You might also like
- ITLS Advanced Pre-Test 9-20071Document7 pagesITLS Advanced Pre-Test 9-20071Atif Mohammed Al Yamany92% (12)
- Cat Dissection ReviewDocument4 pagesCat Dissection ReviewElijah PunzalanNo ratings yet
- Form TOOLBOX MEETINGDocument2 pagesForm TOOLBOX MEETINGLuthfi BahriNo ratings yet
- User's Guide: Hygro-Thermometer Alarm ClockDocument1 pageUser's Guide: Hygro-Thermometer Alarm ClockjNo ratings yet
- Rumah Sakit As-Syifa Ruang HcuDocument1 pageRumah Sakit As-Syifa Ruang HcuAlrahman JoneriNo ratings yet
- CDP Sleep DiaryDocument1 pageCDP Sleep DiaryRandall Short100% (1)
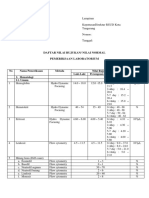
- Daftar Nilai Rujukan/ Nilai Normal Pemeriksaan LaboratoriumDocument7 pagesDaftar Nilai Rujukan/ Nilai Normal Pemeriksaan LaboratoriumOlivia Nur FathyaNo ratings yet
- Diabetic Retinopathy Screening ModuleDocument96 pagesDiabetic Retinopathy Screening ModuleSehaRizaNo ratings yet
- Diebetic TestDocument1 pageDiebetic Testعصام السامرائيNo ratings yet
- CDP Sleep DiaryDocument1 pageCDP Sleep Diaryzrombie7No ratings yet
- Diabetic Retinopathy Screening Module PDFDocument96 pagesDiabetic Retinopathy Screening Module PDFpet_al2001No ratings yet
- Names - Section: - Date: - Homework On Animal Reproduction I.Differentiate The Two Forms of ReproductionDocument4 pagesNames - Section: - Date: - Homework On Animal Reproduction I.Differentiate The Two Forms of ReproductionMaryNicoleDatlanginNo ratings yet
- Strictly Confidential!: Failure Mode and Effect AnalysisDocument11 pagesStrictly Confidential!: Failure Mode and Effect AnalysisWeekly Lean SeriesNo ratings yet
- Diebetic TestDocument1 pageDiebetic TestYusof MazlanNo ratings yet
- Colour WorksheetDocument2 pagesColour WorksheetEisya AbdullahNo ratings yet
- Daftar Prosedur Bedah AXA Mandiri Kesehatan PrimaDocument67 pagesDaftar Prosedur Bedah AXA Mandiri Kesehatan PrimasiucupNo ratings yet
- Type of Grouping StatisticsDocument3 pagesType of Grouping StatisticsИринаNo ratings yet
- Acute and ChronicDocument18 pagesAcute and ChronicShuvani ChughNo ratings yet
- Daftar Prosedur PDFDocument67 pagesDaftar Prosedur PDFDavid Raja MarpaungNo ratings yet
- Maintenance Medicines Liquidation FormDocument2 pagesMaintenance Medicines Liquidation FormBarangay CalaocanNo ratings yet
- Weekly Study Plan WorksheetDocument2 pagesWeekly Study Plan WorksheetAndantes ColombiaNo ratings yet
- 006 Museum Keyword MatrixDocument1 page006 Museum Keyword MatrixmuseumplanningNo ratings yet
- Department of Chemical Pathology: NormalDocument1 pageDepartment of Chemical Pathology: NormalHaris AkbarNo ratings yet
- Apollo Hospital International Limited: Nirali S.Donga A-One Pharmacy College (1 September, 2020 To 27 September, 2020)Document7 pagesApollo Hospital International Limited: Nirali S.Donga A-One Pharmacy College (1 September, 2020 To 27 September, 2020)Nirali DongaNo ratings yet
- Worksheet of Human Reproductive SystemDocument3 pagesWorksheet of Human Reproductive SystemMaria LorraineNo ratings yet
- CLAIM Analysis ReportDocument43 pagesCLAIM Analysis ReportRahul T ShedgeNo ratings yet
- Damage Onset Speed AnalisysDocument1 pageDamage Onset Speed Analisysgamusino2No ratings yet
- ST SH Words WeakDocument2 pagesST SH Words Weakilalika9926No ratings yet
- Daftar HadirDocument1 pageDaftar HadirAngga Dwi PutrantoNo ratings yet
- Parts of A Plant (Crossword)Document1 pageParts of A Plant (Crossword)zeqialNo ratings yet
- Reproductive SystemDocument1 pageReproductive SystemKathleen Ann NarismaNo ratings yet
- Gastro BrochureDocument3 pagesGastro Brochuregus_lionsNo ratings yet
- Chemistry: Edexcel Advanced Subsidiary GCE in Chemistry (8CH01) Edexcel Advanced GCE in Chemistry (9CH01)Document35 pagesChemistry: Edexcel Advanced Subsidiary GCE in Chemistry (8CH01) Edexcel Advanced GCE in Chemistry (9CH01)hassankhalidNo ratings yet
- Classwork: Complete The Following CrosswordDocument2 pagesClasswork: Complete The Following CrosswordJonathan Steve Norato PinzónNo ratings yet
- CrucigramaDocument2 pagesCrucigramaJonathan Steve Norato Pinzón0% (1)
- Weekly GoalsDocument1 pageWeekly GoalsAdryenn AshleyNo ratings yet
- 1.3 Basic Hydraulic Symbols and Major ComponentsDocument31 pages1.3 Basic Hydraulic Symbols and Major ComponentsMahmoud Mohamed100% (1)
- 1.3 Basic Hydraulic Symbols and Major ComponentsDocument31 pages1.3 Basic Hydraulic Symbols and Major ComponentsX800XLNo ratings yet
- 1.3 Basic Hydraulic Symbols and Major ComponentsDocument31 pages1.3 Basic Hydraulic Symbols and Major Componentsyared admassuNo ratings yet
- Basic Hydraulic Symbols and Major ComponentsDocument31 pagesBasic Hydraulic Symbols and Major Componentsmnowaq100% (1)
- 1.3 Basic Hydraulic Symbols and Major ComponentsDocument31 pages1.3 Basic Hydraulic Symbols and Major ComponentsKhaled RabeaNo ratings yet
- Absen Mentor Sains ViiDocument1 pageAbsen Mentor Sains ViiIbnu HunaisNo ratings yet
- Jurnal 1Document12 pagesJurnal 1ririandaluciNo ratings yet
- As Q2M5Document4 pagesAs Q2M5Glenda Manalo CochingNo ratings yet
- ACTIVITY 1 Nucleic AcidsDocument1 pageACTIVITY 1 Nucleic AcidsEllhai CaliwanNo ratings yet
- Msds 5130Document9 pagesMsds 5130Miguel LopezNo ratings yet
- Compliance and Therapy Report 10022023 142513Document2 pagesCompliance and Therapy Report 10022023 142513andreassantodomingoNo ratings yet
- TRUEor FALSEDocument1 pageTRUEor FALSEcrystalornias05No ratings yet
- Rehabilitation of The General BuildingDocument5 pagesRehabilitation of The General BuildingZuhair SaqafNo ratings yet
- Laboran - 4 - 29 Mei 2020Document1 pageLaboran - 4 - 29 Mei 2020ririsNo ratings yet
- Liloan Pumping Station Electro-Mech UpgradeDocument1 pageLiloan Pumping Station Electro-Mech UpgradeElvyn Fabellore HerreraNo ratings yet
- Directions: Identify The Parts of The Respiratory System. Write Your Answer On The Box ProvidedDocument2 pagesDirections: Identify The Parts of The Respiratory System. Write Your Answer On The Box ProvidedElsie A. GalvezNo ratings yet
- Medication Administration Record (MAR) : Facility NameDocument2 pagesMedication Administration Record (MAR) : Facility NameYouth AllenNo ratings yet
- Safe Motherhood Project Updated PresentationDocument43 pagesSafe Motherhood Project Updated Presentationmohamedamiinhassan6No ratings yet
- Vdocuments - MX MfagDocument170 pagesVdocuments - MX MfagEmpoy AlphaNo ratings yet
- How Does Canada Compare: OECD Health Data 2008Document3 pagesHow Does Canada Compare: OECD Health Data 2008caneman85No ratings yet
- QUIZ Sewing MachineDocument7 pagesQUIZ Sewing MachineMeldin May PerezNo ratings yet
- Surveilans Health Care Associated Infections: PersiDocument49 pagesSurveilans Health Care Associated Infections: Persifebri12No ratings yet
- Nutritional Biochemistry: From the Classroom to the Research BenchFrom EverandNutritional Biochemistry: From the Classroom to the Research BenchNo ratings yet
- Computational and Statistical Methods for Protein Quantification by Mass SpectrometryFrom EverandComputational and Statistical Methods for Protein Quantification by Mass SpectrometryNo ratings yet
- Clinical Medicine and Public Health Program Outline: Analytical SkillsDocument14 pagesClinical Medicine and Public Health Program Outline: Analytical SkillsdavidNo ratings yet
- نكليزيDocument4 pagesنكليزيdavidNo ratings yet
- ملزمه جديدDocument8 pagesملزمه جديدdavidNo ratings yet
- دبفبضلاا Spelling: broken underDocument7 pagesدبفبضلاا Spelling: broken underdavidNo ratings yet
- Vocabulary and Spelling: Hurts - Valid Librarian Course Fees QualificationsDocument12 pagesVocabulary and Spelling: Hurts - Valid Librarian Course Fees QualificationsdavidNo ratings yet
- Unit One: Take Up, Ankle, Sneeze, Pills, Bleeding, Skin Deeply PillsDocument11 pagesUnit One: Take Up, Ankle, Sneeze, Pills, Bleeding, Skin Deeply PillsdavidNo ratings yet
- خطّ الرقعة الدارج (العادي)Document16 pagesخطّ الرقعة الدارج (العادي)davidNo ratings yet
- داربيزخلاا و ميصىزنا Matching and Choices:: ةاىجنا 1. D 2. A 3. B 4. E 5. CDocument10 pagesداربيزخلاا و ميصىزنا Matching and Choices:: ةاىجنا 1. D 2. A 3. B 4. E 5. CdavidNo ratings yet
- Nursing Home Private Hospital / ICU: Treatment and Follow UpDocument1 pageNursing Home Private Hospital / ICU: Treatment and Follow UpdavidNo ratings yet
- Nursing Home Private Hospital / ICU Nursing Chart: 6 HR 18 HRDocument2 pagesNursing Home Private Hospital / ICU Nursing Chart: 6 HR 18 HRdavidNo ratings yet
- 5 Approach To The Patient With Disease of The Respiratory SystemDocument36 pages5 Approach To The Patient With Disease of The Respiratory SystemPhoebie Gael AsisNo ratings yet
- Indicator Dilution Method of Blood Flow MeasurementDocument3 pagesIndicator Dilution Method of Blood Flow MeasurementabhilashkrishnantkNo ratings yet
- ENDOTRACHEAL INTUBATIOn SandeepDocument17 pagesENDOTRACHEAL INTUBATIOn SandeepSimran JosanNo ratings yet
- Emergency Neurological Life Support: Airway, Ventilation, and SedationDocument17 pagesEmergency Neurological Life Support: Airway, Ventilation, and SedationLezard DomiNo ratings yet
- Bronchiectasis PathophysiologyDocument1 pageBronchiectasis PathophysiologyRayne Dunstan Pascual VergaraNo ratings yet
- Rockwool Pipe MSDSDocument5 pagesRockwool Pipe MSDSJullius CarballoNo ratings yet
- NCP For SVTDocument6 pagesNCP For SVTRen VillenaNo ratings yet
- A Case of COVID-19 Infection: Chief Symptom, Diarrhea To The EditorDocument2 pagesA Case of COVID-19 Infection: Chief Symptom, Diarrhea To The EditorJor GarciaNo ratings yet
- AlbatrossDocument5 pagesAlbatrossJuan David Ospina GonzalezNo ratings yet
- Esophageal Intubation? Just Look at Your Monitors!: ¿Intubación Esofágica? ¡Mire Sus Monitores!Document2 pagesEsophageal Intubation? Just Look at Your Monitors!: ¿Intubación Esofágica? ¡Mire Sus Monitores!MARJORIE LISSETH CALDERON LOZANONo ratings yet
- Carga Horária Mensal 04 Códigos Das Habilidades Objetos de ConhecimentosDocument8 pagesCarga Horária Mensal 04 Códigos Das Habilidades Objetos de ConhecimentosRX7 FFNo ratings yet
- ICU Ventilator - Group 4Document26 pagesICU Ventilator - Group 4Anh TrầnNo ratings yet
- Cybermed Oxi-Vent Transport Ventilator FinalDocument55 pagesCybermed Oxi-Vent Transport Ventilator FinalAbdo BedoNo ratings yet
- Chemical Hazard Bulletin: Potassium Silver (I) CyanideDocument1 pageChemical Hazard Bulletin: Potassium Silver (I) CyanideHaleemUrRashidBangashNo ratings yet
- Module 1 - Heart AnatomyDocument1 pageModule 1 - Heart AnatomytararraNo ratings yet
- Keyword: Acute Resporitory Infection, Under Five Children Characteristic, Physical Condition of House, Occupant BehaviorDocument10 pagesKeyword: Acute Resporitory Infection, Under Five Children Characteristic, Physical Condition of House, Occupant BehaviorPutri Permatasari WakidiNo ratings yet
- Updated-MARC ARBOUR CITY HOTEL-COSHH Assessment 2 - Paint Thinner PlusDocument2 pagesUpdated-MARC ARBOUR CITY HOTEL-COSHH Assessment 2 - Paint Thinner PlusPaul McGahanNo ratings yet
- Taking Vital SignsDocument6 pagesTaking Vital SignsKIAT SMART - Putri Septi Yanti NadilaNo ratings yet
- EVI - SDS - E1017 - PU Catalyst (Hardener) at 50%Document15 pagesEVI - SDS - E1017 - PU Catalyst (Hardener) at 50%Rohith RahulNo ratings yet
- Material Safety Data Sheet: PAC - RDocument6 pagesMaterial Safety Data Sheet: PAC - RJose AlejandroBlancoNo ratings yet
- Common Complications of Iv TherapyDocument63 pagesCommon Complications of Iv TherapyFrancis James RigodonNo ratings yet
- Patient Assessment Marking SheetDocument2 pagesPatient Assessment Marking SheetJim Courtney100% (4)
- Deltacide (2013)Document11 pagesDeltacide (2013)rei estacioNo ratings yet
- Fundamentals of Nursing Exam 16 (85 Items)Document13 pagesFundamentals of Nursing Exam 16 (85 Items)Mimi VeeNo ratings yet
- PDF Inderbir Singh S Textbook of Anatomy Thorax Abdomen and Pelvis Vol 2 6Th Edition Inderbir Singh Ebook Full ChapterDocument53 pagesPDF Inderbir Singh S Textbook of Anatomy Thorax Abdomen and Pelvis Vol 2 6Th Edition Inderbir Singh Ebook Full Chapterjeannette.king876100% (2)
- Vitamin B Complex Injection SDS (Aug2016) PDFDocument5 pagesVitamin B Complex Injection SDS (Aug2016) PDFERICA LILIAN ESGUERRA GILNo ratings yet
- Manual Capnografo EMMADocument33 pagesManual Capnografo EMMAAlejandro Barrera Torres0% (1)
- Steris - Enzycare2 - Enzymatic Presoak and CleanerDocument2 pagesSteris - Enzycare2 - Enzymatic Presoak and CleanerWalid KhalidNo ratings yet
- BTL SpirometrieDocument4 pagesBTL SpirometrieMeiNo ratings yet