment CheckllistTimothy Tuason100% (1)
- Prime-Hrm Forum 2017 - RSPDocument28 pagesPrime-Hrm Forum 2017 - RSPJonalyn Emen100% (3)
- Individual Development Plan (Blank Form)Document2 pagesIndividual Development Plan (Blank Form)Rouella May Altar100% (1)
- HRM-RP - TH Separating and Retaining EmployeesDocument3 pagesHRM-RP - TH Separating and Retaining EmployeesPavi Antoni VillaceranNo ratings yet
- Glazer Stress Control Lifestyle Question A IreDocument3 pagesGlazer Stress Control Lifestyle Question A IreHanah Spence Haynes100% (1)
- Office of The Team Leader: Commission On AuditDocument4 pagesOffice of The Team Leader: Commission On Auditrussel1435100% (1)
- Absenteeism PolicyDocument3 pagesAbsenteeism PolicyHannah MananquilNo ratings yet
- 5 Components of Human Resource ManagementDocument7 pages5 Components of Human Resource ManagementClifford Jay Calihat100% (1)
- Employee Exit Policy2191Document3 pagesEmployee Exit Policy2191Sahil JunejaNo ratings yet
- Internal Job Application Insider GuideDocument3 pagesInternal Job Application Insider GuideAaron Rapha RosalesNo ratings yet
- Training Ojt Action Plan Supervisor Sample 1 PDFDocument8 pagesTraining Ojt Action Plan Supervisor Sample 1 PDFYe JoonNo ratings yet
- Ojt Bpsu Moa 2017 Update2Document4 pagesOjt Bpsu Moa 2017 Update2John Dell TolentinoNo ratings yet
- Module 2A - LCPP 1Document8 pagesModule 2A - LCPP 1Ma Portia Jasmin Tabogoc0% (2)
- Sharpen The Saw - Activity WorksheetDocument6 pagesSharpen The Saw - Activity WorksheetClarence Tan100% (1)
- IDP ArlDocument4 pagesIDP ArlErick Jay InokNo ratings yet
- CS Form No. 7 Clearance Blank FormDocument5 pagesCS Form No. 7 Clearance Blank FormNachoNo ratings yet
- Car Sticker GuidelinesDocument3 pagesCar Sticker GuidelinesDen SamonteNo ratings yet
- 2-YEAR IDP FOR LEGAL OFFICERDocument2 pages2-YEAR IDP FOR LEGAL OFFICERJunDagzNo ratings yet
- Nature, Theories and Application of Motivation Needs and ValuesDocument10 pagesNature, Theories and Application of Motivation Needs and ValueshambogalagaNo ratings yet
- Report (Performance Appraisal)Document45 pagesReport (Performance Appraisal)Sirshar Ahmed AbbasiNo ratings yet
- CS Form No. 212 Attachment Work Experience SheetDocument2 pagesCS Form No. 212 Attachment Work Experience SheetLimar Anasco Escaso100% (1)
- Comprehensive Report on School Classroom ObservationsDocument3 pagesComprehensive Report on School Classroom ObservationsBhat MushtaqNo ratings yet
- HRM PlanningDocument13 pagesHRM PlanningAmashi CostaNo ratings yet
- Primary Responsibilities of an HR ManagerDocument4 pagesPrimary Responsibilities of an HR Managermariyam0% (1)
- Form 33 NewDocument2 pagesForm 33 NewJane Heart ManuelNo ratings yet
- Toga Rental ContractDocument8 pagesToga Rental ContractClaire CabactulanNo ratings yet
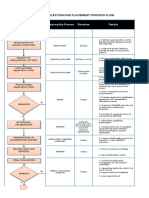
- 9.1 Flow Chart RSPDocument3 pages9.1 Flow Chart RSPmahal79No ratings yet
- Employee Clearance FormDocument1 pageEmployee Clearance FormRrichard Prieto Mmallari100% (1)
- Employee Performance EvaluationDocument4 pagesEmployee Performance Evaluationisagani abril100% (1)
- Training Effectiveness Evaluation FormDocument2 pagesTraining Effectiveness Evaluation FormAireen Letana Siaga100% (1)
- Training Needs Analysis Questionnaire: Basic DataDocument5 pagesTraining Needs Analysis Questionnaire: Basic DatarishiganeshNo ratings yet
- Complete Copy of The Competency Standards For CESOsDocument67 pagesComplete Copy of The Competency Standards For CESOsramil_sanchez50% (2)
- Interview Evaluation FormDocument3 pagesInterview Evaluation FormAnthony RiggsNo ratings yet
- CSC Competency Tables 2011Document15 pagesCSC Competency Tables 2011Erica MuñozNo ratings yet
- Training Session Evaluation Form InstructionsDocument8 pagesTraining Session Evaluation Form Instructionsaaronjules100% (1)
- Annual HRD PlanDocument16 pagesAnnual HRD PlanE Robert SNo ratings yet
- JOB INTERVIEW SCORING RUBRICDocument2 pagesJOB INTERVIEW SCORING RUBRICJM Hernandez VillanuevaNo ratings yet
- Ojt Performance Evaluation: Basak, Cebu CityDocument2 pagesOjt Performance Evaluation: Basak, Cebu CityIrah MarieNo ratings yet
- Designing of TrainingDocument16 pagesDesigning of Training20apr1No ratings yet
- Competency-Based JD GuideDocument25 pagesCompetency-Based JD GuidecruscadenNo ratings yet
- Employee Attendance PolicyDocument4 pagesEmployee Attendance PolicyThink BigNo ratings yet
- HR B2 Linked With Plantilla Sample OnlyDocument30 pagesHR B2 Linked With Plantilla Sample OnlyBenjamin FalladoNo ratings yet
- Paf FormDocument4 pagesPaf FormFauzi LyandaNo ratings yet
- SBN-1006: Salary Standardization Law VDocument8 pagesSBN-1006: Salary Standardization Law VRalph Recto100% (1)
- CS Form 33 - Appointment FormDocument2 pagesCS Form 33 - Appointment FormAldrin Paguirigan100% (1)
- Personnel AdministrationDocument27 pagesPersonnel Administrationrenusiki100% (1)
- Trophies and TragediesDocument2 pagesTrophies and TragediesJose Erwin BorbonNo ratings yet
- HR Functions: 1. Employee FinancesDocument2 pagesHR Functions: 1. Employee FinancesVishnu ChNo ratings yet
- Asking Question Discussing His/her Views or Listening Constructive Criticism Citing Ideas From PreviousDocument1 pageAsking Question Discussing His/her Views or Listening Constructive Criticism Citing Ideas From PreviousIana CruzNo ratings yet
- University of Northern PhilippinesDocument1 pageUniversity of Northern PhilippinesKathleen Joy PingenNo ratings yet
- Employee Transfer and Promotion PolicyDocument31 pagesEmployee Transfer and Promotion PolicyFriti Friti100% (1)
- Sample Internal Job PostingDocument2 pagesSample Internal Job PostingSamule PaulNo ratings yet
- Level 1 Field Experience Exit Conference ReflectionDocument1 pageLevel 1 Field Experience Exit Conference ReflectionNel BorniaNo ratings yet
- Grievance CommitteeDocument6 pagesGrievance Committeeboopathi.n100% (1)
- Prime HRM Recruitment Selection and PlacementDocument29 pagesPrime HRM Recruitment Selection and PlacementlilaquitaineNo ratings yet
- Competency Evaluation Form SampleDocument15 pagesCompetency Evaluation Form Sampleanser lal50% (2)
- Performance EvaluationDocument2 pagesPerformance EvaluationMarie Aranas100% (1)
- Part A: Competency Assessment and Development Priorities: Individual Development Plan (Idp)Document4 pagesPart A: Competency Assessment and Development Priorities: Individual Development Plan (Idp)Russel Saracho100% (1)
- Philippine Statistics Authority Employee Development PlanDocument2 pagesPhilippine Statistics Authority Employee Development PlanIsah MiguelNo ratings yet
- Kindergarten: Siyahan Nga Bahin: Semana 1 - Naiiba AkoDocument12 pagesKindergarten: Siyahan Nga Bahin: Semana 1 - Naiiba AkoMichelle CasinNo ratings yet
- Overview of The Technical Program of Brigada PagbasaDocument11 pagesOverview of The Technical Program of Brigada PagbasaMichelle CasinNo ratings yet
- Two Track Method - Wilfredo RamirezDocument31 pagesTwo Track Method - Wilfredo RamirezMichelle CasinNo ratings yet
- WHLP Q4 Week 31-40Document29 pagesWHLP Q4 Week 31-40Michelle CasinNo ratings yet
- Monitoring Tool For Learners: Curry Elementary SchoolDocument1 pageMonitoring Tool For Learners: Curry Elementary SchoolMichelle CasinNo ratings yet
- Report On Implementation of L&D Program FormDocument1 pageReport On Implementation of L&D Program FormMichelle CasinNo ratings yet
- Northwest Samar State University HRD Learning SystemDocument5 pagesNorthwest Samar State University HRD Learning SystemMichelle CasinNo ratings yet
- Northwest Samar State University IDP TemplateDocument2 pagesNorthwest Samar State University IDP TemplateMichelle CasinNo ratings yet
- Sample of Evaluation FormDocument2 pagesSample of Evaluation FormMichelle CasinNo ratings yet
- Metacognitive Regulation ModuleDocument7 pagesMetacognitive Regulation ModuleMichelle Casin100% (1)
- Sample Training ProposalDocument6 pagesSample Training ProposalMichelle CasinNo ratings yet
- Module 1C - Metacognitive InstructionDocument5 pagesModule 1C - Metacognitive InstructionMichelle Casin100% (2)
- Module 1A - Metacognition & Metacognitive KnowledgeDocument6 pagesModule 1A - Metacognition & Metacognitive KnowledgeMa Portia Jasmin Tabogoc100% (1)
- Learner-Centered Teaching: Venancio P. Bajet College of Teacher EducationDocument39 pagesLearner-Centered Teaching: Venancio P. Bajet College of Teacher EducationMichelle CasinNo ratings yet
- (EBPH) : Mengembangkan Evidence Based Public Health Hiv Dan Aids Berbasis SurveilansDocument8 pages(EBPH) : Mengembangkan Evidence Based Public Health Hiv Dan Aids Berbasis SurveilansDamiriNo ratings yet
- 20 Đề tham khảo tuyển sinh vào lớp 10 2022Document87 pages20 Đề tham khảo tuyển sinh vào lớp 10 2022nguyethuhang.hnNo ratings yet
- Medication AdministrationDocument61 pagesMedication Administrationkerema BadasaNo ratings yet
- Practice Sheet Session 2 - 2021 - Student SheetDocument2 pagesPractice Sheet Session 2 - 2021 - Student SheetAlisa SayNo ratings yet
- Occlusal Plane Template TechniqueDocument39 pagesOcclusal Plane Template TechniqueREWA KAWADENo ratings yet
- Important Issues in IHRMDocument3 pagesImportant Issues in IHRMsam130488No ratings yet
- SPTL Ohs&e 40 Ohse MPR AbrarDocument22 pagesSPTL Ohs&e 40 Ohse MPR AbrarRanjeet Kumar SinghNo ratings yet
- Professional Teachers (Secondary) 10-2022 FilipinoDocument26 pagesProfessional Teachers (Secondary) 10-2022 FilipinoPRC Baguio100% (1)
- G7M-1055-05 - On-Line Visual Inspection Procedures and ChecklistDocument1 pageG7M-1055-05 - On-Line Visual Inspection Procedures and ChecklistMohammad Qureshi100% (1)
- Effective Leadership Theory Cases and Applications 1st Edition Humphrey Test BankDocument9 pagesEffective Leadership Theory Cases and Applications 1st Edition Humphrey Test Bankhillyobsidian8hi42g100% (36)
- Clinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Document555 pagesClinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Dragutin PetrićNo ratings yet
- ORGB 5th Edition Nelson Solutions Manual 1Document44 pagesORGB 5th Edition Nelson Solutions Manual 1shirley100% (52)
- Students Personal Data Sheet FormDocument1 pageStudents Personal Data Sheet FormL 1No ratings yet
- 2 NdresearchpaperDocument5 pages2 Ndresearchpaperapi-356685046No ratings yet
- Shift Manager ResumeDocument2 pagesShift Manager ResumeAbdul NaeemNo ratings yet
- AugustDocument6 pagesAugustchathurika dulanjaliNo ratings yet
- EDocument56 pagesEimee tan100% (3)
- Vitamins Minerals: Composition & Therapeutic UseDocument2 pagesVitamins Minerals: Composition & Therapeutic UseNouman AbbasNo ratings yet
- Overcoming Disordered Eating - 06 - Improving Low Self-EsteemDocument11 pagesOvercoming Disordered Eating - 06 - Improving Low Self-EsteemYesha ShahNo ratings yet
- Operational Management Assignment PDFDocument7 pagesOperational Management Assignment PDFYonas D. EbrenNo ratings yet
- Differences and similarities among the three dopamine receptor partial agonistsDocument10 pagesDifferences and similarities among the three dopamine receptor partial agonistsolivukovic100% (1)
- Annual Record of Homœopathic Literature.1875Document395 pagesAnnual Record of Homœopathic Literature.1875GustavoMarceloDareNo ratings yet
- Understanding Human Subjectivity and IntersubjectivityDocument5 pagesUnderstanding Human Subjectivity and IntersubjectivityKimchiiNo ratings yet
- THE 2020 Online And: Self-Guided Pfa ModulesDocument8 pagesTHE 2020 Online And: Self-Guided Pfa ModulesBurning RoseNo ratings yet
- Exercise 5 Characteristics of Soil ColloidsDocument4 pagesExercise 5 Characteristics of Soil ColloidslexiclesmcgeeNo ratings yet
- Evidence Plan: Prepare/Stake Out Building LinesDocument2 pagesEvidence Plan: Prepare/Stake Out Building LinesJulius Pecasio100% (1)
- Barriers To ListeningDocument2 pagesBarriers To ListeningHammad Ali ShahzadNo ratings yet
- Implant Abutment Emergence Angle and Profile in Relation To Peri Implantitis A Systematic ReviewDocument12 pagesImplant Abutment Emergence Angle and Profile in Relation To Peri Implantitis A Systematic ReviewValentinaNo ratings yet
- SINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsDocument14 pagesSINP International Skilled Workers: Expression of Interest (EOI) Selection ResultsSaquib.MahmoodNo ratings yet