You might also like
- Case Study (Lung Cancer)Document17 pagesCase Study (Lung Cancer)Jobelle Acena100% (1)
- EyeDocument50 pagesEyedavid100% (1)
- Characteristics and Functions of Blood ComponentsDocument51 pagesCharacteristics and Functions of Blood ComponentssamayaNo ratings yet
- Lecture 9 The Digestive SystemDocument59 pagesLecture 9 The Digestive SystemMatthew Bargo100% (2)
- GI Anatomy, Physiology, Disorders & DiagnosticsDocument52 pagesGI Anatomy, Physiology, Disorders & Diagnosticsprabha5050100% (1)
- Geoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)Document77 pagesGeoffrey J. Gladstone, Frank A. Nesi, Evan H. Black - Oculoplastic Surgery Atlas - Cosmetic Facial Surgery-Springer (2018)DANIEL GIRALDONo ratings yet
- 06 - 07 - Anatomy of The Chest Wall and BreastDocument16 pages06 - 07 - Anatomy of The Chest Wall and Breastbo gum parkNo ratings yet
- Chapter 1Document62 pagesChapter 1Ashenafi PaulosNo ratings yet
- Lymphatic SystemDocument22 pagesLymphatic SystemArnab GuinNo ratings yet
- Chapter 1 Introduction To Anatomy and PhysiologyDocument29 pagesChapter 1 Introduction To Anatomy and PhysiologyScarlett Johnson100% (1)
- Anti Psychotic DrugsDocument2 pagesAnti Psychotic DrugscalfornianursingacadNo ratings yet
- Chapter 1 The Human OrganismDocument45 pagesChapter 1 The Human OrganismTrumanXX100% (1)
- Anaphy NotesDocument6 pagesAnaphy NotesTrishaNo ratings yet
- Diagnostic Tests Guide for NursesDocument2 pagesDiagnostic Tests Guide for NursesBenedict AlvarezNo ratings yet
- Fertility Awareness-Based Methods and LactationalDocument29 pagesFertility Awareness-Based Methods and LactationalHowardNo ratings yet
- Final Exam Review Worksheet Introduction-Chapter 1Document30 pagesFinal Exam Review Worksheet Introduction-Chapter 1Jensen BarrettNo ratings yet
- STIs: Common Types, Symptoms and PreventionDocument100 pagesSTIs: Common Types, Symptoms and PreventionEstrella M. Ramirez-Lawas100% (1)
- Histology of The Special SenseDocument84 pagesHistology of The Special SenseRushda100% (1)
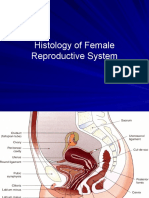
- Female ReproductiveDocument34 pagesFemale ReproductiveAbdallah A. Abu Mattar100% (2)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- Special Senses NotesDocument3 pagesSpecial Senses NotesChelsa LeyritanaNo ratings yet
- Sensory OrgansDocument11 pagesSensory OrgansCurex QANo ratings yet
- Nervous Part 2Document61 pagesNervous Part 2Josh Brenner100% (1)
- Senses (Nervous 3)Document56 pagesSenses (Nervous 3)Josh BrennerNo ratings yet
- Ophtalmic Remedi HomeopathyDocument59 pagesOphtalmic Remedi Homeopathymihaipopescu0No ratings yet
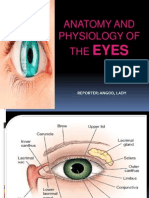
- Anatomy and Physiology of The EyesDocument20 pagesAnatomy and Physiology of The EyesLaidy Aizahlyn Indoc Angod100% (2)
- Subjective: Ventilation AssistanceDocument3 pagesSubjective: Ventilation AssistanceJobelle Acena100% (2)
- Special SensesDocument6 pagesSpecial SensesmasorNo ratings yet
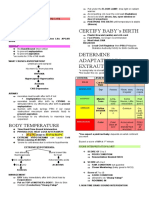
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- The Urinary System & Fluid BalanceDocument8 pagesThe Urinary System & Fluid BalanceMarianne DugosNo ratings yet
- Family Abuse and NeglectDocument20 pagesFamily Abuse and Neglectapi-311788459100% (1)
- Chapter 3Document96 pagesChapter 3Sinclyr Valenciano100% (2)
- Immunologic Disorders ExplainedDocument73 pagesImmunologic Disorders ExplainedDjayNo ratings yet
- Frcophth 400 Sbas and CrqsDocument262 pagesFrcophth 400 Sbas and CrqsZaheer Ullah Soleh100% (1)
- Physical AssessmentDocument19 pagesPhysical Assessmentsilentscream0618No ratings yet
- Seeley's Ess9e.chapt11 - Lecture.aDocument43 pagesSeeley's Ess9e.chapt11 - Lecture.aJhara100% (2)
- Geriatric Case StudyDocument15 pagesGeriatric Case StudyJobelle AcenaNo ratings yet
- EthicsDocument77 pagesEthicsAce Visuals100% (2)
- ER Protocols in The PhilippinesDocument9 pagesER Protocols in The PhilippinesJobelle Acena100% (1)
- Urinary SystemDocument9 pagesUrinary SystemCUESCANO, CRISTEL G. BSMT 2-ANo ratings yet
- Urinary SystemDocument80 pagesUrinary SystemRoeisa Salinas100% (1)
- Immune SystemDocument36 pagesImmune SystemAyessa Yvonne PanganibanNo ratings yet
- Digestive and Body MetabolismDocument25 pagesDigestive and Body MetabolismGuenNo ratings yet
- Psychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeDocument10 pagesPsychiatric Nursing Michael Jimenez, PENTAGON Slovin'S Formula: N 1 + NeJobelle AcenaNo ratings yet
- Case Study (ACS)Document12 pagesCase Study (ACS)Kristel Joy Cabarrubias Acena100% (1)
- Notes On Obstetrics: Normal Labor (Theories of Labor Onset)Document22 pagesNotes On Obstetrics: Normal Labor (Theories of Labor Onset)Jobelle Acena100% (1)
- Bioethics in Nursing Practice: Principles of Autonomy and Informed ConsentDocument5 pagesBioethics in Nursing Practice: Principles of Autonomy and Informed ConsentVhinny Macabontoc100% (1)
- Osama - S Ophthalmology Notes FEBRUARY 2019 EDITIONDocument42 pagesOsama - S Ophthalmology Notes FEBRUARY 2019 EDITIONNazish Saghir67% (3)
- Eye, Orbit, Orbital Region, andDocument72 pagesEye, Orbit, Orbital Region, andSmartyna Sophia100% (1)
- Case StudyDocument10 pagesCase StudyJobelle AcenaNo ratings yet
- Body CavitiesDocument22 pagesBody Cavitiesapi-421876727100% (1)
- Eye AnatomyDocument21 pagesEye AnatomyHammad afzal100% (2)
- Vasectomy Definition, Procedure & EffectivenessDocument3 pagesVasectomy Definition, Procedure & EffectivenessAnggy Wardhini100% (1)
- Anatomy of The EyesDocument35 pagesAnatomy of The EyesKiela Nicole Gatpandan AguilarNo ratings yet
- Development of Gastrointestinal SystemDocument29 pagesDevelopment of Gastrointestinal SystemrifkaraihanaNo ratings yet
- Tissue - SeeleyDocument61 pagesTissue - SeeleyJuli Damayanty Harahap100% (1)
- Shock: Blood TransfusionDocument81 pagesShock: Blood TransfusionBir Mohammad SonetNo ratings yet
- Overview of The Immune SystemDocument9 pagesOverview of The Immune SystemAyadi P. AkinwandeNo ratings yet
- Anatomy of The Eye PDFDocument15 pagesAnatomy of The Eye PDFPaolo Naguit0% (1)
- Normal NewbornAssessmentDocument53 pagesNormal NewbornAssessmentMidori SanNo ratings yet
- Cranial NerveDocument4 pagesCranial NerveBrian OballoNo ratings yet
- Fluid and Electrolyte Management of The Surgical PatientDocument26 pagesFluid and Electrolyte Management of The Surgical PatientYudhi Leo PrimaNo ratings yet
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- Lecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMDocument53 pagesLecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMlilimanao86% (7)
- Nursing Ethics: Raymund Christopher R. Dela Peña, RN, RMDocument23 pagesNursing Ethics: Raymund Christopher R. Dela Peña, RN, RMrnrmmanphd100% (1)
- Madera vs. COADocument53 pagesMadera vs. COAMaVictoria AytonaNo ratings yet
- Histology of Male Reproductive SystemDocument56 pagesHistology of Male Reproductive SystemMuhammad Irfan100% (2)
- PancreasDocument20 pagesPancreasnarendramedaNo ratings yet
- Chapter 8 - The VitaminsDocument3 pagesChapter 8 - The VitaminsYcell Latido100% (1)
- The Human Body A Nutrition PerspectiveDocument50 pagesThe Human Body A Nutrition PerspectiveRichard GelmanNo ratings yet
- Dr. Carlos S. Lanting College Ana-Physio Course SyllabusDocument7 pagesDr. Carlos S. Lanting College Ana-Physio Course SyllabusGabriel CruzNo ratings yet
- Endocrine SystemDocument4 pagesEndocrine SystemMary Louwelyn GurreaNo ratings yet
- Sensory Physiology Student ProtocolDocument18 pagesSensory Physiology Student ProtocolManuel Alejandro Chiguay GonzalezNo ratings yet
- Female Reproductive SystemDocument6 pagesFemale Reproductive SystemממתצמתצמצתNo ratings yet
- ANPH-M2-CU9. Respiratory SystemDocument8 pagesANPH-M2-CU9. Respiratory SystemMary Grace Mapula100% (1)
- BMED 3107 Endocrine & Reproductive Systems DevelopmentDocument32 pagesBMED 3107 Endocrine & Reproductive Systems DevelopmentMarisol AcostaNo ratings yet
- Breasts and AxillaeDocument10 pagesBreasts and Axillaedlneisha61100% (1)
- Intergumentary SystemDocument2 pagesIntergumentary SystemAkihiro FurukawaNo ratings yet
- The Muscular SystemDocument183 pagesThe Muscular SystemRochelle Antig100% (2)
- Muscular TissueDocument18 pagesMuscular Tissueabbaslafe100% (1)
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Visual Disorder Insights: Altered Perception PatternsDocument7 pagesVisual Disorder Insights: Altered Perception PatternsJobelle AcenaNo ratings yet
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalDocument5 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale Evaluation Short Term Goal Independent: Short Term GoalJobelle AcenaNo ratings yet
- Date/Schedule Activities Expected Output Verified/Checked by Area in ChargeDocument2 pagesDate/Schedule Activities Expected Output Verified/Checked by Area in ChargeJobelle AcenaNo ratings yet
- Pediatric Case StudyDocument21 pagesPediatric Case StudyJobelle AcenaNo ratings yet
- NCM 107 SY 2020-2021: Legal and Ethical Consideration of Euthanasia in India: A Choice Between Life and DeathDocument8 pagesNCM 107 SY 2020-2021: Legal and Ethical Consideration of Euthanasia in India: A Choice Between Life and DeathJobelle AcenaNo ratings yet
- NCM 107 Leadership and Management RLEDocument4 pagesNCM 107 Leadership and Management RLEJobelle AcenaNo ratings yet
- Union Christian College School of Health and Sciences City of San Fernando La UnionDocument11 pagesUnion Christian College School of Health and Sciences City of San Fernando La UnionJobelle AcenaNo ratings yet
- Difference Between Mechanism of Action of Cell Mediated Immune System and Humoral Mediated Immune SystemDocument4 pagesDifference Between Mechanism of Action of Cell Mediated Immune System and Humoral Mediated Immune SystemJobelle AcenaNo ratings yet
- GC ncp1Document2 pagesGC ncp1Jobelle AcenaNo ratings yet
- GC ncp1 and 2Document4 pagesGC ncp1 and 2Jobelle AcenaNo ratings yet
- Er Drugs StudyDocument80 pagesEr Drugs StudyJobelle AcenaNo ratings yet
- DRUG STUDY (Lung Cancer)Document10 pagesDRUG STUDY (Lung Cancer)Jobelle AcenaNo ratings yet
- SummaryDocument1 pageSummaryJobelle AcenaNo ratings yet
- Online LectureDocument9 pagesOnline LectureJobelle AcenaNo ratings yet
- Nursing Care Plans for Fever, Wound Healing and Pressure UlcerDocument11 pagesNursing Care Plans for Fever, Wound Healing and Pressure UlcerJobelle AcenaNo ratings yet
- Normal Cell GrowthDocument5 pagesNormal Cell GrowthJobelle AcenaNo ratings yet
- Nursing: Core Values of NursingDocument14 pagesNursing: Core Values of NursingJobelle AcenaNo ratings yet
- PHARMAfdDocument7 pagesPHARMAfdJobelle AcenaNo ratings yet
- Assessing The EyesDocument61 pagesAssessing The EyessrslytrdNo ratings yet
- Meghna PresentationDocument72 pagesMeghna PresentationSoumen Roy SourovNo ratings yet
- Heen P and RDocument6 pagesHeen P and RTamara Kate HalicanNo ratings yet
- Anatomy of Eye AppendigesDocument19 pagesAnatomy of Eye AppendigesSiyaNo ratings yet
- Eye Eye Assessment Assessment and Care and CareDocument126 pagesEye Eye Assessment Assessment and Care and CareBern NerquitNo ratings yet
- Eye Structure and FunctionsDocument9 pagesEye Structure and FunctionsFraiza BirowaNo ratings yet
- Orbital Cellulitis GuideDocument49 pagesOrbital Cellulitis GuideCarmela VargasNo ratings yet
- Jadwal Penguatan Kompetensi Perawat Mata Tahun 2023Document10 pagesJadwal Penguatan Kompetensi Perawat Mata Tahun 2023ThabutiNo ratings yet
- Anatomy of The EyesDocument2 pagesAnatomy of The EyesTricia De TorresNo ratings yet
- Trigeminal Nerve Anatomy PDFDocument13 pagesTrigeminal Nerve Anatomy PDFvinaykishore0% (1)
- Anatomy of The Eye and Orbit The Clinical.12Document1 pageAnatomy of The Eye and Orbit The Clinical.12asad aliNo ratings yet
- Nerves of The OrbitDocument6 pagesNerves of The OrbitAshifa SahiraNo ratings yet
- Aa AnatomyDocument109 pagesAa AnatomyshailendraNo ratings yet
- 10.7556 Jaoa.2015.022Document5 pages10.7556 Jaoa.2015.022CarolinaNo ratings yet
- Asvs 04 0267Document7 pagesAsvs 04 0267T KNo ratings yet
- EDentistryy Textbook of Trigeminal NeuralgiaDocument257 pagesEDentistryy Textbook of Trigeminal NeuralgiaLily BlossomNo ratings yet
- Lacrimal Apparatus - DR AshwiniDocument36 pagesLacrimal Apparatus - DR AshwiniAlv JDNo ratings yet
- ICO - Basic Science Instructions For CandidatesDocument20 pagesICO - Basic Science Instructions For Candidatesrak3uNo ratings yet
- Unusual and Rare Complications of Orthognathic Surgery: A Literature ReviewDocument14 pagesUnusual and Rare Complications of Orthognathic Surgery: A Literature ReviewRodrigo RojasNo ratings yet
- Eyelid and Anterior Eye Segment Procedures CodesDocument34 pagesEyelid and Anterior Eye Segment Procedures CodesnasrudinNo ratings yet
- Cranial Nerves GuideDocument18 pagesCranial Nerves GuideAndrew EldeiryNo ratings yet