You might also like
- Alt - Cancer (1) BookDocument419 pagesAlt - Cancer (1) Bookniceia matos100% (3)
- Contractor Safety ManualDocument145 pagesContractor Safety Manualdaladar2008No ratings yet
- Common Medical Abbreviations With MeaningsDocument16 pagesCommon Medical Abbreviations With MeaningsWilliam Franz SyNo ratings yet
- Coronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentFrom EverandCoronavirus: Arm Yourself With Facts: Symptoms, Modes of Transmission, Prevention & TreatmentRating: 5 out of 5 stars5/5 (1)
- Dengue Fever Case StudyDocument55 pagesDengue Fever Case StudyGlory Holmes67% (6)
- Redeemer'S Basic School, Yola 3Rd Term Examination Subject: Phe Class: Jss2 Duration: 1 HourDocument3 pagesRedeemer'S Basic School, Yola 3Rd Term Examination Subject: Phe Class: Jss2 Duration: 1 HourRBS RISSNo ratings yet
- Nutrition QuestionnaireDocument4 pagesNutrition QuestionnaireNitya Krishna100% (1)
- Learning ObjectivesDocument6 pagesLearning Objectivesangot123No ratings yet
- Dengvaxia VaccineDocument8 pagesDengvaxia VaccineBayek NgekekNo ratings yet
- WHO Position Paper Dengue 2016 ReferencesDocument17 pagesWHO Position Paper Dengue 2016 Referencessingularity24601_302No ratings yet
- Practiva No 3 Anova Serrano 2017Document7 pagesPractiva No 3 Anova Serrano 2017CARLOS DIONEY MOLINA CLEMENTENo ratings yet
- Dengue LancetDocument16 pagesDengue LancetJorge Ricardo Uchuya GómezNo ratings yet
- Paper FataldengueDocument19 pagesPaper FataldengueaidsariveraNo ratings yet
- Dengue (Lancet)Document16 pagesDengue (Lancet)Roberth Mero100% (1)
- Review of Literature On Dengue Fever in IndiaDocument9 pagesReview of Literature On Dengue Fever in Indial1wot1j1fon3100% (1)
- Dengue 1Document10 pagesDengue 1Ramón Pardo VillafrancaNo ratings yet
- 1 s2.0 S2667193X2100137X MainDocument9 pages1 s2.0 S2667193X2100137X MainTrhiana FuentesNo ratings yet
- Maternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoDocument8 pagesMaternal, Fetal, and Neonatal Outcomes in Pregnant Dengue Patients in MexicoLola del carmen RojasNo ratings yet
- 2016 Article 1668Document7 pages2016 Article 1668Rahmiati LaoNo ratings yet
- 1 s2.0 S1473309916000268 MainDocument12 pages1 s2.0 S1473309916000268 MainLachlan PetersonNo ratings yet
- 8d9c PDFDocument11 pages8d9c PDFJulian AshbourneNo ratings yet
- Title: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruDocument20 pagesTitle: Seroprevalence of Anti-Sars-Cov-2 Antibodies in Iquitos, Loreto, PeruCésar LópezNo ratings yet
- AsdsfDocument6 pagesAsdsfvirta andhikaNo ratings yet
- Research Paper On Dengue Fever in PakistanDocument6 pagesResearch Paper On Dengue Fever in Pakistangvzz4v44100% (1)
- Diaz Quijano Determinants DengueMortality Tropmed 86 328Document7 pagesDiaz Quijano Determinants DengueMortality Tropmed 86 328F Alexander Diaz-QuijanoNo ratings yet
- IVERMECTINA-NO-TRATAMENTO-DA-DENGUEDocument18 pagesIVERMECTINA-NO-TRATAMENTO-DA-DENGUEuchoaNo ratings yet
- Epidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudyDocument9 pagesEpidemiological Risk Factors For Adult Dengue in Singapore: An 8-Year Nested Test Negative Case Control StudydouwesdNo ratings yet
- WHO Dengue Bulletin Vol 24 Dec 2000Document3 pagesWHO Dengue Bulletin Vol 24 Dec 2000Tapojyoti DasNo ratings yet
- Research Paper On h1n1 VirusDocument5 pagesResearch Paper On h1n1 Viruszijkchbkf100% (1)
- Research Paper On Dengue VirusDocument6 pagesResearch Paper On Dengue Virusfvgy6fn3100% (1)
- Vaccine: Pablo Wenceslao Orellano, Julieta Itati Reynoso, Hans-Christian Stahl, Oscar Daniel SalomonDocument6 pagesVaccine: Pablo Wenceslao Orellano, Julieta Itati Reynoso, Hans-Christian Stahl, Oscar Daniel SalomonrahayuNo ratings yet
- Fimmu 05 00280Document10 pagesFimmu 05 00280Analia UrueñaNo ratings yet
- CLN 71 08 455Document9 pagesCLN 71 08 455Ranny Yovita MaharaniNo ratings yet
- Journal LeticiaDocument12 pagesJournal LeticiaDewi KUNo ratings yet
- Data Analysis Plan On The Association Between Socio Economic and Demographic Factors and Dengue Fever Infection PDFDocument8 pagesData Analysis Plan On The Association Between Socio Economic and Demographic Factors and Dengue Fever Infection PDFKeshab RijalNo ratings yet
- Tropmed 91 1002Document9 pagesTropmed 91 1002Khalifah Future LearningNo ratings yet
- Sitasi Jurnal 4Document8 pagesSitasi Jurnal 4ninikNo ratings yet
- Dengue Virus Research PaperDocument7 pagesDengue Virus Research Paperafnhicafcspyjh100% (1)
- Dengue Virus ThesisDocument7 pagesDengue Virus Thesisafjvbpvce100% (1)
- Spatial Analysis of Hospitalized Dengue Patients in Cabanatuan City: Demographics and RiskDocument11 pagesSpatial Analysis of Hospitalized Dengue Patients in Cabanatuan City: Demographics and RiskIJAERS JOURNALNo ratings yet
- Prevalence and Incidence of Dengue Virus and Antibody Placental Transfer During Late Pregnancy in Central BrazilDocument7 pagesPrevalence and Incidence of Dengue Virus and Antibody Placental Transfer During Late Pregnancy in Central Brazilrgutierrez1722No ratings yet
- Burden of DengueDocument12 pagesBurden of DengueChairut ChampoonoteNo ratings yet
- Fritzell2018 PDFDocument29 pagesFritzell2018 PDFJuan Fernando BermúdezNo ratings yet
- Dengue in Latin AmericaDocument19 pagesDengue in Latin AmericaCarolina Neciosup TullumeNo ratings yet
- Upward Trend in Hospitalized Dengue Cases in the United StatesDocument6 pagesUpward Trend in Hospitalized Dengue Cases in the United StatesArhaMozaNo ratings yet
- Down Syndrome and The Risk of Severe RSV Infection - A Meta-Analysis CHDocument10 pagesDown Syndrome and The Risk of Severe RSV Infection - A Meta-Analysis CHMaria Gratzia OrdoñezNo ratings yet
- Estimating Dengue Transmission Intensity From Case-Notification Data From Multiple CountriesDocument15 pagesEstimating Dengue Transmission Intensity From Case-Notification Data From Multiple CountriesMario LNo ratings yet
- Dengue FeverDocument15 pagesDengue FeverWawa ManNo ratings yet
- Clinical Characteristics of Norovirus-Associated Deaths A Systematic Literature ReviewDocument4 pagesClinical Characteristics of Norovirus-Associated Deaths A Systematic Literature ReviewafmzvjvjzoeqtgNo ratings yet
- J Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressDocument3 pagesJ Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressRaja Ahmad Rusdan MusyawirNo ratings yet
- International Journal of Infectious Diseases: G.G. SimonDocument4 pagesInternational Journal of Infectious Diseases: G.G. Simonlucasdesouza2No ratings yet
- The Problem and Its ScopeDocument59 pagesThe Problem and Its ScopeRochelle GallofinNo ratings yet
- The Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Document11 pagesThe Rise of Imported Dengue Infections in Victoria, Australia, 2010-2016Satriya WibawaNo ratings yet
- Jose Research v2Document10 pagesJose Research v2Jose Emmanuel FranciaNo ratings yet
- Assessing The Burden of Dengue Among Household Members in Alaminos Laguna The Philippines A Prospective Cohort StudyDocument10 pagesAssessing The Burden of Dengue Among Household Members in Alaminos Laguna The Philippines A Prospective Cohort Studyfigin86893No ratings yet
- Research Paper About Dengue FeverDocument5 pagesResearch Paper About Dengue Feveraflbskzqa100% (1)
- HealthcareDocument13 pagesHealthcareMaria Liliana Calderon MaciasNo ratings yet
- Risk Factors For Mortality in Patients With DengueDocument13 pagesRisk Factors For Mortality in Patients With DengueTaufiqurrokhman RofiiNo ratings yet
- Research Paper On Dengue FeverDocument5 pagesResearch Paper On Dengue Feverz1h1dalif0n3100% (1)
- A Review of Dengue Research in MalaysiaDocument9 pagesA Review of Dengue Research in MalaysiaAriff RazakNo ratings yet
- Laboratory Diagnosis of Dengue Infection: Current Techniques and Future StrategiesDocument9 pagesLaboratory Diagnosis of Dengue Infection: Current Techniques and Future StrategiesAndri YansyahNo ratings yet
- CDC 133479 DS1Document11 pagesCDC 133479 DS1tiata fitriNo ratings yet
- Epidemic Patterns of Dengue From 1980-2007Document3 pagesEpidemic Patterns of Dengue From 1980-2007api-272476883No ratings yet
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDocument14 pagesSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNo ratings yet
- COVID-19 in Clinical Practice: Lessons Learned and Future PerspectivesFrom EverandCOVID-19 in Clinical Practice: Lessons Learned and Future PerspectivesFlavio TangianuNo ratings yet
- Coronavirus Uncovered: What You Need to Know to Be ProtectedFrom EverandCoronavirus Uncovered: What You Need to Know to Be ProtectedNo ratings yet
- 44899-Article Text-170228-1-10-20220729Document6 pages44899-Article Text-170228-1-10-20220729Narulitha ririnNo ratings yet
- 29966-Article Text-75429-1-10-20190803Document8 pages29966-Article Text-75429-1-10-20190803Narulitha ririnNo ratings yet
- Pyruvat Transaminase Pada Serum Ikan Nila (Oreochromis Niloticus)Document6 pagesPyruvat Transaminase Pada Serum Ikan Nila (Oreochromis Niloticus)Narulitha ririnNo ratings yet
- PlagueDocument50 pagesPlagueSajad WaniNo ratings yet
- PlagueDocument50 pagesPlagueSajad WaniNo ratings yet
- 1460458216628312Document15 pages1460458216628312Narulitha ririnNo ratings yet
- Health and Demographic Surveillance System (HDSS) in Matlab, BangladeshDocument8 pagesHealth and Demographic Surveillance System (HDSS) in Matlab, BangladeshNarulitha ririnNo ratings yet
- Health & Demographic Surveillance System Profile: The Dikgale Health and Demographic Surveillance SystemDocument7 pagesHealth & Demographic Surveillance System Profile: The Dikgale Health and Demographic Surveillance SystemNarulitha ririnNo ratings yet
- Jurnal Hubungan Faktor Sosial Ekonomi Ibu HamilDocument10 pagesJurnal Hubungan Faktor Sosial Ekonomi Ibu HamilNarulitha ririnNo ratings yet
- Study Literatur: Pengkajian Luka Kaki DiabetesDocument15 pagesStudy Literatur: Pengkajian Luka Kaki DiabetesoctaviamayvikaNo ratings yet
- Q4 Module 4 Answer Health 10Document3 pagesQ4 Module 4 Answer Health 10Brian MirandaNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Biology InvestigatoryDocument6 pagesBiology InvestigatoryAananthan Jayvardan100% (2)
- Health and Skill Related Components of Physical FitnessDocument6 pagesHealth and Skill Related Components of Physical FitnessJovanne CabaluNo ratings yet
- How ergonomics improves employee performance and reduces costsDocument3 pagesHow ergonomics improves employee performance and reduces costsPradeep Dahiya100% (1)
- STUDENT KAP ON HIV/AIDSDocument22 pagesSTUDENT KAP ON HIV/AIDSbegosewNo ratings yet
- BPH treatment options and assessmentDocument7 pagesBPH treatment options and assessmentVon BellosilloNo ratings yet
- Nephrotic SyndromeDocument23 pagesNephrotic SyndromeDivina Francia JovenNo ratings yet
- Munjir Abdullah - Project On PBH101Document4 pagesMunjir Abdullah - Project On PBH101Munjir Abdullah 2112217030No ratings yet
- Career Day Brochure FinalDocument2 pagesCareer Day Brochure Finalapi-375229945No ratings yet
- Case 034: ConstipationDocument7 pagesCase 034: ConstipationZauza100% (1)
- Initation of Insulin - Final 2023Document27 pagesInitation of Insulin - Final 2023DEWI RIZKI AGUSTINANo ratings yet
- Efficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsDocument6 pagesEfficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsthiagoNo ratings yet
- 【课件】自然游戏治疗01场Document67 pages【课件】自然游戏治疗01场xjawyh0208No ratings yet
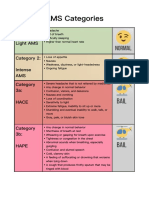
- AMS Symptoms and CategoriesDocument1 pageAMS Symptoms and CategoriesyyggvcNo ratings yet
- Reading Unit 3Document2 pagesReading Unit 3estefania aranda jimenezNo ratings yet
- Atos CFSDocument22 pagesAtos CFSPaul SmithNo ratings yet
- Trauma and Stressor-Related DisordersDocument58 pagesTrauma and Stressor-Related DisordersHamid Colangcag AmborNo ratings yet
- B. Bruce Myers, MD PHD FACSDocument5 pagesB. Bruce Myers, MD PHD FACSallison8844No ratings yet
- Salmodil Syrup: What Is in This LeafletDocument2 pagesSalmodil Syrup: What Is in This LeafletNadia SalwaniNo ratings yet
- Mere WaliDocument7 pagesMere WaliMaliCk TaimoorNo ratings yet
- Brunswick County 2022 Community Health Needs AssessmentDocument154 pagesBrunswick County 2022 Community Health Needs AssessmentJamie BouletNo ratings yet
- Motor Disturbance in ChildrenDocument84 pagesMotor Disturbance in ChildrenYuri BrosgolNo ratings yet