You might also like
- Hydioic AcidDocument55 pagesHydioic AcidJamie Lynn Peters Taylor67% (12)
- Guide For Stop Using MethDocument16 pagesGuide For Stop Using MethDaniel Waluyo Sejati100% (2)
- Systematic Review Springer 2020 PDFDocument188 pagesSystematic Review Springer 2020 PDFArin Ghassani100% (5)
- (Mebooksfree Net) Pra&man&exp&cli&pha&med&pra&1st PDFDocument390 pages(Mebooksfree Net) Pra&man&exp&cli&pha&med&pra&1st PDFI. Elias Aguilera Vaca100% (1)
- Meth Overdose HelpDocument1 pageMeth Overdose HelpWfmy TegnaNo ratings yet
- Bailey 2002Document7 pagesBailey 2002Ayelen GaldeanoNo ratings yet
- Effect of Methamphetamine On CardiacDocument27 pagesEffect of Methamphetamine On CardiacABDALLANo ratings yet
- Mephedrone Pharmacokinetics After Intravenous and Oral Administration in Rats: Relation To PharmacodynamicsDocument23 pagesMephedrone Pharmacokinetics After Intravenous and Oral Administration in Rats: Relation To PharmacodynamicsReal GuruNo ratings yet
- The Ugly Side of Amphetamines: Short-And Long-Term Toxicity of 3,4-Methylenedioxymethamphetamine (MDMA, Ecstasy'), Methamphetamine and - AmphetamineDocument14 pagesThe Ugly Side of Amphetamines: Short-And Long-Term Toxicity of 3,4-Methylenedioxymethamphetamine (MDMA, Ecstasy'), Methamphetamine and - AmphetamineNocturnal PulseNo ratings yet
- Anaesthesia & Intensive Care Medicine Volume 14 Issue 3 2013 (Doi 10.1016/j.mpaic.2013.01.006) Hawthorne, Christopher Sutcliffe, Nick - Total Intravenous Anaesthesia PDFDocument3 pagesAnaesthesia & Intensive Care Medicine Volume 14 Issue 3 2013 (Doi 10.1016/j.mpaic.2013.01.006) Hawthorne, Christopher Sutcliffe, Nick - Total Intravenous Anaesthesia PDFAnonymous nbU88FeNo ratings yet
- Trichloroethylene Hazard Summary and UsesDocument5 pagesTrichloroethylene Hazard Summary and UsesC MNo ratings yet
- Half LifeDocument6 pagesHalf LifeDr. Mushfique Imtiaz ChowdhuryNo ratings yet
- Jurnal Yang DigunakanDocument6 pagesJurnal Yang DigunakanTrisna Trisna TrisnaNo ratings yet
- All Products MSDSDocument143 pagesAll Products MSDSkuldeepchahal1987No ratings yet
- Paper 2Document9 pagesPaper 2yadira toazaNo ratings yet
- Employ FTIR Spectroscopic Method For Determination of Certain Multiple Sclerosis Medications in Plasma and Pharmaceutical FormulationsDocument6 pagesEmploy FTIR Spectroscopic Method For Determination of Certain Multiple Sclerosis Medications in Plasma and Pharmaceutical FormulationsKarina CordovaNo ratings yet
- IV Inggris IpitDocument6 pagesIV Inggris Ipittutorial desatuNo ratings yet
- TMP CADBDocument9 pagesTMP CADBFrontiersNo ratings yet
- 2001 Rothman 1 PDFDocument10 pages2001 Rothman 1 PDFRoman SassNo ratings yet
- Liver and neurological effects of 1,1,2,2-TetrachloroethaneDocument5 pagesLiver and neurological effects of 1,1,2,2-TetrachloroethaneMali teaNo ratings yet
- MethamphetamineDocument7 pagesMethamphetaminerashikarema17No ratings yet
- Prini 2018Document15 pagesPrini 2018tiziana rubinoNo ratings yet
- Artigo Samuel ValençaDocument5 pagesArtigo Samuel ValençaKleber DennisNo ratings yet
- 3-Fluoromethcathinone, A Structural Analog of Mephedrone - Siedlecka-Kroplewska - Journal of Physiology and Pharmacology 64 (2014)Document6 pages3-Fluoromethcathinone, A Structural Analog of Mephedrone - Siedlecka-Kroplewska - Journal of Physiology and Pharmacology 64 (2014)dextroenantiomerNo ratings yet
- Tacrine Induce Hepatotoksik PDFDocument9 pagesTacrine Induce Hepatotoksik PDFItamahYulaikhaNo ratings yet
- Anaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiaDocument3 pagesAnaesthesia & Intensive Care Medicine Volume 11 Issue 4 2010 (Doi 10.1016/j.mpaic.2009.12.013) Ben Shelley Nick Sutcliffe - Total Intravenous AnaesthesiamikhatiarNo ratings yet
- Pentachlorophenol Hazard SummaryDocument5 pagesPentachlorophenol Hazard SummaryAyuNo ratings yet
- Featured Article: Is Dextromethorphan A Concern For Causing A False Positive During Urine Drug Screening?Document4 pagesFeatured Article: Is Dextromethorphan A Concern For Causing A False Positive During Urine Drug Screening?Cut Nyak Ilma AsyuraNo ratings yet
- Methamphetamine Dysregulation of The Central Nervous System InglesDocument14 pagesMethamphetamine Dysregulation of The Central Nervous System InglesElor TorrotoNo ratings yet
- (14796805 - Journal of Endocrinology) The Role of Corticotropin-Releasing Factor in Depression and Anxiety DisordersDocument12 pages(14796805 - Journal of Endocrinology) The Role of Corticotropin-Releasing Factor in Depression and Anxiety Disorderskaren Daniela Puma FarinangoNo ratings yet
- Chapter 165: Effects of Toxic Agents Leonard P. Rybak, Gregory J. MatzDocument26 pagesChapter 165: Effects of Toxic Agents Leonard P. Rybak, Gregory J. MatzbudiceriaNo ratings yet
- Tryptophane-Kynurenine Pathway in The Remote Ischemic Conditioning MechanismDocument8 pagesTryptophane-Kynurenine Pathway in The Remote Ischemic Conditioning MechanismSol SolNo ratings yet
- Therapeutic Drug Monitoring Part 2 PDFDocument23 pagesTherapeutic Drug Monitoring Part 2 PDFChandra AvicennaNo ratings yet
- Basic PharmacokineticsDocument131 pagesBasic PharmacokineticsSyeda Ayesha FarhanaNo ratings yet
- Conteúdos de Semiologia MedicinaDocument10 pagesConteúdos de Semiologia MedicinaCRISLLEY MULBAUERNo ratings yet
- The Gut Microbiota-Derived Metabolite Trimethylamine N-Oxide Is Elevated in Alzheimer 'S DiseaseDocument8 pagesThe Gut Microbiota-Derived Metabolite Trimethylamine N-Oxide Is Elevated in Alzheimer 'S DiseaseVitor PereiraNo ratings yet
- Ejm 19483 Original - Article Erdogmus - OzgenDocument6 pagesEjm 19483 Original - Article Erdogmus - OzgenArya GuganNo ratings yet
- Theobromine Inhibits CoughDocument16 pagesTheobromine Inhibits CoughRaffaello MobiliaNo ratings yet
- Endocrine System Pathology PPT Lecture SeriesDocument285 pagesEndocrine System Pathology PPT Lecture SeriesMarc Imhotep Cray, M.D.100% (6)
- Research Article Quetiapine Nanoemulsion For Intranasal Drug Delivery: Evaluation of Brain-Targeting EfficiencyDocument11 pagesResearch Article Quetiapine Nanoemulsion For Intranasal Drug Delivery: Evaluation of Brain-Targeting EfficiencyDeepak GuptaNo ratings yet
- Drug Metab Dispos 2003 James 1499 506Document8 pagesDrug Metab Dispos 2003 James 1499 506Cecilia Nanik WidjajatiNo ratings yet
- Anti EpilepticDocument13 pagesAnti EpilepticArbiati RahmanNo ratings yet
- Influence of Route on Drug Metabolite ProfilesDocument10 pagesInfluence of Route on Drug Metabolite ProfilesIstiqomah KalallaNo ratings yet
- Two New Pterocarpans and A New Pyrone Drivative With Cytoxic Activies FromDocument8 pagesTwo New Pterocarpans and A New Pyrone Drivative With Cytoxic Activies FromFilza Qurrota 'AiniNo ratings yet
- Effects of Repeated Treatment With Methcathinone, Mephedrone, and Fenfluramine On Intracranial Self-Stimulation in RatsDocument10 pagesEffects of Repeated Treatment With Methcathinone, Mephedrone, and Fenfluramine On Intracranial Self-Stimulation in RatsMariana MadiaNo ratings yet
- Role of The Parasympathetic Nervous System in Cancer Initiation and ProgressionDocument13 pagesRole of The Parasympathetic Nervous System in Cancer Initiation and ProgressionEquilibrium EduardoNo ratings yet
- Principles of Local Drug Delivery To The Inner EarDocument11 pagesPrinciples of Local Drug Delivery To The Inner Eararina windri rivartiNo ratings yet
- Postmortem Drug RedistributionDocument10 pagesPostmortem Drug RedistributionZeba NiazNo ratings yet
- Procainamide Hydrochloride: Major UseDocument3 pagesProcainamide Hydrochloride: Major UseDosi SiliNo ratings yet
- Pharmaco DynamicsDocument2 pagesPharmaco DynamicsSunil DeshpandeNo ratings yet
- Toxicology and Applied PharmacologyDocument11 pagesToxicology and Applied Pharmacologylaura EstaloteNo ratings yet
- 2020 Article 479Document5 pages2020 Article 479Anida HasnaNo ratings yet
- Biomedicines: Pituitary Adenomas: From Diagnosis To TherapeuticsDocument18 pagesBiomedicines: Pituitary Adenomas: From Diagnosis To TherapeuticsTavili J NetiviliNo ratings yet
- Figure 9-4: PharmacokineticsDocument12 pagesFigure 9-4: PharmacokineticsReni Wahyu NoviantiNo ratings yet
- Pilhatsch 2011Document7 pagesPilhatsch 2011omar rodriguezNo ratings yet
- Extracorporeal Membrane Oxygenation For Refractory Cardiac Arrest: A Retrospective Multicenter StudyDocument10 pagesExtracorporeal Membrane Oxygenation For Refractory Cardiac Arrest: A Retrospective Multicenter StudyFraternity LiviNo ratings yet
- Wang Et Al. (1999)Document5 pagesWang Et Al. (1999)Jay CHANNo ratings yet
- Effect of Perfl Uorohexane On The Expression of Cellular Adhesion Molecules and Surfactant Protein A in Human Mesothelial Cells in VitroDocument9 pagesEffect of Perfl Uorohexane On The Expression of Cellular Adhesion Molecules and Surfactant Protein A in Human Mesothelial Cells in VitroIstván PortörőNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- DARK Classics in Chemical Neuroscience: Methamphetamine: Thomas J. Abbruscato and Paul C. TrippierDocument6 pagesDARK Classics in Chemical Neuroscience: Methamphetamine: Thomas J. Abbruscato and Paul C. Trippier943909No ratings yet
- TMP 6 EF0Document6 pagesTMP 6 EF0FrontiersNo ratings yet
- Section3 THC ToxicologyDocument14 pagesSection3 THC ToxicologyCentenoCornezuelodelGuillermoNo ratings yet
- Regulation of Adhesion Molecules During Human Endotoxemia: No Acute Effects of AspirinDocument7 pagesRegulation of Adhesion Molecules During Human Endotoxemia: No Acute Effects of AspirinPablo VélezNo ratings yet
- Histopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationFrom EverandHistopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationNo ratings yet
- International Review of Experimental Pathology: Kidney DiseaseFrom EverandInternational Review of Experimental Pathology: Kidney DiseaseG. W. RichterRating: 5 out of 5 stars5/5 (1)
- Nutraceutical and Pharmacological Implications of Marine CarbohydrateDocument13 pagesNutraceutical and Pharmacological Implications of Marine CarbohydrateHajrah SuhardiNo ratings yet
- Manual of Laboratory Animals Basic Facilities, Handling and CareDocument24 pagesManual of Laboratory Animals Basic Facilities, Handling and CareHajrah SuhardiNo ratings yet
- Pharmacokinetics and Pharmacodynamics of The Proton Pump InhibitorsDocument11 pagesPharmacokinetics and Pharmacodynamics of The Proton Pump InhibitorsHadiNugrahaNo ratings yet
- Emulsion Micro Emulsion and Nano Emulsion: A ReviewDocument9 pagesEmulsion Micro Emulsion and Nano Emulsion: A ReviewHajrah SuhardiNo ratings yet
- Migraine A Summary of Existing Guidelines For UseDocument9 pagesMigraine A Summary of Existing Guidelines For UseHajrah SuhardiNo ratings yet
- Nutraceutical Functions of Cumin (Cuminum Cyminum L)Document11 pagesNutraceutical Functions of Cumin (Cuminum Cyminum L)Hajrah SuhardiNo ratings yet
- Nutraceutical antioxidants in neuroprotection and anti-cancer therapyDocument85 pagesNutraceutical antioxidants in neuroprotection and anti-cancer therapyHajrah SuhardiNo ratings yet
- World TB Day 2016 Presentations 1 520688 7Document69 pagesWorld TB Day 2016 Presentations 1 520688 7georgeNo ratings yet
- Nutraceutical Functions of Cumin (Cuminum Cyminum L)Document11 pagesNutraceutical Functions of Cumin (Cuminum Cyminum L)Hajrah SuhardiNo ratings yet
- Jurnal Microbiome-Tuberculosis-BiomolecularDocument24 pagesJurnal Microbiome-Tuberculosis-BiomolecularNurul Annisa MuthaharaNo ratings yet
- Evaluation of Broth Microdilution Antifungal Susceptibility TestingDocument4 pagesEvaluation of Broth Microdilution Antifungal Susceptibility TestingHajrah SuhardiNo ratings yet
- Evolution of Antifungal PDFDocument10 pagesEvolution of Antifungal PDFHajrah SuhardiNo ratings yet
- Pathogenesis of Post Primary Tuberculosis: Immunity and Hypersensitivity in The Development of CavitiesDocument24 pagesPathogenesis of Post Primary Tuberculosis: Immunity and Hypersensitivity in The Development of CavitiesHajrah SuhardiNo ratings yet
- Impairment of Liver Function Tests and Lipid Profiles in Type Diabetic Patients Treated at The Diabetic Center in Tikur Anbessa 2155 6156.1000454Document7 pagesImpairment of Liver Function Tests and Lipid Profiles in Type Diabetic Patients Treated at The Diabetic Center in Tikur Anbessa 2155 6156.1000454Hajrah SuhardiNo ratings yet
- Evolution of Antifungal PDFDocument10 pagesEvolution of Antifungal PDFHajrah SuhardiNo ratings yet
- A Novel Coculture Model For Benign Prostatic PDFDocument8 pagesA Novel Coculture Model For Benign Prostatic PDFHajrah SuhardiNo ratings yet
- 2010a-Stem Cells (Ming)Document20 pages2010a-Stem Cells (Ming)Hajrah SuhardiNo ratings yet
- Potency of Lobak Leaves As Anticancer PDFDocument5 pagesPotency of Lobak Leaves As Anticancer PDFHajrah SuhardiNo ratings yet
- A 10-Year Survey of Antifungal Susceptibility of CandidemiaDocument3 pagesA 10-Year Survey of Antifungal Susceptibility of CandidemiaHajrah SuhardiNo ratings yet
- Comparison of A Photometric Method With StandardizedDocument5 pagesComparison of A Photometric Method With StandardizedHajrah SuhardiNo ratings yet
- Ball Hyperplasia PDFDocument7 pagesBall Hyperplasia PDFHajrah SuhardiNo ratings yet
- Ipi 270583Document8 pagesIpi 270583NasruddinNo ratings yet
- Antimicrob. Agents Chemother. 1998 Klepser 1207 12Document7 pagesAntimicrob. Agents Chemother. 1998 Klepser 1207 12Hajrah SuhardiNo ratings yet
- 2009 8 4 12 DulgerDocument5 pages2009 8 4 12 DulgerHajrah SuhardiNo ratings yet
- Time of Incubation For Antifungal Susceptibility Testing ofDocument3 pagesTime of Incubation For Antifungal Susceptibility Testing ofHajrah SuhardiNo ratings yet
- Use of The Sensititre Colorimetric Microdilution Panel For AntifungalDocument4 pagesUse of The Sensititre Colorimetric Microdilution Panel For AntifungalHajrah SuhardiNo ratings yet
- Antibacterial Activity of Pterocarpus IndicusDocument3 pagesAntibacterial Activity of Pterocarpus IndicusHajrah SuhardiNo ratings yet
- Qa Cdi 3Document28 pagesQa Cdi 3AIRRAH LACANARIANo ratings yet
- National Service Training Program 1 Module 10: Drug Abuse and PreventionDocument1 pageNational Service Training Program 1 Module 10: Drug Abuse and PreventionKristine PangahinNo ratings yet
- MAPEH 9 Q2 Week 4 HealthDocument8 pagesMAPEH 9 Q2 Week 4 HealthMhark Adrian FernandezNo ratings yet
- DRUGS and DRUG ADDICTIONDocument67 pagesDRUGS and DRUG ADDICTIONMarcus Nikolai Gibb AxeNo ratings yet
- Crystal Methamphetamine FactsDocument5 pagesCrystal Methamphetamine Factsdirtyunderdog520100% (1)
- Judy Wigmore Newsbreak 05Document8 pagesJudy Wigmore Newsbreak 05uncleadolphNo ratings yet
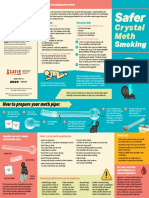
- CATIE SaferSmoking CrystalMeth E 2020 FINAL WEBDocument2 pagesCATIE SaferSmoking CrystalMeth E 2020 FINAL WEBJeff PuglisiNo ratings yet
- Jasco Applications Book CD and PolarimetersDocument62 pagesJasco Applications Book CD and PolarimetersDan Pantoș100% (1)
- Drug Situationer LectureDocument69 pagesDrug Situationer LectureJane DizonNo ratings yet
- Grounds for Annulment of Marriage in the Philippines ExplainedDocument3 pagesGrounds for Annulment of Marriage in the Philippines ExplainedStian Jay YpnNo ratings yet
- Test Bank For Drugs Behaviour and Society Canadian Edition Carl Hart DownloadDocument24 pagesTest Bank For Drugs Behaviour and Society Canadian Edition Carl Hart Downloadmeganyoungebnmofkysx100% (47)
- MAPEH 9 Second GradingDocument9 pagesMAPEH 9 Second GradingSittie Rahma AlawiNo ratings yet
- RESEARCHDocument6 pagesRESEARCHReimar QuiambaoNo ratings yet
- NSTP Outline For ExamDocument6 pagesNSTP Outline For Exammaricar nunezNo ratings yet
- NSTP ReviewerDocument18 pagesNSTP ReviewerKrystel TullaoNo ratings yet
- P121.M3.Substance Related DisordersDocument33 pagesP121.M3.Substance Related Disordersgwen awasNo ratings yet
- Meth Anonymous ExperienceDocument7 pagesMeth Anonymous ExperienceJayson KarunaNo ratings yet
- Jurnal Data P4GN 2015 - Edisi 2016 - ENDocument228 pagesJurnal Data P4GN 2015 - Edisi 2016 - ENAnti NarkobaNo ratings yet
- "Speed-Balling": Mixing Stimulants and Opioids: MicromoduleDocument40 pages"Speed-Balling": Mixing Stimulants and Opioids: MicromoduleHigor ChamaneNo ratings yet
- Forensics ManualDocument227 pagesForensics ManualWilfredo P. Sudio, Jr.No ratings yet
- Addiction Science: From Molecules To Managed CareDocument75 pagesAddiction Science: From Molecules To Managed Carenidaebooks0% (1)
- Amelita Sari PDFDocument13 pagesAmelita Sari PDFJonel NaquitaNo ratings yet
- CM - 008 - NSTP1 - Drug EducationDocument36 pagesCM - 008 - NSTP1 - Drug EducationVher Christopher DucayNo ratings yet
- 001 G.R. No. 121345Document3 pages001 G.R. No. 121345Paul ToguayNo ratings yet
- Strategic Planning and The Drug Threat Pub318Document185 pagesStrategic Planning and The Drug Threat Pub318scparcoNo ratings yet
- Narcotic DrugsDocument53 pagesNarcotic DrugsAl Vincent0% (1)
- Illegal DrugsDocument5 pagesIllegal DrugsJOCELYN VARGASNo ratings yet