You might also like
- CorneaDocument465 pagesCorneawisinasa100% (2)
- CPG 19Document78 pagesCPG 19anon-24970100% (1)
- Dry EyeDocument2 pagesDry EyeDaya PNo ratings yet
- Ophthalmology: Almendrala-Molina, Jorja Post Graduate InternDocument65 pagesOphthalmology: Almendrala-Molina, Jorja Post Graduate InternJajaAlmendralaNo ratings yet
- The Lacrimal System: Lynn E. Lawrence, CPOT, ABOC, COA, OSCDocument31 pagesThe Lacrimal System: Lynn E. Lawrence, CPOT, ABOC, COA, OSCUlayya Ghina NabillaNo ratings yet
- Topic 12-Special Senses: Eyes: Name: Jewel Eve Balida Competency Appraisal Date: 10/17/16Document9 pagesTopic 12-Special Senses: Eyes: Name: Jewel Eve Balida Competency Appraisal Date: 10/17/16Lewej Eve Laurente AdilabNo ratings yet
- Corneal Dystrophies: Retinal DetachmentDocument5 pagesCorneal Dystrophies: Retinal DetachmentCake ManNo ratings yet
- DRY EYE AgungDocument23 pagesDRY EYE AgungGustiAngriAngalanNo ratings yet
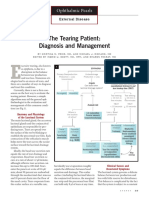
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- Dry Eye Syndrome OverviewDocument7 pagesDry Eye Syndrome OverviewhaninamaulianiNo ratings yet
- Dry Eye SyndromeDocument39 pagesDry Eye Syndromeمحمد عمر الجركNo ratings yet
- Eye and Vision Problems GuideDocument11 pagesEye and Vision Problems GuideDarius CrisostomoNo ratings yet
- Perceptual DisturbancesDocument7 pagesPerceptual DisturbancesVin SageNo ratings yet
- The EyeDocument8 pagesThe Eyezyrine jhen100% (1)
- The CorneaDocument60 pagesThe CorneaSarahNo ratings yet
- Marco-Equinox-Patient Hand OutDocument2 pagesMarco-Equinox-Patient Hand OutDr. Richard JohnsonNo ratings yet
- Unit 3Document14 pagesUnit 3Krunal ParmarNo ratings yet
- Corneal Dystrophies, Contact Lenses, and Retinal Detachment GuideDocument6 pagesCorneal Dystrophies, Contact Lenses, and Retinal Detachment GuideMarissa AsimNo ratings yet
- General Eye Care: Prepared By: Ma. Elena Fe G. Acosta, SN4, HTUDocument26 pagesGeneral Eye Care: Prepared By: Ma. Elena Fe G. Acosta, SN4, HTUmefacostaNo ratings yet
- The Healthy Eye: Structure, Function and Common Eye DiseasesDocument38 pagesThe Healthy Eye: Structure, Function and Common Eye DiseasesHasnain Ahmad KhanNo ratings yet
- Secondary Glaucoma IGADocument28 pagesSecondary Glaucoma IGANur JannahNo ratings yet
- M040GB014A00A-DOC00 - Smart ScreeningDocument11 pagesM040GB014A00A-DOC00 - Smart Screeningrocol.aplicaciones2No ratings yet
- Eyes, Ears, Nose, Throat and Mouth AssessmentDocument86 pagesEyes, Ears, Nose, Throat and Mouth AssessmentD A M N E R ANo ratings yet
- Special Senses (1)Document8 pagesSpecial Senses (1)Giane Qeirr Osias TimmalogNo ratings yet
- Red Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMDocument23 pagesRed Eye - Conjunctivitis I Dr. Nuke Erlina Mayasari, SPMismkipendprowil2No ratings yet
- NCM 114 Finals LectureDocument11 pagesNCM 114 Finals LectureClea Amber FullanteNo ratings yet
- Secondary Glaucomas: Printed July 2014 Review Date July 2017Document28 pagesSecondary Glaucomas: Printed July 2014 Review Date July 2017Anonymous YYWsfmocYNo ratings yet
- Chp6 Ocular Surface DiseasesDocument31 pagesChp6 Ocular Surface DiseasesarifdikmanNo ratings yet
- BLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONDocument15 pagesBLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONWaiwit KritayakiranaNo ratings yet
- Computer Vision Syndrome and Dry Eye: Causes, Symptoms, and TreatmentsDocument37 pagesComputer Vision Syndrome and Dry Eye: Causes, Symptoms, and TreatmentsIntan Winta PratiwiNo ratings yet
- Anatomyphysiology ReviewerDocument116 pagesAnatomyphysiology Reviewerrosekatekate929No ratings yet
- Assessing The EyesDocument61 pagesAssessing The EyessrslytrdNo ratings yet
- ATENGCO - Activity11 The Sense OrgansDocument8 pagesATENGCO - Activity11 The Sense OrgansJoann Mae PudaderaNo ratings yet
- Chapter 8 AnaPhyDocument15 pagesChapter 8 AnaPhyCorinne VizcondeNo ratings yet
- 4 23Document8 pages4 23Camila Díaz QuinterosNo ratings yet
- DISORDERS of The EYE and EARDocument8 pagesDISORDERS of The EYE and EARAnna Carmela P. MelendezNo ratings yet
- Dry EyeDocument36 pagesDry EyeJ NATASHA MARIANo ratings yet
- DARE's Eye PDFDocument33 pagesDARE's Eye PDFvirag.patilNo ratings yet
- Dry Eye Investigation Management 2003Document18 pagesDry Eye Investigation Management 2003Harminul Isya100% (1)
- 8 Lacrimal Drainage System Diseases by James PMDocument63 pages8 Lacrimal Drainage System Diseases by James PMCharles AntonyNo ratings yet
- Eye PDFDocument16 pagesEye PDFhasbshahNo ratings yet
- The EyeDocument48 pagesThe Eyezyrine jhen100% (1)
- Special SensesDocument10 pagesSpecial SensesEthel May AlabastroNo ratings yet
- Eyelid Orbit and ConjunctivaDocument123 pagesEyelid Orbit and ConjunctivaRgdNo ratings yet
- Eye PPT 01Document21 pagesEye PPT 01zzzNo ratings yet
- NursingDocument4 pagesNursingAndrea Jewel BaladjayNo ratings yet
- Danni All'occhio Dopo Intervento Da Neurinoma AcusticoDocument20 pagesDanni All'occhio Dopo Intervento Da Neurinoma Acusticoctenzo56No ratings yet
- Human Eye Sec4 BioDocument10 pagesHuman Eye Sec4 BioFrancine TheophilaNo ratings yet
- U2 OphthalmicTerminologyDocument6 pagesU2 OphthalmicTerminologyAlberto Ybañez CastañedaNo ratings yet
- The Human EyeDocument33 pagesThe Human Eyegrace liwantoNo ratings yet
- DRY EYE AgungDocument23 pagesDRY EYE AgungGustiAngriAngalanNo ratings yet
- Dry Eye AgungDocument23 pagesDry Eye AgungAgung TriatmojoNo ratings yet
- Mata Merah 2Document26 pagesMata Merah 2Miftahuljnh01No ratings yet
- Eye ExaminationDocument34 pagesEye ExaminationSashwini DheviNo ratings yet
- Visual SystemDocument6 pagesVisual SystemJobelle Acena100% (1)
- Anatomy of Human EyeDocument41 pagesAnatomy of Human EyeCarly MelachioNo ratings yet
- BlepDocument1 pageBlepSweet CandyNo ratings yet
- Assessment of The EyesDocument9 pagesAssessment of The Eyesmarkkkkkkkheeess100% (3)
- Journal Article 27 487 PDFDocument4 pagesJournal Article 27 487 PDFrifkidwianugrahNo ratings yet
- The Lacrimal System: Anatomy and FunctionDocument6 pagesThe Lacrimal System: Anatomy and FunctionIon NagomirNo ratings yet
- Dry Eye SyndromeDocument69 pagesDry Eye Syndromeendalew mulugetaNo ratings yet
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsFrom EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsNo ratings yet
- Wound ManagementDocument53 pagesWound ManagementJay DeeNo ratings yet
- Foreign Body Airway Obstruction First AidDocument87 pagesForeign Body Airway Obstruction First AidPrincess Cate MercadoNo ratings yet
- Types of Wounds 2Document30 pagesTypes of Wounds 2Jay Dee100% (1)
- EMED4Document59 pagesEMED4Princess Cate MercadoNo ratings yet
- EMED2Document23 pagesEMED2Princess Cate MercadoNo ratings yet
- Types of Wounds 2Document30 pagesTypes of Wounds 2Jay Dee100% (1)
- FB Airway Obstruction in Adults & ChildrenDocument28 pagesFB Airway Obstruction in Adults & ChildrenPrincess Cate MercadoNo ratings yet
- Emed - BLS - FBAO - First Aid Part 1Document85 pagesEmed - BLS - FBAO - First Aid Part 1Princess Cate MercadoNo ratings yet
- Emed - BLS - FBAO - First Aid Part 1Document85 pagesEmed - BLS - FBAO - First Aid Part 1Princess Cate MercadoNo ratings yet
- Wound ManagementDocument53 pagesWound ManagementJay DeeNo ratings yet
- Special Resuscitation Situations: Stroke, Hypothermia, Anaphylaxis, Drowning, Trauma, PregnancyDocument55 pagesSpecial Resuscitation Situations: Stroke, Hypothermia, Anaphylaxis, Drowning, Trauma, PregnancyPrincess Cate MercadoNo ratings yet
- Emed - TriageDocument54 pagesEmed - TriagePrincess Cate MercadoNo ratings yet
- Emed - Pedia2 GiNeuroDocument7 pagesEmed - Pedia2 GiNeuroPrincess Cate MercadoNo ratings yet
- Shock: Types, Causes, Signs and TreatmentDocument34 pagesShock: Types, Causes, Signs and TreatmentPrincess Cate MercadoNo ratings yet
- Emed - Advance Cardiac Life Support (Doc Vito)Document38 pagesEmed - Advance Cardiac Life Support (Doc Vito)Princess Cate MercadoNo ratings yet
- RV Ollero MD's Guide to Advanced Trauma Life SupportDocument18 pagesRV Ollero MD's Guide to Advanced Trauma Life SupportPrincess Cate MercadoNo ratings yet
- Emed - Trauma Life Support (Doc Ollero)Document51 pagesEmed - Trauma Life Support (Doc Ollero)Princess Cate MercadoNo ratings yet
- Wound Closure TechniqueDocument73 pagesWound Closure TechniqueJay DeeNo ratings yet
- Emed - Principles of Poison ManagementDocument40 pagesEmed - Principles of Poison ManagementPrincess Cate MercadoNo ratings yet
- Emed - Pedia 1Document7 pagesEmed - Pedia 1Princess Cate MercadoNo ratings yet
- Emed - Pulmonary EmergenciesDocument13 pagesEmed - Pulmonary EmergenciesPrincess Cate MercadoNo ratings yet
- Emed - Airway Management of The Trauma VictimDocument49 pagesEmed - Airway Management of The Trauma VictimPrincess Cate MercadoNo ratings yet
- Emed - Pulmonary Emergencies (Doc Vito) .PDFXDocument13 pagesEmed - Pulmonary Emergencies (Doc Vito) .PDFXPrincess Cate MercadoNo ratings yet
- Emed - OB Part 1Document6 pagesEmed - OB Part 1Princess Cate MercadoNo ratings yet
- Emed - Advance Cardiac Life SupportDocument45 pagesEmed - Advance Cardiac Life SupportPrincess Cate MercadoNo ratings yet
- Suture MaterialsDocument39 pagesSuture MaterialsJay DeeNo ratings yet
- Emed - Head Injuries (Doc Ollero)Document49 pagesEmed - Head Injuries (Doc Ollero)Princess Cate MercadoNo ratings yet
- Emed DR de Guzman SamplexDocument2 pagesEmed DR de Guzman SamplexMarco TolentinoNo ratings yet
- Emed - OB Part 2Document4 pagesEmed - OB Part 2Princess Cate MercadoNo ratings yet
- ACLSDocument37 pagesACLSWendy LucasNo ratings yet
- Shadrack Muma ThesisDocument74 pagesShadrack Muma ThesisJune BellNo ratings yet
- Vernal Keratoconjunctivitis: Moderator-Dr. Seema Meena Presenter - Dr. Sulabh SahuDocument58 pagesVernal Keratoconjunctivitis: Moderator-Dr. Seema Meena Presenter - Dr. Sulabh SahuSulabh SahuNo ratings yet
- Eyelid & Lacrimal DisordersDocument35 pagesEyelid & Lacrimal Disordersputri wid100% (1)
- Dry Eye ManagementDocument8 pagesDry Eye ManagementMul YaniNo ratings yet
- Wang 2005Document10 pagesWang 2005Anggia BungaNo ratings yet
- Computer Vision Syndrome (Digital Eye Strain) - EyeWikiDocument12 pagesComputer Vision Syndrome (Digital Eye Strain) - EyeWikiYeremia JerryNo ratings yet
- Contact Lenses and Associated AnteriorDocument13 pagesContact Lenses and Associated AnteriorJose Antonio Fuentes VegaNo ratings yet
- Lipofilm Microemulsion Effectiveness in Dry EyeDocument5 pagesLipofilm Microemulsion Effectiveness in Dry Eyedr.cintaNo ratings yet
- KeratitisDocument70 pagesKeratitisHoopmen Silaen100% (1)
- Eyes Condition Associated With Exposure To HazeDocument15 pagesEyes Condition Associated With Exposure To HazeTria PahanNo ratings yet
- Frequency and Risk Factors of Symptomatic Dry Eye Disease at Tertiary Care Eye Hospital, KarachiDocument4 pagesFrequency and Risk Factors of Symptomatic Dry Eye Disease at Tertiary Care Eye Hospital, KarachiekalapaleloNo ratings yet
- Anatomi Dan Fisiologi KorneaDocument133 pagesAnatomi Dan Fisiologi KorneaAriyanie NurtaniaNo ratings yet
- Cornea and External DiseaseDocument26 pagesCornea and External Diseaserajeshwari saravananNo ratings yet
- EYE DISORDERS: GLAUCOMA AND CATARACTSDocument127 pagesEYE DISORDERS: GLAUCOMA AND CATARACTSjoan olanteNo ratings yet
- Rev G - TearLab Osmolarity System User Manual - EnglishDocument20 pagesRev G - TearLab Osmolarity System User Manual - EnglishRommel ValladaresNo ratings yet
- Dry EyeDocument36 pagesDry EyeJ NATASHA MARIANo ratings yet
- How Does Radiation Therapy Work?Document5 pagesHow Does Radiation Therapy Work?mikeadrianNo ratings yet
- BLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONDocument15 pagesBLEPHAROKERATOCONJUNCTIVITIS: EYE INFLAMMATIONWaiwit KritayakiranaNo ratings yet
- Drug Rewetting Drops, Artificial TearsDocument1 pageDrug Rewetting Drops, Artificial TearsSrkocherNo ratings yet
- Oamjms 10b 668Document6 pagesOamjms 10b 668Faris Mufid MadyaputraNo ratings yet
- An Insight Into Meibomian Gland DysfunctionDocument22 pagesAn Insight Into Meibomian Gland DysfunctionvalbayerosNo ratings yet
- Hom M, Demodex - Clinical Cases & Diagnostic Protocol. OVS 2013Document8 pagesHom M, Demodex - Clinical Cases & Diagnostic Protocol. OVS 2013cassie_kuldaNo ratings yet
- Ocular Pharmacology - Dr. Fermin (2023)Document6 pagesOcular Pharmacology - Dr. Fermin (2023)Patricia Manalili100% (1)
- Senior Citizen's Day - 27 August 2019Document8 pagesSenior Citizen's Day - 27 August 2019Times MediaNo ratings yet
- A Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Document10 pagesA Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Lepaksha GowdaNo ratings yet
- Ophthalmology NotesDocument82 pagesOphthalmology NotesDr-Fadi AlkayyaliNo ratings yet
- Vision and Values: Teacher ManualDocument133 pagesVision and Values: Teacher ManualWim SupergansNo ratings yet
- MCQ in OphthalmologyDocument107 pagesMCQ in OphthalmologyDr-Arsalan Zahid100% (2)