You might also like
- Antibiotic Study Cheat Sheet August 2019Document1 pageAntibiotic Study Cheat Sheet August 2019Ryan TurnerNo ratings yet
- Bacteriology PDFDocument49 pagesBacteriology PDFPearl Medina100% (2)
- Emergency Patient Care GuideDocument10 pagesEmergency Patient Care GuideRyan Turner100% (1)
- Micro I ReviewDocument15 pagesMicro I ReviewEmilee Tu100% (1)
- Bacte Notes #1 - Introduction To BacteriologyDocument14 pagesBacte Notes #1 - Introduction To BacteriologyMartin ClydeNo ratings yet
- High Yield - Bacteriology ChartsDocument9 pagesHigh Yield - Bacteriology ChartsAmirsalar EslamiNo ratings yet
- Microbiology Made Ludicrously SimplerDocument59 pagesMicrobiology Made Ludicrously SimplerLaylee Clare100% (2)
- Robbins Questions Chp1-10Document28 pagesRobbins Questions Chp1-10verbatimmt100% (1)
- S. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusDocument14 pagesS. Aureus, Cons: S.Epidermidis, Cons: S.SaprophyticusMugiNo ratings yet
- Parasitology Table: ProtozoaDocument10 pagesParasitology Table: ProtozoaKate Alyssa CatonNo ratings yet
- Anaerobic BacteriaDocument16 pagesAnaerobic BacteriaPriti Go0% (1)
- Zanki (Complete) + R/medicalschoolanki Microbiology ErrataDocument70 pagesZanki (Complete) + R/medicalschoolanki Microbiology ErrataedNo ratings yet
- Systemic BacteriologyDocument495 pagesSystemic BacteriologyAkash KaranwalNo ratings yet
- Structure and Classification of Bacteria: Morpho DifferencesDocument8 pagesStructure and Classification of Bacteria: Morpho DifferencesJaz CNo ratings yet
- Concise SEO-Optimized Title for Clotting DocumentDocument3 pagesConcise SEO-Optimized Title for Clotting DocumentRyan TurnerNo ratings yet
- Prelim ExamDocument17 pagesPrelim Examsaci PTNo ratings yet
- Microbiology Special Report: General Template for Characterizing Important MicrobesDocument68 pagesMicrobiology Special Report: General Template for Characterizing Important MicrobesrefuapalackyNo ratings yet
- Periodontal Disease Mombelli PDFDocument191 pagesPeriodontal Disease Mombelli PDFApeksha GhaiNo ratings yet
- BiochemDocument7 pagesBiochemRyan TurnerNo ratings yet
- BiochemDocument7 pagesBiochemRyan TurnerNo ratings yet
- ImmunizationDocument30 pagesImmunizationAhmed Ali100% (1)
- DRUG STUDY CefuroximeDocument2 pagesDRUG STUDY CefuroximeLyana Stark92% (39)
- Immunology & Serology ReviewDocument4 pagesImmunology & Serology Reviewmaria email86% (7)
- FULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF EbookDocument41 pagesFULL Download Ebook PDF Fundamentals of Human Neuropsychology 7th Edition PDF Ebookjennifer.lawver532100% (42)
- IDNT TerminologyDocument6 pagesIDNT TerminologyLaura Pérez RamosNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- Step 3: Sample Test QuestionsDocument81 pagesStep 3: Sample Test QuestionsThaer HafiNo ratings yet
- StaphDocument6 pagesStaphpekibelssNo ratings yet
- USMLE Flashcards: Microbiology and Immunology - Side by SideDocument196 pagesUSMLE Flashcards: Microbiology and Immunology - Side by SideMedSchoolStuff0% (1)
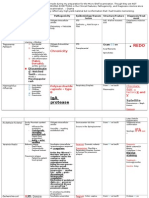
- Toxicology g5 Sua Outline Final 1Document39 pagesToxicology g5 Sua Outline Final 1Giang Thị Thanh HươngNo ratings yet
- Microbial Toxins PDFDocument11 pagesMicrobial Toxins PDFAnonymous OPix6Tyk5INo ratings yet
- 01 - DiarrheaDocument36 pages01 - DiarrheafrizkapfNo ratings yet
- Lecture 2 General BacteriologyDocument32 pagesLecture 2 General BacteriologyAyat MostafaNo ratings yet
- Gram-Positive Cocci Classification and Pathogenic SpeciesDocument11 pagesGram-Positive Cocci Classification and Pathogenic SpeciesJo Marchianne PigarNo ratings yet
- Mix of Micro Mne MonDocument21 pagesMix of Micro Mne MonallybishNo ratings yet
- Bacte Midterm (Walang Pictures)Document21 pagesBacte Midterm (Walang Pictures)AL-HUSSEIN NAWABNo ratings yet
- Chart - Vector BorneDocument1 pageChart - Vector BorneRedNo ratings yet
- Anaerobic Bacteria: Fig. 1 Different Categories of Bacteria - On The Basis of Oxygen RequirementsDocument17 pagesAnaerobic Bacteria: Fig. 1 Different Categories of Bacteria - On The Basis of Oxygen RequirementsVishaliniNo ratings yet
- Bacterial PathogenesisDocument36 pagesBacterial Pathogenesisapi-19969058100% (3)
- Bacterial ToxinsDocument20 pagesBacterial ToxinsYogiabrorNo ratings yet
- Bacteriology by Dhshan Hassan DhshanDocument48 pagesBacteriology by Dhshan Hassan Dhshanعلي الكوافي100% (1)
- Bacte Midterm Di TaposDocument9 pagesBacte Midterm Di TaposAL-HUSSEIN NAWABNo ratings yet
- Parasitology Table ProtozoaDocument10 pagesParasitology Table ProtozoaMae Rose Charlene MendozaNo ratings yet
- Division of Tropical Medicine and Infectious Diseases at Gatot Soebroto Central Army HospitalDocument63 pagesDivision of Tropical Medicine and Infectious Diseases at Gatot Soebroto Central Army HospitalAggiFitiyaningsihNo ratings yet
- Bacterial Toxin: DR Ance Roslina, M.Kes Bagian Mikrobiologi FK - Umsu 2019Document35 pagesBacterial Toxin: DR Ance Roslina, M.Kes Bagian Mikrobiologi FK - Umsu 2019atikaNo ratings yet
- AEROBIC, GRAM POS BACILLI NON-SPORE FORMER (Nahaeminrmt)Document7 pagesAEROBIC, GRAM POS BACILLI NON-SPORE FORMER (Nahaeminrmt)Rach ReyesNo ratings yet
- StaphylococcusDocument13 pagesStaphylococcusZeth MoturiNo ratings yet
- ACE Edit 1 - 2Document142 pagesACE Edit 1 - 2Carly DyaNo ratings yet
- Chapter 41 - 42 - Anaerobic OrganimsDocument4 pagesChapter 41 - 42 - Anaerobic OrganimsKoarie Frae ZuleNo ratings yet
- Staphylococcus aureus: A Clinically Significant PathogenDocument40 pagesStaphylococcus aureus: A Clinically Significant PathogenMarissa Terrado SorianoNo ratings yet
- Bacteria 3Document45 pagesBacteria 3jessicaNo ratings yet
- RevalidaDocument5 pagesRevalidaHawkins FletcherNo ratings yet
- Acid (Acts As Antigenic Determinant-Impo For Serologic ID)Document5 pagesAcid (Acts As Antigenic Determinant-Impo For Serologic ID)qwertier2No ratings yet
- Bacterial ToxinsDocument4 pagesBacterial ToxinsAnonymous kPaB8WvNo ratings yet
- Immunity To Extracellular BacteriaDocument23 pagesImmunity To Extracellular BacteriaNoor NawawraNo ratings yet
- Lecture 3 Bacteria G Biology ES1Document27 pagesLecture 3 Bacteria G Biology ES1nourhan yousefNo ratings yet
- BACTERIAL TOXINS: TARGETS AND MECHANISMSDocument20 pagesBACTERIAL TOXINS: TARGETS AND MECHANISMSYogiabrorNo ratings yet
- Day 1 BacteriaDocument251 pagesDay 1 BacteriaLisa NetherlandNo ratings yet
- Bacteria With Toxin-Dr AnceDocument32 pagesBacteria With Toxin-Dr AnceSuita Allemina Gloria SitepuNo ratings yet
- Reviewer - Bacteriology FINALS - ANGELES, ANGELICDocument38 pagesReviewer - Bacteriology FINALS - ANGELES, ANGELICAngelic AngelesNo ratings yet
- Pediatric Bacterial InfectiousDocument39 pagesPediatric Bacterial InfectiousGopu SaitejaNo ratings yet
- Micro paraDocument2 pagesMicro parafeminaNo ratings yet
- Peptostreptococcus Veillonella Megasphaera Acidaminococcus: DescriptionDocument1 pagePeptostreptococcus Veillonella Megasphaera Acidaminococcus: Descriptionhuyenthanh1807No ratings yet
- Wuolah Free Bacteria TableDocument11 pagesWuolah Free Bacteria TableELENA FERNANDEZNo ratings yet
- GAS GANGRENE IN SOFT TISSUEDocument28 pagesGAS GANGRENE IN SOFT TISSUERana Muhammad AshfaqNo ratings yet
- Gram Stain vs Acid Fast Stain ComparisonDocument4 pagesGram Stain vs Acid Fast Stain ComparisonNarcisa Romano AplodNo ratings yet
- Protozoa Revision Toxoplasma GondiiDocument2 pagesProtozoa Revision Toxoplasma GondiipixiedustNo ratings yet
- Microbiology Mock Boards 1 RatioDocument4 pagesMicrobiology Mock Boards 1 RatioMarie LlanesNo ratings yet
- TransDocument6 pagesTransZllison Mae Teodoro MangabatNo ratings yet
- MBIO 4823 Final Review IIIDocument1 pageMBIO 4823 Final Review IIIuberjunk426801100% (1)
- Parasitic - Toxic SummaryDocument9 pagesParasitic - Toxic Summaryakilesh hardowarNo ratings yet
- Clinical Terms and Definitions for Medical StudentsDocument136 pagesClinical Terms and Definitions for Medical StudentsrubyNo ratings yet
- Lipid MediatorsFrom EverandLipid MediatorsFiona M. CunninghamNo ratings yet
- Concentration Gradient: Cell Physiology 1 of 5Document5 pagesConcentration Gradient: Cell Physiology 1 of 5Ryan TurnerNo ratings yet
- Connective TissueDocument2 pagesConnective TissueRyan TurnerNo ratings yet
- MC Tumors and Cancers of Various OrgansDocument12 pagesMC Tumors and Cancers of Various OrgansRyan TurnerNo ratings yet
- Concentration Gradient: Cell Physiology 1 of 5Document5 pagesConcentration Gradient: Cell Physiology 1 of 5Ryan TurnerNo ratings yet
- Connective TissueDocument2 pagesConnective TissueRyan TurnerNo ratings yet
- Trigger: Infection That Causes MyositisDocument4 pagesTrigger: Infection That Causes MyositisRyan TurnerNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- NEW UMHS Clinical Student HandbookDocument25 pagesNEW UMHS Clinical Student HandbookRyan TurnerNo ratings yet
- Content Step3Document28 pagesContent Step3coralkaomaNo ratings yet
- Herpes Zoster in Hospitalized AdultsDocument11 pagesHerpes Zoster in Hospitalized AdultsagusNo ratings yet
- Current Forensic Assessment TechniquesDocument23 pagesCurrent Forensic Assessment TechniquesDesmond DraughonNo ratings yet
- Liu 2017-Herbal Medicine For The Treatment of ObesityDocument17 pagesLiu 2017-Herbal Medicine For The Treatment of ObesityMas NuriNo ratings yet
- Herbs CampDocument42 pagesHerbs CampJohn JohnNo ratings yet
- PDFDocument6 pagesPDFKoko “urya” No NekoNo ratings yet
- CIL EXE Leave Rule - UpdatedDocument4 pagesCIL EXE Leave Rule - Updatedparmod kumarNo ratings yet
- Overview of Sudden Cardiac Arrest and Sudden Cardiac Death - UpToDateDocument23 pagesOverview of Sudden Cardiac Arrest and Sudden Cardiac Death - UpToDateSamuel MartinezNo ratings yet
- Neonatal assessment essentialsDocument91 pagesNeonatal assessment essentialsSHAFIQNo ratings yet
- SM Lazo Medical Clinic PEME Schedule ConfirmationDocument1 pageSM Lazo Medical Clinic PEME Schedule ConfirmationMaximoNo ratings yet
- Round Table 2013-07-13Document52 pagesRound Table 2013-07-13Cokorda Istri Devi LarayanthiNo ratings yet
- Nursing Care Plan of The NewbornDocument4 pagesNursing Care Plan of The Newbornbowki namoNo ratings yet
- PD Week 5Document7 pagesPD Week 5DAPHNEE MAE AGUDONGNo ratings yet
- Evidence Based Ophthalmology: Noel D. Atienza, MD, MSCDocument59 pagesEvidence Based Ophthalmology: Noel D. Atienza, MD, MSCJanBarlaanNo ratings yet
- FinalDocument66 pagesFinalRakshith gowdaNo ratings yet
- Test Report:: Patient Name:Mr Bahu Anil Kumar Sahu Patient IDDocument1 pageTest Report:: Patient Name:Mr Bahu Anil Kumar Sahu Patient IDANILNo ratings yet
- COVID-19 Prevention and Control Literature ReviewDocument2 pagesCOVID-19 Prevention and Control Literature ReviewericNo ratings yet
- Patient Medical Records ListDocument20 pagesPatient Medical Records ListStella Putri WandaNo ratings yet
- Lecture 5.urine AnalysisDocument33 pagesLecture 5.urine AnalysisRaja Iqbal Mulya HarahapNo ratings yet
- Pernicious Anaemia and B12 2020Document42 pagesPernicious Anaemia and B12 2020viraaj pawarNo ratings yet
- Sexlinkedgenes DemoDocument57 pagesSexlinkedgenes DemopearlNo ratings yet
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonNo ratings yet
- Disaster Management-Group 2Document90 pagesDisaster Management-Group 2Kavitha ArjunNo ratings yet
- Respiratory Disease Anatomy and Phys Sheridan CollegeDocument7 pagesRespiratory Disease Anatomy and Phys Sheridan CollegeAudrey AndinoNo ratings yet
- Group 3 - Week 5 (Nur192)Document10 pagesGroup 3 - Week 5 (Nur192)Cristine JanolinoNo ratings yet