You might also like
- Operating Manual FX-7102 PDFDocument140 pagesOperating Manual FX-7102 PDFBoyke Winterberg67% (3)
- Learning Exercise 5.9: To Float or Not To FloatDocument2 pagesLearning Exercise 5.9: To Float or Not To FloatZunnel Cortes100% (2)
- Final Clinical EvaluationDocument3 pagesFinal Clinical Evaluationapi-1850934630% (1)
- N 657 - Advanced Physical Assessment Clinical Decision MakingDocument17 pagesN 657 - Advanced Physical Assessment Clinical Decision Makingapi-267840127No ratings yet
- Mandatory OvertimeDocument6 pagesMandatory Overtimeapi-402775925No ratings yet
- Final EvaluationDocument10 pagesFinal Evaluationapi-338285420No ratings yet
- BSN Learning Plan Senior CapstoneDocument3 pagesBSN Learning Plan Senior Capstoneapi-258684779100% (1)
- Learning Plans GoalsDocument2 pagesLearning Plans Goalsapi-284048628100% (1)
- Nursing Care Plan For Patient With Excessive FluidDocument11 pagesNursing Care Plan For Patient With Excessive FluidTsaabitah AnwarNo ratings yet
- Retrograde PlanetsDocument3 pagesRetrograde Planetsddeepuk100% (1)
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Course SyllabusDocument8 pagesCourse Syllabusapi-320828853No ratings yet
- Major Professional Smart Goals 1Document3 pagesMajor Professional Smart Goals 1api-549749065No ratings yet
- Final Evaluation 3020Document9 pagesFinal Evaluation 3020api-400034813No ratings yet
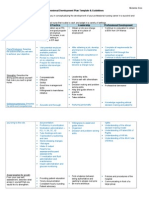
- Report On Progress of Professional Portfoli - MaternityDocument2 pagesReport On Progress of Professional Portfoli - Maternityapi-319323335No ratings yet
- Nursing and Midwifery Board - Questionnaire - Re Entry To Practice Self Assessment Questionnaire - Enrolled NurseDocument10 pagesNursing and Midwifery Board - Questionnaire - Re Entry To Practice Self Assessment Questionnaire - Enrolled NurseZafarsodikNo ratings yet
- N410 SyllabusDocument20 pagesN410 SyllabusTwobucktinNo ratings yet
- Nursing-Associates-Proficiency-Standards 2Document30 pagesNursing-Associates-Proficiency-Standards 2SteveNo ratings yet
- Health Promotion Course Outline 2021Document14 pagesHealth Promotion Course Outline 2021Unufa KhafraNo ratings yet
- QUIZ Critical Thinking in Nursing PracticeDocument16 pagesQUIZ Critical Thinking in Nursing Practicegabrielle magdaraogNo ratings yet
- Needs Assessment For Oral Health Program 1Document16 pagesNeeds Assessment For Oral Health Program 1api-302323771No ratings yet
- Pre-Grad Leadership Experience Reflection Part BDocument5 pagesPre-Grad Leadership Experience Reflection Part Bapi-285304739No ratings yet
- 3020 Learning Plan - SiloDocument4 pages3020 Learning Plan - Siloapi-660581645No ratings yet
- Nursing Code of EthicsDocument2 pagesNursing Code of EthicsClarissa HeatonNo ratings yet
- Critical Thinking Clinical Judgment and Nursing Process - Nurse KeyDocument21 pagesCritical Thinking Clinical Judgment and Nursing Process - Nurse KeyNurul pattyNo ratings yet
- Ch10 - Critical Thinking and Clinical ReasoningDocument31 pagesCh10 - Critical Thinking and Clinical ReasoningVinz TombocNo ratings yet
- Nrs 207 Course ReflectionDocument3 pagesNrs 207 Course Reflectionapi-488741098No ratings yet
- Clinical Nursing JudgementDocument6 pagesClinical Nursing Judgementapi-508132058No ratings yet
- Clinical Nursing JudgmentDocument5 pagesClinical Nursing Judgmentapi-546730313No ratings yet
- Final Reflection DkropaczekDocument3 pagesFinal Reflection Dkropaczekapi-294937204No ratings yet
- PDP KmiuraDocument2 pagesPDP Kmiuraapi-295640482No ratings yet
- Clpna: College of Licensed Practical Nurses of AlbertaDocument28 pagesClpna: College of Licensed Practical Nurses of AlbertaKrista KloseNo ratings yet
- Nursing 350 Reflection PaperDocument7 pagesNursing 350 Reflection Paperapi-2518349340% (1)
- Clinical Goals AssignmentDocument3 pagesClinical Goals Assignmentapi-444846122No ratings yet
- Domain 4 Leadership Management and Team WorkingDocument6 pagesDomain 4 Leadership Management and Team WorkingBryanGavinoSulquianoNo ratings yet
- Clinical Nursing JudgmentDocument5 pagesClinical Nursing Judgmentapi-508051902No ratings yet
- Nurs217 Scholarly AssignmentDocument8 pagesNurs217 Scholarly Assignmentapi-314700318No ratings yet
- Course f2f Inp CPRDocument9 pagesCourse f2f Inp CPRMichelle Gliselle Guinto MallareNo ratings yet
- Portfolio NFDN 2003 2Document3 pagesPortfolio NFDN 2003 2api-306095474No ratings yet
- Nursing Metaparadigm Video TranscriptDocument17 pagesNursing Metaparadigm Video TranscriptAvrianna AveryNo ratings yet
- Infographic Breastfeeding PDFDocument1 pageInfographic Breastfeeding PDFIsmatul MaulahNo ratings yet
- CM1, CU 1, WK 1-Introduction To Leadership and ManagementDocument16 pagesCM1, CU 1, WK 1-Introduction To Leadership and ManagementMichelle Gliselle Guinto MallareNo ratings yet
- NMC Standards For Competence For Registered NursesDocument21 pagesNMC Standards For Competence For Registered NursesAgnieszka WaligóraNo ratings yet
- QsenDocument16 pagesQsenapi-239630424100% (1)
- Godiva Progress ReportDocument2 pagesGodiva Progress Reportapi-323259651No ratings yet
- Nurs 3020 Final EvalDocument9 pagesNurs 3020 Final Evalapi-312968341No ratings yet
- School Nursing SyllabusDocument4 pagesSchool Nursing SyllabusFirenze Fil100% (1)
- Insights Gained Through Interviewing Chief Nurse ExecutiveDocument4 pagesInsights Gained Through Interviewing Chief Nurse Executivecljjch75769901No ratings yet
- Ethics AssignmentDocument3 pagesEthics Assignmenttonydickpatakesseh100% (4)
- NURS222 Clinical Evaluation Tool (CET) Compton Rev 3-14-19Document7 pagesNURS222 Clinical Evaluation Tool (CET) Compton Rev 3-14-19Anie NNo ratings yet
- Test 4 Review CHP 10-14Document5 pagesTest 4 Review CHP 10-14Jacqueline GreerNo ratings yet
- 11 24 19 Nur 403 Final Practice Summary PaperDocument14 pages11 24 19 Nur 403 Final Practice Summary Paperapi-488513754No ratings yet
- EvalDocument3 pagesEvalapi-433857993No ratings yet
- NFDN 2003 Report On Progress of Professional PortfolioDocument2 pagesNFDN 2003 Report On Progress of Professional Portfolioapi-323186111No ratings yet
- FinalDocument4 pagesFinalapi-281066612100% (1)
- Nursing and Midwifery Board Guidelines Supervision Guidelines For Nursing and MidwiferyDocument10 pagesNursing and Midwifery Board Guidelines Supervision Guidelines For Nursing and MidwiferypritamNo ratings yet
- WCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Document29 pagesWCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Joseph MeyerNo ratings yet
- 696 Clinical Learning Agreement - Plan EvaluationDocument16 pages696 Clinical Learning Agreement - Plan Evaluationapi-456551916No ratings yet
- Nursing Competencies. The Artristy of NursingDocument6 pagesNursing Competencies. The Artristy of NursingneoclintNo ratings yet
- The Problem and Its BackgroundDocument9 pagesThe Problem and Its BackgroundPeace Andong PerochoNo ratings yet
- PDP MgooDocument2 pagesPDP Mgooapi-273082149No ratings yet
- Leadership and ManagementDocument2 pagesLeadership and Managementbooda09No ratings yet
- Review of Related Literature and StudiesDocument8 pagesReview of Related Literature and StudiesPrincess Melanie MelendezNo ratings yet
- Ra 11166Document33 pagesRa 11166Princess Melanie MelendezNo ratings yet
- Ra 442Document14 pagesRa 442Princess Melanie MelendezNo ratings yet
- Meet The Awesome Filipino Who Just Won ADocument9 pagesMeet The Awesome Filipino Who Just Won APrincess Melanie MelendezNo ratings yet
- SwotDocument9 pagesSwotPrincess Melanie MelendezNo ratings yet
- Law On Property Required Digested CasesDocument308 pagesLaw On Property Required Digested CasesPrincess Melanie MelendezNo ratings yet
- Key RolesDocument17 pagesKey RolesPrincess Melanie MelendezNo ratings yet
- Ra 7210Document3 pagesRa 7210Princess Melanie MelendezNo ratings yet
- Definition of Decision MakingDocument12 pagesDefinition of Decision MakingPrincess Melanie MelendezNo ratings yet
- What Is Administration in Nursing Service?Document4 pagesWhat Is Administration in Nursing Service?Princess Melanie MelendezNo ratings yet
- Ra 442Document14 pagesRa 442Princess Melanie MelendezNo ratings yet
- Philosophy of Nursing ServiceDocument6 pagesPhilosophy of Nursing ServicePrincess Melanie MelendezNo ratings yet
- Official Gazette of The Republic of The PhilippinesDocument24 pagesOfficial Gazette of The Republic of The PhilippinesPrincess Melanie MelendezNo ratings yet
- Notes On Legal EthicsDocument3 pagesNotes On Legal EthicsPrincess Melanie MelendezNo ratings yet
- ORGANIZATIONDocument36 pagesORGANIZATIONPrincess Melanie MelendezNo ratings yet
- Have A Good Understanding of Full Cycle Recruiting and Solid Knowledge of Labor LegislationDocument2 pagesHave A Good Understanding of Full Cycle Recruiting and Solid Knowledge of Labor LegislationPrincess Melanie MelendezNo ratings yet
- Legal Ethics CasesDocument116 pagesLegal Ethics CasesPrincess Melanie Melendez100% (1)
- Vocabulary:: IELTS Speaking Sample About MusicDocument2 pagesVocabulary:: IELTS Speaking Sample About MusicPrincess Melanie MelendezNo ratings yet
- Advanced Vocabulary:: IELTS Speaking Sample About HealthDocument2 pagesAdvanced Vocabulary:: IELTS Speaking Sample About HealthPrincess Melanie MelendezNo ratings yet
- Search On Leadership and Management On How It Will Apply To Your Position As Head or A Leader in A Certain InstitutionDocument12 pagesSearch On Leadership and Management On How It Will Apply To Your Position As Head or A Leader in A Certain InstitutionPrincess Melanie MelendezNo ratings yet
- Vocabulary:: IELTS Speaking Sample About MusicDocument2 pagesVocabulary:: IELTS Speaking Sample About MusicPrincess Melanie MelendezNo ratings yet
- Advanced Vocabulary:: IELTS Speaking Sample About HealthDocument2 pagesAdvanced Vocabulary:: IELTS Speaking Sample About HealthPrincess Melanie MelendezNo ratings yet
- Modeling and Visualizing Substrata Data With CIVIL 3DDocument21 pagesModeling and Visualizing Substrata Data With CIVIL 3Dg5680No ratings yet
- Steel Railway BridgesDocument161 pagesSteel Railway BridgesMircea Tomus100% (1)
- 71 Bed Bug Information HLDocument1 page71 Bed Bug Information HLMatthew SelfNo ratings yet
- Excavator Solutions Manual PDFDocument8 pagesExcavator Solutions Manual PDFplcNo ratings yet
- Clinical Ocular Toxicology - FraunfelderDocument371 pagesClinical Ocular Toxicology - Fraunfelderelias misael montero ramirez100% (1)
- Semester IIIDocument2 pagesSemester IIIAakarshak NandwaniNo ratings yet
- PWD JE SyllabusDocument4 pagesPWD JE Syllabus323 Aditya DhepeNo ratings yet
- Start UpsDocument6 pagesStart Upsv9991 v9991No ratings yet
- Heritage City Development AND Augmentation Yojana (Hriday) : Kavya Vinay V Noohiya Thasni Snigdha SajeevDocument76 pagesHeritage City Development AND Augmentation Yojana (Hriday) : Kavya Vinay V Noohiya Thasni Snigdha Sajeevkavya vinayNo ratings yet
- GPS 175 GNC 355 GNX 375: Pilot's GuideDocument276 pagesGPS 175 GNC 355 GNX 375: Pilot's GuideJanaka GamageNo ratings yet
- My Running Analytics: Distance and Pace Over TimeDocument12 pagesMy Running Analytics: Distance and Pace Over TimeJayanthi JaganNo ratings yet
- MBS2250 Heavy-Duty Pressure Transmitter: Features Principle of OperationDocument2 pagesMBS2250 Heavy-Duty Pressure Transmitter: Features Principle of Operationjose salvadorNo ratings yet
- Geometry Section 1 1Document9 pagesGeometry Section 1 1api-262621710No ratings yet
- Sci 6 DLL Week 6 q4Document11 pagesSci 6 DLL Week 6 q4Christinne Anne LupoNo ratings yet
- Industrial Scientific - 2021 - Americas - Catalog - ENDocument44 pagesIndustrial Scientific - 2021 - Americas - Catalog - ENcomprasaemarineNo ratings yet
- Outline of Tibetan MedicineDocument13 pagesOutline of Tibetan MedicineTaliah BassarabaNo ratings yet
- Alloy Steel Socket-Head Cap Screws: Standard Specification ForDocument7 pagesAlloy Steel Socket-Head Cap Screws: Standard Specification ForMARCELO DOS SANTOS BARRETOSNo ratings yet
- Durabuilt Vs NLRCDocument1 pageDurabuilt Vs NLRChello_hoarder100% (1)
- Lecture 9 NotchesDocument25 pagesLecture 9 NotchesCh ZainNo ratings yet
- SSD TC 3 7 Prehistory and Archaeology StudentDocument25 pagesSSD TC 3 7 Prehistory and Archaeology StudentyokirendrapriyantokoNo ratings yet
- Chem Notes Chapter 10Document68 pagesChem Notes Chapter 10johnNo ratings yet
- Periodontal Ligament: Teeth Maxillary MandibularDocument7 pagesPeriodontal Ligament: Teeth Maxillary MandibularAsfoor gake1No ratings yet
- Nick Herbert Dossier: Ong's HatDocument4 pagesNick Herbert Dossier: Ong's HatJoseph Matheny0% (1)
- Boxing Bag Gloves Price LIstDocument11 pagesBoxing Bag Gloves Price LIstIresha UdayangiNo ratings yet
- GATRONOVA Internship ReportDocument34 pagesGATRONOVA Internship ReportAbdulmunaf SheikhNo ratings yet
- CV - Tansha Muwarwan TidanDocument2 pagesCV - Tansha Muwarwan TidantanshamuwarwanNo ratings yet
- What Is Telecommunication TransmissionDocument26 pagesWhat Is Telecommunication TransmissionmyotezaNo ratings yet