You might also like
- This Study Resource WasDocument6 pagesThis Study Resource WasReyna Mee AhiyasNo ratings yet
- DU UTI Stage 1 Hypertension Case - Analysis FinalDocument87 pagesDU UTI Stage 1 Hypertension Case - Analysis FinalReyna Mee AhiyasNo ratings yet
- Cardiac Catheterization and MonitoringDocument25 pagesCardiac Catheterization and MonitoringReyna Mee AhiyasNo ratings yet
- Case Study GuidelinesDocument1 pageCase Study GuidelinesReyna Mee AhiyasNo ratings yet
- Table 1. Shows The VITAL SIGNS During AdmissionDocument14 pagesTable 1. Shows The VITAL SIGNS During AdmissionReyna Mee AhiyasNo ratings yet
- The Family With A Toddler ToddlerDocument5 pagesThe Family With A Toddler ToddlerReyna Mee AhiyasNo ratings yet
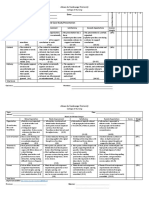
- Team Leader Grading Scheme Case StudyDocument3 pagesTeam Leader Grading Scheme Case StudyReyna Mee AhiyasNo ratings yet
- NCM 118 RLE Case Analysis No.2Document4 pagesNCM 118 RLE Case Analysis No.2Reyna Mee AhiyasNo ratings yet
- Ateneo de Zamboanga University: Deliverables (ALT#1) Learning Objectives: 1. 2. 3Document3 pagesAteneo de Zamboanga University: Deliverables (ALT#1) Learning Objectives: 1. 2. 3Reyna Mee AhiyasNo ratings yet
- Rubric For Oral and Written Case Study PresentationDocument2 pagesRubric For Oral and Written Case Study PresentationReyna Mee AhiyasNo ratings yet
- Nutritional AssessmentDocument6 pagesNutritional AssessmentReyna Mee AhiyasNo ratings yet
- Performing Urethral Urinary CatheterizationDocument4 pagesPerforming Urethral Urinary CatheterizationReyna Mee AhiyasNo ratings yet
- Uncontrolled HypertensionDocument3 pagesUncontrolled HypertensionReyna Mee AhiyasNo ratings yet
- Case Study (HOSPITAL)Document4 pagesCase Study (HOSPITAL)Reyna Mee AhiyasNo ratings yet
- Significance of The StudyDocument2 pagesSignificance of The StudyReyna Mee AhiyasNo ratings yet
- Weekly Course Learning Objectives (Postpartum)Document4 pagesWeekly Course Learning Objectives (Postpartum)Reyna Mee AhiyasNo ratings yet
- Physiologic Changes of PregnancyDocument7 pagesPhysiologic Changes of PregnancyReyna Mee AhiyasNo ratings yet
- The First Stage of LaborDocument5 pagesThe First Stage of LaborReyna Mee AhiyasNo ratings yet
- Draping in Lithotomy PositionDocument1 pageDraping in Lithotomy PositionReyna Mee AhiyasNo ratings yet
- Color Coding of Medication CardDocument1 pageColor Coding of Medication CardReyna Mee AhiyasNo ratings yet
- Learning Feedback DiaryDocument2 pagesLearning Feedback DiaryReyna Mee AhiyasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- IELTS Speaking Task Sheets: Week 8: HealthDocument1 pageIELTS Speaking Task Sheets: Week 8: HealthÁnh ĐỗNo ratings yet
- Energy Storage System Safety - Codes & Standards: David RosewaterDocument24 pagesEnergy Storage System Safety - Codes & Standards: David RosewaterDeepak GehlotNo ratings yet
- 03.affinity Efficacy PotencyDocument33 pages03.affinity Efficacy PotencyelitechemsNo ratings yet
- Makeup Consultation FormDocument2 pagesMakeup Consultation Formapi-339347949100% (1)
- MERS Coronavirus: Diagnostics, Epidemiology and TransmissionDocument21 pagesMERS Coronavirus: Diagnostics, Epidemiology and TransmissionramopavelNo ratings yet
- Employee Testing and Selection: Global Edition 12eDocument39 pagesEmployee Testing and Selection: Global Edition 12eMI2preciousNo ratings yet
- TUGAS I - BING 4104 - Reading IIDocument2 pagesTUGAS I - BING 4104 - Reading IIFaurizki TurziNo ratings yet
- Biology Curriculum and Assessment Guide (Secondary 4 - 6) : Science Education Key Learning AreaDocument139 pagesBiology Curriculum and Assessment Guide (Secondary 4 - 6) : Science Education Key Learning AreaUniversityJC100% (1)
- BmjvudxxzdrtyyhDocument14 pagesBmjvudxxzdrtyyhsoud aladwani100% (1)
- Ebola Virus DiseaseDocument3 pagesEbola Virus DiseasePoonam RanaNo ratings yet
- Magic CardDocument2 pagesMagic CardbedabyashmirdhaNo ratings yet
- Unit 5 Risk Assessment PDFDocument24 pagesUnit 5 Risk Assessment PDFReda MashalNo ratings yet
- MLA FormatDocument4 pagesMLA Formatkevin ochiengNo ratings yet
- 5 Essentials of Laboratory Wall FinishesDocument2 pages5 Essentials of Laboratory Wall FinishesBelay TadesseNo ratings yet
- DIASS Quarter1 Module 1Document24 pagesDIASS Quarter1 Module 1JoshNo ratings yet
- Muriatic Acid MsdsDocument6 pagesMuriatic Acid MsdsChe Gu BadriNo ratings yet
- Multimodal Imaging Evaluation of Excessive DaytimeDocument17 pagesMultimodal Imaging Evaluation of Excessive Daytimekano bhavNo ratings yet
- Project 2: Technical University of DenmarkDocument11 pagesProject 2: Technical University of DenmarkRiyaz AlamNo ratings yet
- Bladder Cancer GuidelieneDocument129 pagesBladder Cancer GuidelieneAndreas RonaldNo ratings yet
- Journalof Media Psychology 112008Document40 pagesJournalof Media Psychology 112008MUHAMMAD CHAMDAN HUSEINNo ratings yet
- CATCH UP FRIDAY DLL Feb 16Document5 pagesCATCH UP FRIDAY DLL Feb 16Raymart MagsumbolNo ratings yet
- Corrigendum-I: Prabandh Shikhar, Rau-Pithampur Road, Indore - 453556 PHONE: +91-731-2439630-34 FAX: +91-731-2439800Document65 pagesCorrigendum-I: Prabandh Shikhar, Rau-Pithampur Road, Indore - 453556 PHONE: +91-731-2439630-34 FAX: +91-731-2439800Shashank PriyadarshiNo ratings yet
- SEARO Proposal For Demonstration Project On R&D For Diabetes MellitusDocument17 pagesSEARO Proposal For Demonstration Project On R&D For Diabetes Mellitussubramanyam62No ratings yet
- 701 W. 51st Street Austin, Texas 78751 Phone-512-438-4800Document2 pages701 W. 51st Street Austin, Texas 78751 Phone-512-438-4800api-550348575No ratings yet
- Vol7No1 PDFDocument56 pagesVol7No1 PDFStereo PodNo ratings yet
- IMS ManualDocument70 pagesIMS ManualCandice100% (3)
- Going Viral ExcerptDocument20 pagesGoing Viral ExcerptI Read YA0% (3)
- CounsellingDocument6 pagesCounsellingNiharika savitaNo ratings yet
- Listeningpracticetest2 v9 18836014Document17 pagesListeningpracticetest2 v9 18836014FAREED PASHANo ratings yet
- 100 20210811 ICOPH 2021 Abstract BookDocument186 pages100 20210811 ICOPH 2021 Abstract Bookwafiq alibabaNo ratings yet