You might also like
- Female GenitaliaDocument96 pagesFemale GenitaliaJopaii TanakaNo ratings yet
- Incompetent CervixDocument29 pagesIncompetent CervixCyrelle Jen TorresNo ratings yet
- POP June 10,2021 1Document48 pagesPOP June 10,2021 1Kerod AbebeNo ratings yet
- Gynecology: 3.09 - AmenorrheaDocument13 pagesGynecology: 3.09 - AmenorrheaAnna Mae MarantanNo ratings yet
- Abnormal Uterine BleedingDocument29 pagesAbnormal Uterine BleedingJed Mostajo100% (2)
- BreechDocument1 pageBreechZiyadNo ratings yet
- Pemphigus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPemphigus, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 2 - Anatomy and Histology of Female Genital TractDocument26 pages2 - Anatomy and Histology of Female Genital TractHervis FantiniNo ratings yet
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Diseases of Vulva MCQDocument6 pagesDiseases of Vulva MCQCommunity Round3 G1100% (1)
- Endometriosis Diet Plan: A Beginner's 3-Week Step-by-Step Guide for Women, With Curated Recipes and a Sample Meal PlanFrom EverandEndometriosis Diet Plan: A Beginner's 3-Week Step-by-Step Guide for Women, With Curated Recipes and a Sample Meal PlanNo ratings yet
- Human Reproductive SystemDocument4 pagesHuman Reproductive SystemGoal Digger Squad VlogNo ratings yet
- Harel 2012Document14 pagesHarel 2012auliaNo ratings yet
- Puerperal Sepsis and Abnormalities of PuerperiumDocument10 pagesPuerperal Sepsis and Abnormalities of PuerperiumMaikka IlaganNo ratings yet
- Disordered Proliferative Endometrium Causes and SymptomsDocument7 pagesDisordered Proliferative Endometrium Causes and SymptomsMuhammad BabarNo ratings yet
- Jsafog 11 23Document4 pagesJsafog 11 23nanamy kesNo ratings yet
- RH Incompatibility Resource UnitDocument6 pagesRH Incompatibility Resource UnitJannah Marie A. DimaporoNo ratings yet
- CELLE DismenorreaDocument7 pagesCELLE DismenorreaJose Vergara GNo ratings yet
- AUBF Amniotic FluidDocument6 pagesAUBF Amniotic FluidRichelyn Grace B. VenusNo ratings yet
- Lesson Plan Infertility .Document23 pagesLesson Plan Infertility .Naresh JarwalNo ratings yet
- Slides Mullerian AnomaliesDocument29 pagesSlides Mullerian AnomaliesAsunción AncoNo ratings yet
- Sign - Symptom AND Management of Severe MalnutritionDocument62 pagesSign - Symptom AND Management of Severe MalnutritionTiara KhairinaNo ratings yet
- Management of Primary Dysmenorrhoea by Dry Cupping: A ReviewDocument5 pagesManagement of Primary Dysmenorrhoea by Dry Cupping: A ReviewWilyanto YangNo ratings yet
- Artic Carcinoma Endometrial 2021Document12 pagesArtic Carcinoma Endometrial 2021Fabiola Milagros Castillo LlicaNo ratings yet
- Case Study 4Document10 pagesCase Study 4Dyan Bianca Suaso LastimosaNo ratings yet
- Optimizing Fertility Using Functional MedicineDocument68 pagesOptimizing Fertility Using Functional MedicinerachNo ratings yet
- Bezuidenhout 2018 DysmenorrhoeaanoverviewDocument6 pagesBezuidenhout 2018 Dysmenorrhoeaanoverviewcarladabboura79No ratings yet
- Disorders of The Vagina and CervixDocument4 pagesDisorders of The Vagina and CervixLOUISE VENICE PEREZ CIDNo ratings yet
- Breast Fibroadenomas in Adolescents CurrentDocument5 pagesBreast Fibroadenomas in Adolescents CurrentEvediciNo ratings yet
- Jurnal Pendukung Data DisminoreDocument8 pagesJurnal Pendukung Data DisminorePuput AnggarNo ratings yet
- Diagnostic Tests For EndometriosisDocument2 pagesDiagnostic Tests For EndometriosisApril Kirstin ChuaNo ratings yet
- Diagnosing Endometriosis MO 18aug15 PDFDocument1 pageDiagnosing Endometriosis MO 18aug15 PDFRifki Hilman FauziNo ratings yet
- Endometriossis and DepresiDocument8 pagesEndometriossis and Depresibobbyrianto2210No ratings yet
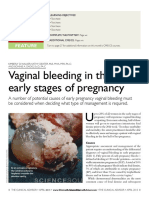
- CME CE: Vaginal Bleeding in The Early Stages of PregnancyDocument7 pagesCME CE: Vaginal Bleeding in The Early Stages of PregnancyMiratunnisa AzzahrahNo ratings yet
- Dyspareunia in Climacteric Women: What Should We Know?: Mini ReviewDocument3 pagesDyspareunia in Climacteric Women: What Should We Know?: Mini RevieworienteNo ratings yet
- Incomplete Abortion Day 2Document25 pagesIncomplete Abortion Day 2Tricia Denise EstabilloNo ratings yet
- 8-Article Text-11-1-10-20200304 - 2Document4 pages8-Article Text-11-1-10-20200304 - 2Christopher RyalinoNo ratings yet
- EndometriosisDocument8 pagesEndometriosisMuhammadR1No ratings yet
- LP KEHAMILAN NORMAL Haidir (2) .Id - enDocument7 pagesLP KEHAMILAN NORMAL Haidir (2) .Id - enMuhammad ZainuddinNo ratings yet
- Ever Intriguing Primary Amenorrhea'-An Audit: January 2014Document8 pagesEver Intriguing Primary Amenorrhea'-An Audit: January 2014AgusNo ratings yet
- Clinicopathological Correlation of Endometrial, Myometrial and Ovarian Pathologies With Secondary Changes in LeiomyomaDocument5 pagesClinicopathological Correlation of Endometrial, Myometrial and Ovarian Pathologies With Secondary Changes in LeiomyomakushalNo ratings yet
- Sirenomelia A Case ReportDocument4 pagesSirenomelia A Case ReportAyanawNo ratings yet
- Study: Reduce Dymenorore Pain With Compress WarmDocument6 pagesStudy: Reduce Dymenorore Pain With Compress WarmTriNo ratings yet
- NCP - 110323Document4 pagesNCP - 110323designericlelynsoronioNo ratings yet
- Drug Study SyntometrineDocument2 pagesDrug Study Syntometrinerica sebabillonesNo ratings yet
- Vesicovaginal FistulaDocument54 pagesVesicovaginal FistuladanielNo ratings yet
- Drug Study FORMDocument2 pagesDrug Study FORMLovely heart AñanaNo ratings yet
- 2020.dysmenorrhea andDocument8 pages2020.dysmenorrhea andObgynism 2019No ratings yet
- NCMA 217 WK 2C MensDocument7 pagesNCMA 217 WK 2C MensABEGAIL BALLORANNo ratings yet
- Angka Kejadian DismenoreDocument9 pagesAngka Kejadian DismenorePutri KartiniNo ratings yet
- Congenital AnbnormalityDocument25 pagesCongenital Anbnormalityshivani dasNo ratings yet
- NCM 109 Problems With Power DraftDocument3 pagesNCM 109 Problems With Power DraftJP Porras AliNo ratings yet
- The Role of Epidemiology in Public HealthDocument19 pagesThe Role of Epidemiology in Public HealthGilbert LimenNo ratings yet
- Fertility and Infertility: The Purpose of Reproduction Students' WorksheetDocument9 pagesFertility and Infertility: The Purpose of Reproduction Students' WorksheetCristian RajagukgukNo ratings yet
- Labial Adhesion: Evaluation and ManagementDocument4 pagesLabial Adhesion: Evaluation and ManagementAnadya RhadikaNo ratings yet
- Faktor Yang Mempengaruhi Kejadian Dismenorea Pada Remaja Putri Kelas X Di MAN Rantauprapat Tahun 2021 Rika Handayani1Document17 pagesFaktor Yang Mempengaruhi Kejadian Dismenorea Pada Remaja Putri Kelas X Di MAN Rantauprapat Tahun 2021 Rika Handayani1Rika HandayaniNo ratings yet
- Mullerian MalformationsDocument6 pagesMullerian MalformationsMau JkjlNo ratings yet
- DINOPROSTONEDocument2 pagesDINOPROSTONEWemslaiNo ratings yet
- Alternative Methods of BirthDocument32 pagesAlternative Methods of BirthVictoriaNo ratings yet
- شيت اوبس وقايناDocument19 pagesشيت اوبس وقايناFares OsmanNo ratings yet
- Rle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyDocument6 pagesRle 107 Maternal and Child Health Nursing: University of The Assumption College of Nursing and PharmacyEvangeline Anne Macanas100% (2)
- Pcsoadolescent20202in1 200819164750Document24 pagesPcsoadolescent20202in1 200819164750JemalNo ratings yet
- Dela Cruz Mikee MarcosDocument1 pageDela Cruz Mikee MarcosIRISH GENEVIEVE DE VERANo ratings yet
- Sex Hormone-Binding Globulin (SHBG) As An Early Biomarker and Therapeutic Target in Polycystic Ovary SyndromeDocument17 pagesSex Hormone-Binding Globulin (SHBG) As An Early Biomarker and Therapeutic Target in Polycystic Ovary SyndromeFernando Silva RivasNo ratings yet
- Embryology of The Female Genital TractDocument11 pagesEmbryology of The Female Genital Tractzovi100% (1)
- Reproductive Health & Family PlanningDocument37 pagesReproductive Health & Family PlanningKerod AbebeNo ratings yet
- STD and PIDDocument42 pagesSTD and PIDKerod AbebeNo ratings yet
- Uterine Myoma, Sept, 2021Document63 pagesUterine Myoma, Sept, 2021Kerod AbebeNo ratings yet
- Cardiac & Respiratory Diseases in PregnancyDocument30 pagesCardiac & Respiratory Diseases in PregnancyKerod AbebeNo ratings yet
- Breast Care and Breast Feeding For CI, by DR Abera Sept 2021Document57 pagesBreast Care and Breast Feeding For CI, by DR Abera Sept 2021Kerod AbebeNo ratings yet
- Cephalopelvic Disproportion, Obstructed Lab Our, UterineDocument49 pagesCephalopelvic Disproportion, Obstructed Lab Our, UterineKerod AbebeNo ratings yet
- Diabetes in PregnancyDocument27 pagesDiabetes in PregnancyKerod AbebeNo ratings yet
- Abortion and Post-Abortion Care Abortion and Post-Abortion CareDocument48 pagesAbortion and Post-Abortion Care Abortion and Post-Abortion CareKerod AbebeNo ratings yet
- Female Condome How To UseDocument4 pagesFemale Condome How To UseRam Bahadur Saru100% (4)
- Uterine AbnormalityDocument8 pagesUterine AbnormalityberylianamayaNo ratings yet
- Grade 10 Reproductive HealthDocument26 pagesGrade 10 Reproductive HealthMissy BanguisNo ratings yet
- 3-1 Female Anatomy - Full ScreenDocument30 pages3-1 Female Anatomy - Full ScreenfiazNo ratings yet
- GIN 2 IAN 28.01.2020 FixDocument7 pagesGIN 2 IAN 28.01.2020 FixRyan IlhamNo ratings yet
- Pathophysiology of HysterectomyDocument5 pagesPathophysiology of HysterectomyJORINA PUMIHICNo ratings yet
- Gyne - Case 11 Lower Genital UTI PDFDocument2 pagesGyne - Case 11 Lower Genital UTI PDFcbac1990No ratings yet
- Information For You: Pelvic Organ ProlapseDocument8 pagesInformation For You: Pelvic Organ Prolapsesandeepv08No ratings yet
- Abnormal Vaginal BleedingDocument2 pagesAbnormal Vaginal BleedingPrincess Gee OdanNo ratings yet
- Ovarian Torsion in Pregnancy A Case ReportDocument3 pagesOvarian Torsion in Pregnancy A Case ReportCakraEkkyNo ratings yet
- Entrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDocument2 pagesEntrapment of A Vaginal Ring Pessary - Case Report and Review of The LiteratureDR RISKA WAHYUNo ratings yet
- Leiomyoma - What Is It? Pathogenesis, Clinical Presentation, Diagnosis, HysterectomyDocument10 pagesLeiomyoma - What Is It? Pathogenesis, Clinical Presentation, Diagnosis, HysterectomyRida ArifNo ratings yet
- CHAPTER 8 - Abnormal Uterine BleedingDocument42 pagesCHAPTER 8 - Abnormal Uterine BleedingJesselyn ReginaNo ratings yet
- Sistem Reproduksi Wanita-Uswatun Hasanah 195037Document13 pagesSistem Reproduksi Wanita-Uswatun Hasanah 195037Uswatun HasanahNo ratings yet
- Abstract Publication ESGE28thAnnualCongress 2019 FinalDocument446 pagesAbstract Publication ESGE28thAnnualCongress 2019 FinalNina ThieleNo ratings yet
- Mri Station Synechiae Vagina 30 September 2021Document36 pagesMri Station Synechiae Vagina 30 September 2021diniNo ratings yet
- Gynecologic-Nursing Part 1Document33 pagesGynecologic-Nursing Part 1jomariNo ratings yet
- I.Objective: Ii - Subject Matter:: Science 5Document2 pagesI.Objective: Ii - Subject Matter:: Science 5Yvette LeonidaNo ratings yet
- Ovarian Cyst: Ovary Ovarian Follicle Centimeters Pea BenignDocument3 pagesOvarian Cyst: Ovary Ovarian Follicle Centimeters Pea BenignSyazwana AnaNo ratings yet
- Reproduction System Terminology QuizDocument6 pagesReproduction System Terminology QuizIrams KitchenNo ratings yet
- Abnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarDocument80 pagesAbnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarSharoon KumarNo ratings yet
- These Are Not Recalls-If You Know What I MeanDocument3 pagesThese Are Not Recalls-If You Know What I MeanFareesha KhanNo ratings yet
- Note: Refer To The Structures Above and Familiarize The Functions of Each PartsDocument2 pagesNote: Refer To The Structures Above and Familiarize The Functions of Each PartsRam August100% (1)
- Flour AlbusDocument26 pagesFlour AlbusPengeran Al-fikriNo ratings yet
- Introduction of Insemination Intra Uterine: Dicky Moch RizalDocument19 pagesIntroduction of Insemination Intra Uterine: Dicky Moch RizalRobeth EriaNo ratings yet