You might also like
- Study Guide PCE Shane Mrsic Toma 2014Document137 pagesStudy Guide PCE Shane Mrsic Toma 2014Nidhi Katyal100% (3)
- Differential Diagnosis MSK PathoDocument13 pagesDifferential Diagnosis MSK PatholizNo ratings yet
- Nursing Care Plan-Herniated Nucleus PulposusDocument3 pagesNursing Care Plan-Herniated Nucleus PulposusJasmin Jacob67% (3)
- Foundations Adult Health Nursing 8th Cooper Test BankDocument15 pagesFoundations Adult Health Nursing 8th Cooper Test BankRaadqqqNo ratings yet
- Cyriax ConceptDocument26 pagesCyriax ConceptMeenakshiputraeashwarprasad MacherlaNo ratings yet
- Orthopedic Surgery NotesDocument3 pagesOrthopedic Surgery NotesJoel Salu100% (1)
- Spine PDFDocument7 pagesSpine PDFDRAHMEDFAHMYORTHOCLINIC100% (1)
- Bedah 2Document204 pagesBedah 2Muhammad Sobri MaulanaNo ratings yet
- Tiss 28Document12 pagesTiss 28Ubaid RahamanNo ratings yet
- Injury NotesDocument15 pagesInjury NotesJaden MusclowNo ratings yet
- Neuro RehabilitationDocument58 pagesNeuro Rehabilitationsyafaat164No ratings yet
- MSK Ncm106lecDocument50 pagesMSK Ncm106lecJASTINE JOY PEREZNo ratings yet
- 3.1 Cervical Spine & TMJDocument5 pages3.1 Cervical Spine & TMJAIREN MARGARET MAGDALENANo ratings yet
- Upper Limb Orthopedics: ManojDocument3 pagesUpper Limb Orthopedics: ManojManoj PakalapatiNo ratings yet
- Ortho. CompDocument51 pagesOrtho. CompSakshi ChoudharyNo ratings yet
- PT3 Postural AnalysisDocument5 pagesPT3 Postural Analysisim. EliasNo ratings yet
- GFHDocument34 pagesGFHaisa mutiaraNo ratings yet
- OsteoarthritisDocument2 pagesOsteoarthritisapi-518311936No ratings yet
- Cancer Epidemiology Pathogenesis Lab/Gross Clinical Features Prognosis/TxDocument7 pagesCancer Epidemiology Pathogenesis Lab/Gross Clinical Features Prognosis/TxCaryn RobertsonNo ratings yet
- Rotator Cuff Tears IhoqkuDocument2 pagesRotator Cuff Tears IhoqkuKeefe TanNo ratings yet
- Orthopaedic!Document15 pagesOrthopaedic!bowelprepcolonNo ratings yet
- Common Health Problems in AdolescentDocument11 pagesCommon Health Problems in Adolescent2BGrp3Plaza, Anna MaeNo ratings yet
- Day 2 Concept MapDocument2 pagesDay 2 Concept Mapkyle frascoNo ratings yet
- ELBOWDocument7 pagesELBOWPhoebe DemegilloNo ratings yet
- Shoulder Dislocation ARSDocument4 pagesShoulder Dislocation ARSBambang Ulan AeiyuNo ratings yet
- Hip Disorders SummaryDocument2 pagesHip Disorders SummarybhnsboshkashNo ratings yet
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- Wrist Injuries (Orthopedics)Document2 pagesWrist Injuries (Orthopedics)Kimmybee GarciaNo ratings yet
- Unlock - (PESERTA) BEDAH 2 - Mantap Februari 2018Document202 pagesUnlock - (PESERTA) BEDAH 2 - Mantap Februari 2018Selvi AristinaNo ratings yet
- Underlying Process Umum AkhirnyaDocument3 pagesUnderlying Process Umum AkhirnyaannyNo ratings yet
- Ortho NotesDocument283 pagesOrtho NotesGaushinee VallimanalanNo ratings yet
- W7 CTSDocument4 pagesW7 CTSStevanie SesiliaNo ratings yet
- OrthopaediDocument87 pagesOrthopaediGalihNo ratings yet
- DegenerativeDiskDisease (HNP) IDocument2 pagesDegenerativeDiskDisease (HNP) Iapi-3822433No ratings yet
- Bedah 2 Batch 3 2018Document87 pagesBedah 2 Batch 3 2018Meiza Ihsan FakhriNo ratings yet
- Final Year SyllabusDocument4 pagesFinal Year SyllabusAanchal SharmaNo ratings yet
- Chapter 36Document3 pagesChapter 36Samantha QuintoNo ratings yet
- Temporomandibular Joint: Structure, Function, Dysfunction and Treatment Chris KeatingDocument34 pagesTemporomandibular Joint: Structure, Function, Dysfunction and Treatment Chris KeatingHichem SeghierNo ratings yet
- Head Neck Spine Conditions SummaryDocument5 pagesHead Neck Spine Conditions SummaryDominic c. CastañedaNo ratings yet
- CA II Prefinal Neuro 1Document4 pagesCA II Prefinal Neuro 1emilyfaye.nebabNo ratings yet
- Bedah Menejemen FrakkturDocument53 pagesBedah Menejemen FrakkturvitaNo ratings yet
- Toxins 10 00018Document27 pagesToxins 10 00018Dana DumitruNo ratings yet
- Back Spine ConditionsDocument2 pagesBack Spine ConditionsNinjaNo ratings yet
- 116A PrelimsDocument6 pages116A PrelimsKimjin MallareNo ratings yet
- Orthopedic FinalDocument858 pagesOrthopedic Finalhashmf180% (10)
- (Mantap) Slide Materi Bedah-2 Batch 3 2018 SalinanDocument200 pages(Mantap) Slide Materi Bedah-2 Batch 3 2018 SalinantikaNo ratings yet
- Dislokasi Catatan Unas Myn Van ZarDocument6 pagesDislokasi Catatan Unas Myn Van ZardewiswahyuNo ratings yet
- Dylan Sciara Catergory 1Document4 pagesDylan Sciara Catergory 1api-508474347No ratings yet
- Mnemonic: Erotica: MGT For FractureDocument6 pagesMnemonic: Erotica: MGT For FractureBianx Flores DosdosNo ratings yet
- Zuku Visual Flashnotes Cruciate ExtendedDocument3 pagesZuku Visual Flashnotes Cruciate ExtendedMargarita BrownNo ratings yet
- Radio - MusculoskeletalDocument20 pagesRadio - MusculoskeletalVon HippoNo ratings yet
- Fracture Dislocation LesionsDocument14 pagesFracture Dislocation LesionsReichelle Reine LisingNo ratings yet
- Mus Culo SkeletalDocument7 pagesMus Culo SkeletalJessica Abella SohNo ratings yet
- Management of Chronic Pain With Interventional TechniqueDocument40 pagesManagement of Chronic Pain With Interventional TechniqueRovika RovikaNo ratings yet
- Spodylolysthes IsDocument70 pagesSpodylolysthes IsshravaniNo ratings yet
- Hip ConditionsDocument2 pagesHip ConditionsseemaNo ratings yet
- Patellofemoral Arthralgia Osteochondritis Dissecans (OCD)Document4 pagesPatellofemoral Arthralgia Osteochondritis Dissecans (OCD)Carlos GonzalesNo ratings yet
- Aging Spine: A Degenerative Cascade: TH STDocument4 pagesAging Spine: A Degenerative Cascade: TH STChristi EspinosaNo ratings yet
- Rheuma (Gout, CPD, Rheumatoid Arthritis, Osteoarthritis)Document2 pagesRheuma (Gout, CPD, Rheumatoid Arthritis, Osteoarthritis)Jezreel Yanah De LeonNo ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
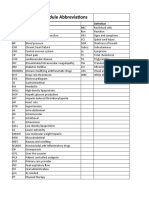
- Pharmacology AbbreviationsDocument1 pagePharmacology AbbreviationsMegan RalstinNo ratings yet
- Patient Case 5 Mr. Chlif-Chronic Heart FailureDocument67 pagesPatient Case 5 Mr. Chlif-Chronic Heart FailureMegan RalstinNo ratings yet
- Ringworm: Morgan Giacobazzi, Megan RalstinDocument8 pagesRingworm: Morgan Giacobazzi, Megan RalstinMegan RalstinNo ratings yet
- Timed Up and Go: Lauren Walters SPT, Megan Ralstin, SPT, Marissa Taylor, SPTDocument14 pagesTimed Up and Go: Lauren Walters SPT, Megan Ralstin, SPT, Marissa Taylor, SPTMegan RalstinNo ratings yet
- Hormone Responses To ExerciseDocument4 pagesHormone Responses To ExerciseMegan RalstinNo ratings yet
- SHCDocument58 pagesSHCElizabethmike100% (4)
- Nursing Care Plan (NCP)Document2 pagesNursing Care Plan (NCP)Aaron ArceNo ratings yet
- PRELIMINARY ACTIVITY of Module 1Document3 pagesPRELIMINARY ACTIVITY of Module 1Casio, Anthony MaryNo ratings yet
- 2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutDocument3 pages2.2 First Aid - Basic First Aid and Resuscitation - Participant HandoutEva ChristinaNo ratings yet
- Covid GuidelinesDocument1 pageCovid Guidelinesapi-509452068No ratings yet
- Bmi Lab Viva QuestionDocument7 pagesBmi Lab Viva QuestionnijafancyNo ratings yet
- Demodex Infestation Requires Immediate, Aggressive Treatment by Doctor, Patient - Primary Care Optometry NewsDocument5 pagesDemodex Infestation Requires Immediate, Aggressive Treatment by Doctor, Patient - Primary Care Optometry NewsΔιονύσης ΦιοραβάντεςNo ratings yet
- Medication - Chart ADHD PDFDocument2 pagesMedication - Chart ADHD PDFaayceeNo ratings yet
- Biographic Data: Nursing Health HistoryDocument14 pagesBiographic Data: Nursing Health HistoryMae Jane AuzaNo ratings yet
- Grade 7 3rd Term English Question 2078Document8 pagesGrade 7 3rd Term English Question 2078Deependra SilwalNo ratings yet
- Rmu Surgery OspesDocument110 pagesRmu Surgery OspesHumna YounisNo ratings yet
- Daftar Sampel ReadyDocument6 pagesDaftar Sampel ReadydindaNo ratings yet
- World Sight Day-Activity Report - 2022-PICO PakistanDocument5 pagesWorld Sight Day-Activity Report - 2022-PICO Pakistanjibran khanNo ratings yet
- What Is High Blood PressureDocument3 pagesWhat Is High Blood PressureShekarNo ratings yet
- Gastro POMDocument63 pagesGastro POMLionell Castillo100% (1)
- WedDocument6 pagesWedPratiwi IkaNo ratings yet
- Mispa Count Plus 1Document2 pagesMispa Count Plus 1Tony DanartoNo ratings yet
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- Body Fluids and Circulation Class 11 Study Notes: BloodDocument7 pagesBody Fluids and Circulation Class 11 Study Notes: BloodTUSHAR DASHNo ratings yet
- Hemolytic Disease of NewbornDocument15 pagesHemolytic Disease of Newborncyphochilus100% (1)
- DuchenneDocument13 pagesDuchennejenika studiesNo ratings yet
- Diane Kazer Loving On Our LymphDocument22 pagesDiane Kazer Loving On Our LymphKátia BárbaraNo ratings yet
- A Comparison of Conventional Tube Test and Gel Technique in Evaluation of Direct Antiglobulin TestDocument5 pagesA Comparison of Conventional Tube Test and Gel Technique in Evaluation of Direct Antiglobulin TestYunita RapaNo ratings yet
- Osteomielitis Akut Edit MeiDocument9 pagesOsteomielitis Akut Edit MeiRaja DarmawanNo ratings yet
- ISC236 Abnormal PsychologyDocument2 pagesISC236 Abnormal PsychologyGregNo ratings yet
- TESTDocument22 pagesTESTjuniati samparaNo ratings yet
- Retic MethodDocument18 pagesRetic MethodFaty DearNo ratings yet
- 37 - Acute Rheumatic FeverDocument1 page37 - Acute Rheumatic FevernasibdinNo ratings yet