You might also like
- Bronchial AsthmaDocument71 pagesBronchial AsthmaHero MondaresNo ratings yet
- MedSurg Ch30-31Document8 pagesMedSurg Ch30-31Vanessa Da Cruz100% (1)
- Bronchial AsthmaDocument71 pagesBronchial AsthmaQuolette Constante100% (1)
- Case Analysis 4 GERDDocument12 pagesCase Analysis 4 GERDCJ100% (1)
- Physical Diagnoses: Respiratory SystemDocument72 pagesPhysical Diagnoses: Respiratory SystemAmanuel MaruNo ratings yet
- Care of A Child With RespiratoryDocument185 pagesCare of A Child With RespiratoryVanessa Lopez100% (1)
- Assessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuDocument80 pagesAssessment of Respiratory System: Submitted by Pankaj Singh Rana Nurse Practitioner in Critical Care, SrhuMary Christine Estrada CabactulanNo ratings yet
- Clinical SkilllllllllllllllDocument12 pagesClinical SkilllllllllllllllAlmira Putri100% (1)
- Assessment of The Lungs and ThoraxDocument21 pagesAssessment of The Lungs and ThoraxNur Rofikoh Bil Karomah100% (2)
- Respiratory Examination OSCE GuideDocument14 pagesRespiratory Examination OSCE GuideSam James100% (1)
- A Case Study On Bronchial Asthma in Acute ExacerbationDocument71 pagesA Case Study On Bronchial Asthma in Acute ExacerbationATEHAN BORDSNo ratings yet
- EmphysemaDocument29 pagesEmphysemajericx2605No ratings yet
- CPAC-SON-HA-7-Thorax-1Document59 pagesCPAC-SON-HA-7-Thorax-1misshalieediiNo ratings yet
- Jarvis Chapter 18 Study GuideDocument5 pagesJarvis Chapter 18 Study GuideEmily Cheng100% (2)
- How to use an incentive spirometer for COPDDocument19 pagesHow to use an incentive spirometer for COPDKoleen KirstenNo ratings yet
- Nursing Management of Respiratory DisordersDocument151 pagesNursing Management of Respiratory DisordersAbirajan100% (2)
- MEDICAL SURGICAL (MS) RLE PULMONARY ASSESSMENTDocument8 pagesMEDICAL SURGICAL (MS) RLE PULMONARY ASSESSMENTYman Gio BumanglagNo ratings yet
- Bates Outline of Chapter 8Document15 pagesBates Outline of Chapter 8KatherynSotoNo ratings yet
- Pulmonary Tuberculosis With Severe MalnutritionDocument49 pagesPulmonary Tuberculosis With Severe MalnutritionYifei Ping LeongshiNo ratings yet
- Thoracic & Lung Assessment GuideDocument66 pagesThoracic & Lung Assessment GuideJoyce Jacobe0% (1)
- Lungs and ThoraxDocument9 pagesLungs and ThoraxMaria Mika Ella RetizaNo ratings yet
- Age Rate (In Breaths Per Minute)Document13 pagesAge Rate (In Breaths Per Minute)Itadori YujiNo ratings yet
- Respiratory exam guideDocument3 pagesRespiratory exam guideAndreea Q. PopaNo ratings yet
- Case Study On AsthmaDocument8 pagesCase Study On AsthmaDoff Cruz100% (1)
- Chest and Lung Development and PhysiologyDocument9 pagesChest and Lung Development and PhysiologyironNo ratings yet
- Cough AsthamDocument15 pagesCough AsthamOM BAWNENo ratings yet
- Respiratory System Chapter SummaryDocument19 pagesRespiratory System Chapter SummaryAmit Kiran RathNo ratings yet
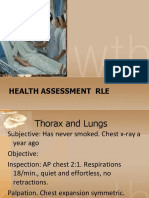
- Thorax and LungsDocument11 pagesThorax and LungsJoel SantosNo ratings yet
- Respiratory AssessmentDocument43 pagesRespiratory AssessmentLui Andrei AnilaNo ratings yet
- Respiratory ExaminarionDocument40 pagesRespiratory ExaminarionAbdelrahman AldemerdashNo ratings yet
- COPD - Case PresentationDocument68 pagesCOPD - Case PresentationJaslir MendozaNo ratings yet
- Block B Overview of Respiratory Exam PresentationDocument5 pagesBlock B Overview of Respiratory Exam PresentationKim Adarem Joy ManimtimNo ratings yet
- ملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةDocument59 pagesملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةabdullah almatary100% (1)
- Respiratory Syatem: January 2009Document19 pagesRespiratory Syatem: January 2009aarti devNo ratings yet
- ASSESSING THORAX and LUNGSDocument25 pagesASSESSING THORAX and LUNGSPrincess AñabezaNo ratings yet
- Respiratory Exam (RCT)Document8 pagesRespiratory Exam (RCT)kenners100% (31)
- 8 Lung Auscultation Points and SoundsDocument11 pages8 Lung Auscultation Points and SoundsCHARIEMAE CA�AZARES100% (1)
- SodaPDF Merged Merging ResultDocument648 pagesSodaPDF Merged Merging ResultFaith madayagNo ratings yet
- 2020thoraxlungs Neckheart VesselsDocument171 pages2020thoraxlungs Neckheart VesselsFaith madayagNo ratings yet
- Chapter 27Document6 pagesChapter 27monster40lbsNo ratings yet
- Bronchial Asthma CaseDocument11 pagesBronchial Asthma CaseAngelaTrinidadNo ratings yet
- The Process of OxygenationDocument7 pagesThe Process of OxygenationMich CercadoNo ratings yet
- The Process of OxygenationDocument5 pagesThe Process of Oxygenationapi-3744683100% (3)
- Review NotesDocument9 pagesReview NotesKhaskie Geneva DumaguinNo ratings yet
- Pulmonary Ventilation and OxygenationDocument87 pagesPulmonary Ventilation and Oxygenationபிரேம் குமார் ராஜாமணிNo ratings yet
- Blueprint For Final Exam - Doc Health AssessmentDocument13 pagesBlueprint For Final Exam - Doc Health AssessmentKim DepapeNo ratings yet
- Assessment of the Respiratory SystemDocument20 pagesAssessment of the Respiratory SystemnadyaNo ratings yet
- Physical ExaminationDocument55 pagesPhysical Examinationdakshpanchal26369No ratings yet
- Pulse OximetryDocument7 pagesPulse OximetryEmerson De SilvaNo ratings yet
- ABCDE ApproachDocument19 pagesABCDE ApproachmariamNo ratings yet
- Chest Wall Expands Increase NegativeDocument2 pagesChest Wall Expands Increase NegativeRemelou Garchitorena AlfelorNo ratings yet
- Nursing Respiratory SystemDocument254 pagesNursing Respiratory SystemWendy EvansNo ratings yet
- Essential Parameters of Airway Evaluation Lecture 6Document27 pagesEssential Parameters of Airway Evaluation Lecture 69yqgmkvyzdNo ratings yet
- Chest Examination: Syeda Afsheen Daud Lecturer IPMR KMUDocument59 pagesChest Examination: Syeda Afsheen Daud Lecturer IPMR KMUCHANGEZ KHAN SARDARNo ratings yet
- ABCDE ApproachDocument7 pagesABCDE ApproachmariamNo ratings yet
- RespiratoryDocument29 pagesRespiratoryKristine Joy Librando EscalanteNo ratings yet
- Respiratory gymnastics (Translated): Purification - Health - Strength - EnergyFrom EverandRespiratory gymnastics (Translated): Purification - Health - Strength - EnergyNo ratings yet
- A Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to the Nose and Its Disorders, Diagnosis, Treatment and Related ConditionsNo ratings yet
- FNCP CHN Health ThreatDocument5 pagesFNCP CHN Health ThreatYoongiNo ratings yet
- NCP FinalDocument5 pagesNCP FinalYoongiNo ratings yet
- NCP FinalDocument5 pagesNCP FinalYoongiNo ratings yet
- Family nursing problems for hyperthermia and arthritisDocument5 pagesFamily nursing problems for hyperthermia and arthritisYoongiNo ratings yet
- Cues/Data Family Nursing ProblemDocument1 pageCues/Data Family Nursing ProblemYoongiNo ratings yet
- Family nursing problems for hyperthermia and arthritisDocument5 pagesFamily nursing problems for hyperthermia and arthritisYoongiNo ratings yet
- NCM 214 Aquino - Case StudyDocument3 pagesNCM 214 Aquino - Case StudyYoongiNo ratings yet
- Article Critique 2019Document3 pagesArticle Critique 2019YoongiNo ratings yet
- Application LetterDocument1 pageApplication LetterYoongiNo ratings yet
- Pe March 2020Document6 pagesPe March 2020YoongiNo ratings yet
- Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesAssessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationAlyssa Moutrie Dulay Arabe100% (1)
- Acetone chemical treatment guideDocument90 pagesAcetone chemical treatment guidewilson chinyamurindiNo ratings yet
- Inspiration - 7i - Ventilator EventDocument6 pagesInspiration - 7i - Ventilator EventLicitaciones InbiosNo ratings yet
- 2015 Chest - Blue & Falls ProtocolsDocument12 pages2015 Chest - Blue & Falls ProtocolsWilmer Yanquen VillarrealNo ratings yet
- DGMS Form J To UDocument14 pagesDGMS Form J To UShiv KumarNo ratings yet
- Scorebuilders Cardiac ReviewDocument16 pagesScorebuilders Cardiac Reviewboogie33100% (1)
- CoVent-19 Challenge AbstractDocument2 pagesCoVent-19 Challenge AbstractJuan José GuerreroNo ratings yet
- SATBHSS Presentation Template DR Moyo 19Document109 pagesSATBHSS Presentation Template DR Moyo 19Victor Kbx Kachepa JnrNo ratings yet
- Hemodynamic Monitoring ExplainedDocument19 pagesHemodynamic Monitoring ExplainedAlma SusanNo ratings yet
- Digestion Regents QuestionsDocument3 pagesDigestion Regents Questionsabisantiago613175% (4)
- Respiration in Organisms - Others - CBSE7B - Respiration in Organisms - Test - 01Document2 pagesRespiration in Organisms - Others - CBSE7B - Respiration in Organisms - Test - 01Vansh BhallaNo ratings yet
- Pulmonary ConditionsDocument42 pagesPulmonary ConditionsMinetteNo ratings yet
- Primary ComplexDocument12 pagesPrimary ComplexLevi PosadasNo ratings yet
- BLS TRAINING MANUAL Second Edition PDF 2023-1 - 240226 - 093323Document93 pagesBLS TRAINING MANUAL Second Edition PDF 2023-1 - 240226 - 093323mohdnor29No ratings yet
- Pulmonary Function Testing: David A. Kaminsky Charles G. Irvin EditorsDocument322 pagesPulmonary Function Testing: David A. Kaminsky Charles G. Irvin EditorsMihai-Marian Rusei100% (1)
- Diaphragmatic breathing: A concise guide to this important breathing techniqueDocument23 pagesDiaphragmatic breathing: A concise guide to this important breathing techniqueSonia guptaNo ratings yet
- Donning and Doffing PPE for COVID CareDocument10 pagesDonning and Doffing PPE for COVID CareAla'a Emerald AguamNo ratings yet
- Chapter 1 The Human OrganismDocument12 pagesChapter 1 The Human OrganismJenny AnneNo ratings yet
- ASL Project by Ansh Semwal XII - S2Document25 pagesASL Project by Ansh Semwal XII - S2KESHAV VARSHNEYNo ratings yet
- FU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Document6 pagesFU-M2-CU6 LEC Planning Phase-Towards Goals and Outcomes.Shiro KagomeNo ratings yet
- SDS - Diversey Emerel Multi-Surface Creme Cleanser PDFDocument5 pagesSDS - Diversey Emerel Multi-Surface Creme Cleanser PDFNdega Ya ChumaNo ratings yet
- C-Mac Stylet For Et Tube PlacementDocument2 pagesC-Mac Stylet For Et Tube Placementamor kermayaNo ratings yet
- LA County Treatment Protocols 2018-12-01Document371 pagesLA County Treatment Protocols 2018-12-01Anonymous gTXqJVAmNo ratings yet
- Operator Manual SV800Document282 pagesOperator Manual SV800Nandhini SivakumarNo ratings yet
- NPMCN DissertationDocument4 pagesNPMCN DissertationHelpWritingMyPaperCanada100% (1)
- Disassembly/Assembly: Primus® Family Breathing SystemDocument2 pagesDisassembly/Assembly: Primus® Family Breathing Systemheru pratiknoNo ratings yet
- Therapy: Dr. Ravinder Narwal MPT Cardiopulmonary MPT-OrthoDocument27 pagesTherapy: Dr. Ravinder Narwal MPT Cardiopulmonary MPT-OrthoRavin NarwalNo ratings yet
- Geographic Identifiers CHNNDocument3 pagesGeographic Identifiers CHNNjaira magbanuaNo ratings yet
- SDSDetail PageDocument7 pagesSDSDetail PageHewa PCNo ratings yet
- Pulmonary Function TestingDocument10 pagesPulmonary Function TestingSamman AftabNo ratings yet