You might also like
- Etech 1ST QTR BDocument4 pagesEtech 1ST QTR BJohnArgielLaurenteVictorNo ratings yet
- Work ImmersionDocument28 pagesWork ImmersionBlue Lions50% (4)
- Immersion Competencies For HUMSSDocument1 pageImmersion Competencies For HUMSSleah n gersana100% (2)
- 2 08 2018 Work Immersion Appraisal FormDocument5 pages2 08 2018 Work Immersion Appraisal FormRachel Barote Hernando Paradero100% (2)
- Work Immersion Rules and RegulationsDocument34 pagesWork Immersion Rules and RegulationsJoiemmy Sumedca Bawengan Gayudan57% (14)
- Cpar 1ST QTRDocument4 pagesCpar 1ST QTRJohnArgielLaurenteVictor100% (1)
- Etech 1ST QTRDocument4 pagesEtech 1ST QTRJohnArgielLaurenteVictor100% (4)
- Work Immersion Performance Appraisal - FINALDocument3 pagesWork Immersion Performance Appraisal - FINALBernadette Aycocho100% (5)
- Pre Immersion+OrientationDocument23 pagesPre Immersion+OrientationFrancine Mae HuyaNo ratings yet
- Las English g10 Melc 5 VFDocument9 pagesLas English g10 Melc 5 VFJohnArgielLaurenteVictorNo ratings yet
- Work Immersion AppraisalDocument4 pagesWork Immersion AppraisalRustan Lacanilao80% (15)
- WORK IMMERSION PORTFOLIO Based On DepEdYEEjessDocument55 pagesWORK IMMERSION PORTFOLIO Based On DepEdYEEjessJasmine DiazNo ratings yet
- Work Immersion Agreement and Liability WaiverDocument1 pageWork Immersion Agreement and Liability WaiverLyn VallesNo ratings yet
- Depedshs Work Immersion MELCSDocument5 pagesDepedshs Work Immersion MELCSChristina Legaspi100% (5)
- Immersion Student DTRDocument1 pageImmersion Student DTRVirgilio Rosario Biagtan83% (6)
- ANNEX C: Prescribed Template For The List of Task/Activities To Be Done During Work ImmersionDocument2 pagesANNEX C: Prescribed Template For The List of Task/Activities To Be Done During Work Immersioncelyn laroya67% (6)
- Letter For Work ImmersionDocument16 pagesLetter For Work ImmersionMaestro Mertz100% (1)
- Action Plan For Work ImmersionDocument3 pagesAction Plan For Work ImmersionJoe Jayson Caletena100% (5)
- Work Immersion Training Plan OrlanDocument2 pagesWork Immersion Training Plan OrlanJane-Marie Parba Banga75% (4)
- LAS-English-G10-MELC 1-4 VFDocument56 pagesLAS-English-G10-MELC 1-4 VFJohnArgielLaurenteVictorNo ratings yet
- Letter of Partnership Work Immersion.Document4 pagesLetter of Partnership Work Immersion.danicaNo ratings yet
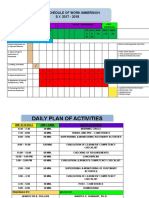
- Work Immersion Schedule: Department of EducationDocument2 pagesWork Immersion Schedule: Department of EducationJohnArgielLaurenteVictorNo ratings yet
- Work Immersion: GRADE 12 General Academic Strand (GAS) Work Immersion ManualDocument23 pagesWork Immersion: GRADE 12 General Academic Strand (GAS) Work Immersion ManualAbegail A. Alangue-Calimag100% (9)
- Immersion Manual Portfolio Lrmds FinalDocument92 pagesImmersion Manual Portfolio Lrmds FinalRYAN PILUETA100% (2)
- LEED GA Exam Questions Set 2Document22 pagesLEED GA Exam Questions Set 2CEG BangladeshNo ratings yet
- Work Immersion - Training Agreement and Liability WaiverDocument2 pagesWork Immersion - Training Agreement and Liability WaiverSteve Marville Aguinaldo50% (2)
- Activity-Design-for-work ImmersionDocument4 pagesActivity-Design-for-work ImmersionKyle Aureo Andagan Ramiso75% (4)
- Ucsp 1ST QTRDocument31 pagesUcsp 1ST QTRJohnArgielLaurenteVictorNo ratings yet
- Humss Work Immersion ProgramDocument9 pagesHumss Work Immersion ProgramCarl Golingay Jun93% (15)
- Work Immersion Orientation PPT EditedDocument9 pagesWork Immersion Orientation PPT EditedSheryl100% (2)
- Work Immersion Evaluation FormDocument2 pagesWork Immersion Evaluation FormRegina Palafox Tolosa67% (3)
- Work Immersion Evaluation FormDocument1 pageWork Immersion Evaluation FormPrince Dkalm Polished86% (7)
- Work Immersion Portfolio StudentsDocument18 pagesWork Immersion Portfolio StudentsJubylyn AficialNo ratings yet
- Work Immersion Action PlanDocument4 pagesWork Immersion Action Planhazel_rivera67% (3)
- Work Immersion ActivitiesDocument4 pagesWork Immersion ActivitiesLeigh Shane92% (13)
- Memorandum of Agreement For Work Immersion ProgramDocument5 pagesMemorandum of Agreement For Work Immersion ProgramAllan Palma Gil100% (1)
- Confidentiality Agreement FormDocument2 pagesConfidentiality Agreement FormHanz Albrech Abella100% (1)
- Work - Immersion - Students ProfileDocument1 pageWork - Immersion - Students ProfileAldrinBalita100% (2)
- Technical Data FN Evolys 762Document1 pageTechnical Data FN Evolys 762Zedney ZedneyNo ratings yet
- Portfolio FinalDocument33 pagesPortfolio FinalAisha Erica S. Dumaan IINo ratings yet
- Las English g10 Melc 1Document12 pagesLas English g10 Melc 1JohnArgielLaurenteVictor100% (1)
- Pre-Immersion Orientation: Bulacan Polytechnic CollegeDocument39 pagesPre-Immersion Orientation: Bulacan Polytechnic CollegeEL Fuentes100% (6)
- Oracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFDocument486 pagesOracle Database 12C SQL WORKSHOP 2 - Student Guide Volume 2 PDFenrrichel0% (1)
- Curs Chimie 1Document79 pagesCurs Chimie 1Onyx Tear100% (1)
- Work Immersion OrientationDocument30 pagesWork Immersion Orientationvida adviento82% (78)
- 1st Quarter Summative Test in WORK IMMERSIONDocument4 pages1st Quarter Summative Test in WORK IMMERSIONDorgieFelicianoViray100% (1)
- Las English g10 Melc 6 VFDocument9 pagesLas English g10 Melc 6 VFJohnArgielLaurenteVictorNo ratings yet
- Updated Shs Work Immersion PortfolioDocument47 pagesUpdated Shs Work Immersion PortfolioAica Rose Dela Cruz100% (1)
- Pre Work Immersion Evaluation FormDocument2 pagesPre Work Immersion Evaluation FormJohnArgielLaurenteVictorNo ratings yet
- Pre Work Immersion Evaluation FormDocument2 pagesPre Work Immersion Evaluation FormJohnArgielLaurenteVictorNo ratings yet
- Work Immersion Portfolio Scoring RubricDocument2 pagesWork Immersion Portfolio Scoring RubricNosaj Hermosilla100% (5)
- Work Immersion CertificateDocument1 pageWork Immersion CertificateARIANE I. LAGATIC100% (6)
- Work Immersion Evaluation FormDocument2 pagesWork Immersion Evaluation FormMaestro Mertz92% (13)
- Work ImmersionDocument40 pagesWork ImmersionRuben Ligutan100% (9)
- Universidad de Sta. Isabel Pili Campus: Work ImmersionDocument2 pagesUniversidad de Sta. Isabel Pili Campus: Work ImmersionLey Park75% (4)
- Work Immersion Performance EvaluationDocument4 pagesWork Immersion Performance EvaluationAko Si Anna80% (5)
- Work Immersion Evaluation FormDocument2 pagesWork Immersion Evaluation Formkent100% (9)
- Requirements For Work ImmersionDocument2 pagesRequirements For Work ImmersionHerbert LaluzNo ratings yet
- Work Immersion Module and Worksheet Week 6Document4 pagesWork Immersion Module and Worksheet Week 6Randy Reyes75% (4)
- Accomplishment Report For Pre ImmersionDocument5 pagesAccomplishment Report For Pre ImmersionJovito Digman Jimenez93% (14)
- Letter of AcceptanceDocument2 pagesLetter of AcceptanceEi100% (6)
- Work Immersion DLPDocument24 pagesWork Immersion DLPCzarrine Junio89% (9)
- Work Immersion (Waiver)Document27 pagesWork Immersion (Waiver)Camille ManlongatNo ratings yet
- Affidavit of ConfirmationDocument1 pageAffidavit of ConfirmationJohnArgielLaurenteVictor0% (1)
- Lesson 4: The Rise of Asian EmpiresDocument44 pagesLesson 4: The Rise of Asian EmpiresJohnArgielLaurenteVictorNo ratings yet
- Work Immersion PortfolioDocument1 pageWork Immersion PortfolioLeo Loven Lumacang75% (24)
- IN Work Immersion: Grade 12 Senior High School Immersion ManualDocument28 pagesIN Work Immersion: Grade 12 Senior High School Immersion Manualsmpaderna08100% (1)
- Work Immersion Progress Monitoring ToolDocument4 pagesWork Immersion Progress Monitoring Tooldorina P.Rodriguez50% (2)
- Work Immersion Portfolio RubricDocument1 pageWork Immersion Portfolio RubricDeb Lub100% (5)
- Moa For Work Immersion 2023Document18 pagesMoa For Work Immersion 2023Christina Manguiob Escasinas100% (2)
- Work Immersion Endorsement LetterDocument1 pageWork Immersion Endorsement LetterBrian Reyes Gangca100% (5)
- Work Immersion 2019 Letter To LGUDocument3 pagesWork Immersion 2019 Letter To LGUBry Esguerra0% (1)
- Work Immersion Orientation and Pre-Immersion Activity TVLDocument3 pagesWork Immersion Orientation and Pre-Immersion Activity TVLGlenzchie TaguibaoNo ratings yet
- Orientation: Pre-Immersion - Grade 12Document3 pagesOrientation: Pre-Immersion - Grade 12Alex Abonales Dumandan100% (3)
- Work Immersion Monitoring HousekeepingDocument16 pagesWork Immersion Monitoring HousekeepingG-one Paisones100% (2)
- Work Immersion - Format and Guidelines For PortfolioDocument18 pagesWork Immersion - Format and Guidelines For PortfolioRodrick Sonajo Ramos75% (4)
- Iphp 1ST QTRDocument30 pagesIphp 1ST QTRJohnArgielLaurenteVictorNo ratings yet
- Iphp 1st QTR StudentDocument10 pagesIphp 1st QTR StudentJohnArgielLaurenteVictorNo ratings yet
- Ucsp 1st QTR StudentDocument15 pagesUcsp 1st QTR StudentJohnArgielLaurenteVictorNo ratings yet
- Individual Learning Monitoring PlanDocument2 pagesIndividual Learning Monitoring PlanJohnArgielLaurenteVictorNo ratings yet
- Junior High School Master Class Program S.Y. 2021-2022: Colonia Divina Integrated SchoolDocument3 pagesJunior High School Master Class Program S.Y. 2021-2022: Colonia Divina Integrated SchoolJohnArgielLaurenteVictorNo ratings yet
- Master Class Program 2021-2022 - 1ST SEMESTERDocument10 pagesMaster Class Program 2021-2022 - 1ST SEMESTERJohnArgielLaurenteVictorNo ratings yet
- Weekly Home Learning Plan: Department of EducationDocument2 pagesWeekly Home Learning Plan: Department of EducationJohnArgielLaurenteVictorNo ratings yet
- NOSP FormDocument4 pagesNOSP FormJohnArgielLaurenteVictorNo ratings yet
- Latest Application Letter May 6 2019Document2 pagesLatest Application Letter May 6 2019JohnArgielLaurenteVictorNo ratings yet
- Introduction To The Philosophy of The Human Person (Iphp)Document1 pageIntroduction To The Philosophy of The Human Person (Iphp)JohnArgielLaurenteVictorNo ratings yet
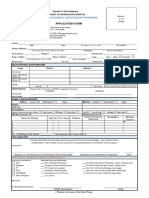
- Application For Vendor AccreditationDocument3 pagesApplication For Vendor AccreditationJohnArgielLaurenteVictorNo ratings yet
- Customer Visit Form & Daiy Transportation DetailsDocument2 pagesCustomer Visit Form & Daiy Transportation DetailsJohnArgielLaurenteVictorNo ratings yet
- The Bullying of Leni RobredoDocument3 pagesThe Bullying of Leni RobredoJohnArgielLaurenteVictorNo ratings yet
- CH Mach II and Mach III Joystick ManualDocument4 pagesCH Mach II and Mach III Joystick Manualucb51525354No ratings yet
- (B) Superposition TheoremDocument4 pages(B) Superposition TheoremMuhammad AbdullahNo ratings yet
- Software Development ProcessDocument16 pagesSoftware Development ProcessSri WulanNo ratings yet
- Annex 1Document23 pagesAnnex 1Richu PaliNo ratings yet
- Đề Thi Thử Thptqg Môn Tiếng AnhDocument11 pagesĐề Thi Thử Thptqg Môn Tiếng AnhnguyenngocquynhchiNo ratings yet
- BSC Iiyr IV Sem Dbms Total NotesDocument110 pagesBSC Iiyr IV Sem Dbms Total NotesVistasNo ratings yet
- Communique - March, 2022Document13 pagesCommunique - March, 2022Ayush RajNo ratings yet
- Law On Partnership - Chapter 1 by DomingoDocument11 pagesLaw On Partnership - Chapter 1 by Domingojhoana morenoNo ratings yet
- 616 Roots Ram Whispair Pressure Performance Curve-2Document1 page616 Roots Ram Whispair Pressure Performance Curve-2Mike LongstockNo ratings yet
- Becoming A Cisco Select Certified Partner-Step by Step GuideDocument7 pagesBecoming A Cisco Select Certified Partner-Step by Step Guidemwaseemno181No ratings yet
- REWP (Core) WORKSHOP GTUDocument8 pagesREWP (Core) WORKSHOP GTUjigarNo ratings yet
- Case Study On BoeingDocument12 pagesCase Study On BoeingshahraashidNo ratings yet
- 10october2020 FriendsNewsDocument4 pages10october2020 FriendsNewspatloubarNo ratings yet
- Blood Banking: By: Anie Jan K. SegoviaDocument19 pagesBlood Banking: By: Anie Jan K. SegoviaArshie08No ratings yet
- Subject: Data Structures Topic: QueueDocument32 pagesSubject: Data Structures Topic: QueueRahna RwpcNo ratings yet
- Eternal Distribution BookDocument107 pagesEternal Distribution BookShappan Abd AllhaNo ratings yet
- Recruitment of AdvisiorDocument66 pagesRecruitment of AdvisiorSamuel DavisNo ratings yet
- Wallstreetjournal 20180919 TheWallStreetJournal-compressedDocument46 pagesWallstreetjournal 20180919 TheWallStreetJournal-compressedAnonymous G0r4iXNo ratings yet
- 10.2 Function Algebra Practice-1 PDFDocument5 pages10.2 Function Algebra Practice-1 PDFYlliw Mercado AredinNo ratings yet
- JabseDocument10 pagesJabseAlison HarperNo ratings yet
- Computer ManualDocument33 pagesComputer ManualZoran KovacevicNo ratings yet
- Annex A - Grant Application FormDocument46 pagesAnnex A - Grant Application FormtijanagruNo ratings yet
- CAPE Management of Business 2018 U2 P2Document13 pagesCAPE Management of Business 2018 U2 P2Unknown userNo ratings yet
- Irctcs E-Ticketing Service Electronic Reservation Slip (Personal User)Document2 pagesIrctcs E-Ticketing Service Electronic Reservation Slip (Personal User)prateekNo ratings yet
- Slawomir Mrozek Lolo FactsheetDocument3 pagesSlawomir Mrozek Lolo Factsheetolaprz24No ratings yet
- MA1 First Test UpdatedDocument14 pagesMA1 First Test UpdatedHammad KhanNo ratings yet