You might also like
- Post Exposure ProphylaxisDocument23 pagesPost Exposure ProphylaxisDAPCU TiruvallurNo ratings yet
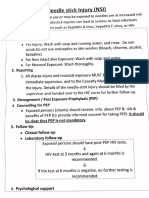
- Needlestick Injury ProtocolDocument5 pagesNeedlestick Injury Protocoldr rajoreNo ratings yet
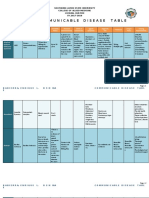
- Communicable Disease TableDocument12 pagesCommunicable Disease TableEnrique Lowe BabierraNo ratings yet
- Nursing Care Plan LeukemiaDocument2 pagesNursing Care Plan Leukemiaderic87% (30)
- Nursing Care Plan Neonatal SepsisDocument2 pagesNursing Care Plan Neonatal Sepsisderic100% (20)
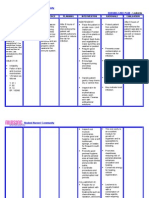
- S.N O Nursing Assessmen T Nursing Diagnosis Goal Nursing Intervention Nursing Implementati ON Rationale Evaluati ONDocument7 pagesS.N O Nursing Assessmen T Nursing Diagnosis Goal Nursing Intervention Nursing Implementati ON Rationale Evaluati ONSimran JosanNo ratings yet
- Nursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Document3 pagesNursing Care Plan For Diabetes Mellitus Type 2 (Kenneth Regida)Kenneth Anthony Tiu Regida100% (8)
- Fever Diff v38 Web PDFDocument1 pageFever Diff v38 Web PDFSharma JiNo ratings yet
- HIV/AIDS Concept MapDocument1 pageHIV/AIDS Concept MapAira AgolongNo ratings yet
- CareplanDocument2 pagesCareplanapi-381090302No ratings yet
- Nursing Care Plan - SepsisDocument2 pagesNursing Care Plan - SepsisJoe Mark Salamero86% (21)
- Nursing Care Plan Diabetes Mellitus Type 2Document2 pagesNursing Care Plan Diabetes Mellitus Type 2deric89% (75)
- Communicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Document11 pagesCommunicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Casilda FranciscoNo ratings yet
- What Is HIV?Document10 pagesWhat Is HIV?MarryRose Dela Torre FerrancoNo ratings yet
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisChristian Remetio100% (1)
- Student Nurses' Community: NURSING CARE PLAN Neonatal SepsisDocument2 pagesStudent Nurses' Community: NURSING CARE PLAN Neonatal SepsisPanJan BalNo ratings yet
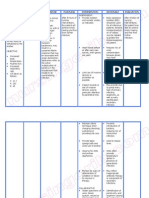
- Assessme NT Diagnos Is Analys Is Planni NG Intervention Rationale Evaluati OnDocument4 pagesAssessme NT Diagnos Is Analys Is Planni NG Intervention Rationale Evaluati OnJasmine BesaNo ratings yet
- Nursing Care Plan - RabiesDocument2 pagesNursing Care Plan - Rabiesderic89% (9)
- Risk factors, signs, symptoms and nursing care for herpes genitalisDocument1 pageRisk factors, signs, symptoms and nursing care for herpes genitalisDanii LuvNo ratings yet
- Assessment Diagnosis Inference Planning Interventions Evaluation SubjectiveDocument2 pagesAssessment Diagnosis Inference Planning Interventions Evaluation SubjectiveMikaela Carisse F. BalbonNo ratings yet
- System Disorder: Herpes SimplexDocument1 pageSystem Disorder: Herpes SimplexEli ReyesNo ratings yet
- Knowledge of Hiv, Aids, and Antiretroviral Therapy (Art)Document5 pagesKnowledge of Hiv, Aids, and Antiretroviral Therapy (Art)Tee flowNo ratings yet
- NCP - Yeast InfectionDocument2 pagesNCP - Yeast InfectionChelzie Laserna100% (2)
- En - Acc Exposure Blood Body Fluids - PosterDocument1 pageEn - Acc Exposure Blood Body Fluids - Posterdhira aninditaNo ratings yet
- Sbar 6Document3 pagesSbar 6marwajr2509No ratings yet
- Handwashing InkyDocument21 pagesHandwashing InkymarilexdomagsangNo ratings yet
- Post Exposure Prophylaxis Imep TotDocument47 pagesPost Exposure Prophylaxis Imep TotHarshaWakodkarNo ratings yet
- Occupational Health Risks For Healthcare WorkersDocument32 pagesOccupational Health Risks For Healthcare WorkersSyi VeenaNo ratings yet
- UNIT 1 LAB Diagnosing and Treating A Jellyfish Sting Mariam SalhienDocument7 pagesUNIT 1 LAB Diagnosing and Treating A Jellyfish Sting Mariam SalhienMariam SalhienNo ratings yet
- Understanding HIV/AIDSDocument2 pagesUnderstanding HIV/AIDSMbiatat BrandonNo ratings yet
- Pre-Op (March 7,2019) Component Result Normal Range Interpretation Implication Nursing Responsibiliti Es 11.76 X 10 9/L 4,000-10,000Document10 pagesPre-Op (March 7,2019) Component Result Normal Range Interpretation Implication Nursing Responsibiliti Es 11.76 X 10 9/L 4,000-10,000Lemuel GuevarraNo ratings yet
- Nursing Care PlanDocument1 pageNursing Care PlanBtob meloNo ratings yet
- Nursing Care Plan (NCP) For A Patient With Acute Renal FailureDocument3 pagesNursing Care Plan (NCP) For A Patient With Acute Renal FailureKian HerreraNo ratings yet
- Nursing Care Plan 2Document2 pagesNursing Care Plan 2marichelle plazaNo ratings yet
- Nursing Care Plan Nursing Diagnosis Anxiety (Mild)Document4 pagesNursing Care Plan Nursing Diagnosis Anxiety (Mild)yvenette_kris871881% (27)
- Needle Stick Injury Prevention and Management: Nirupama Sahoo ICNDocument18 pagesNeedle Stick Injury Prevention and Management: Nirupama Sahoo ICNSantoshMohapatraNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationDocument2 pagesNursing Care Plan: Assessment Diagnosis Inference Planning Intervention Rationale EvaluationJamie Haravata0% (1)
- This Study Resource Was Shared Via: Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDocument3 pagesThis Study Resource Was Shared Via: Cues Nursing Diagnosis Objectives Interventions Rationale EvaluationDanica Fave AndiamNo ratings yet
- The Complete Guide To HIV / AIDs: Symptoms, Diagnosis, Risks, Treatments & SupportFrom EverandThe Complete Guide To HIV / AIDs: Symptoms, Diagnosis, Risks, Treatments & SupportNo ratings yet
- 6 Steps of Hand HygieneDocument1 page6 Steps of Hand HygieneGenevieve Caecilia Linda KartonoNo ratings yet
- Sharps Infographic Web Sm3Document1 pageSharps Infographic Web Sm3Genevieve Caecilia Linda KartonoNo ratings yet
- Sharps Infographic Web Sm3Document1 pageSharps Infographic Web Sm3Genevieve Caecilia Linda KartonoNo ratings yet
- DX DiagDocument27 pagesDX DiagGenevieve Caecilia Linda KartonoNo ratings yet
- 01 Cir 52 6 1023Document7 pages01 Cir 52 6 1023Genevieve Caecilia Linda KartonoNo ratings yet
- MTP For ASA Transfusion Committee FinalDocument11 pagesMTP For ASA Transfusion Committee FinalImmanuel HabeahanNo ratings yet
- S.T.A.R.T: Simple Triage and Rapid TreatmentDocument14 pagesS.T.A.R.T: Simple Triage and Rapid TreatmentGenevieve Caecilia Linda KartonoNo ratings yet
- Growth ChartDocument4 pagesGrowth ChartGenevieve Caecilia Linda KartonoNo ratings yet
- Research in Social and Administrative PharmacyDocument4 pagesResearch in Social and Administrative PharmacyAndrea MendozaNo ratings yet
- Manufacturing of Viral Vectors Part II Downstream Processing and Safety Aspects PDFDocument16 pagesManufacturing of Viral Vectors Part II Downstream Processing and Safety Aspects PDFSana AfzalNo ratings yet
- Pathology Important Solved BCQs 5th Semester MBBS + 3rd Semester BDS LUMHSDocument57 pagesPathology Important Solved BCQs 5th Semester MBBS + 3rd Semester BDS LUMHSNaheed Jatoi100% (1)
- Microbial Diseases (Skin Eyes)Document23 pagesMicrobial Diseases (Skin Eyes)Hazel Mae FestinNo ratings yet
- Fvets 09 1080397Document11 pagesFvets 09 1080397botond77No ratings yet
- Progress Exam - MicrobiologyDocument75 pagesProgress Exam - MicrobiologyAngelicaNo ratings yet
- ABH NanoMack Details R CDocument6 pagesABH NanoMack Details R CrajasajjadNo ratings yet
- NCLEX Notes for Airborne, Contact, and Droplet PrecautionsDocument3 pagesNCLEX Notes for Airborne, Contact, and Droplet PrecautionsTasha100% (20)
- Differentiate Between Theoretical and Empirical Literature ReviewDocument8 pagesDifferentiate Between Theoretical and Empirical Literature ReviewafmzwasolldhwbNo ratings yet
- Lawatan Makmal Virtual Bioteknologi (A182950)Document2 pagesLawatan Makmal Virtual Bioteknologi (A182950)AINA AZRA BINTI NASHARUDDINNo ratings yet
- What Is COVID-19 and How Can I Protect Myself?: Answer From Pritish K. Tosh, M.DDocument2 pagesWhat Is COVID-19 and How Can I Protect Myself?: Answer From Pritish K. Tosh, M.DDonNo ratings yet
- Acute Bronchitis PDFDocument2 pagesAcute Bronchitis PDFGenoMacaraanNo ratings yet
- De Thi Chon DT Nam 2002 Mon Tieng AnhDocument4 pagesDe Thi Chon DT Nam 2002 Mon Tieng AnhTrần HuyềnNo ratings yet
- Gdocs Trans TemplateDocument3 pagesGdocs Trans TemplateshichiNo ratings yet
- Day Two. Disease ResourceDocument8 pagesDay Two. Disease ResourcealicekadzokatanaNo ratings yet
- Daftar Pustaka KtiDocument6 pagesDaftar Pustaka KtiayuNo ratings yet
- Dissertation Martin SchraubDocument5 pagesDissertation Martin SchraubHelpWithFilingDivorcePapersSalem100% (1)
- Hans India Hyderabad - 25-04-20 PDFDocument10 pagesHans India Hyderabad - 25-04-20 PDFShubham NathNo ratings yet
- Communicable DiseasesDocument20 pagesCommunicable DiseasesCai SolanoNo ratings yet
- Wendy Silvers Master Series Interview - Dr. Judy MikovitsDocument92 pagesWendy Silvers Master Series Interview - Dr. Judy MikovitsDaniela30No ratings yet
- Are Viruses Living or Non-LivingDocument2 pagesAre Viruses Living or Non-LivingKyrie OcampoNo ratings yet
- MICR 2101 Review QuestionsDocument2 pagesMICR 2101 Review QuestionsIsabella CarewNo ratings yet
- NFL Memo On COVID-19 Protocol UpdatesDocument5 pagesNFL Memo On COVID-19 Protocol UpdatesHouston ChronicleNo ratings yet
- 1.1 Background of The Study: Bamboo (Bambusa Vulgaris) As Larvicidal Against Mosquito (Aedes Aegypti) LarvaeDocument19 pages1.1 Background of The Study: Bamboo (Bambusa Vulgaris) As Larvicidal Against Mosquito (Aedes Aegypti) LarvaeLightning ArhatNo ratings yet
- Hepatitis BDocument3 pagesHepatitis Bkrishna chandrakani100% (1)
- ESKAPE Pathogen & AntibiogramDocument33 pagesESKAPE Pathogen & Antibiogramvijayasree bavireddyNo ratings yet
- Infectious Diseases Oral RevalidaDocument22 pagesInfectious Diseases Oral RevalidaShella Mae UsquisaNo ratings yet
- MLS 422 Diagnostic MicrobiologyDocument50 pagesMLS 422 Diagnostic MicrobiologyMayowa OgunmolaNo ratings yet
- BAM Chapter 23 - Methods For Cosmetics - FDADocument11 pagesBAM Chapter 23 - Methods For Cosmetics - FDARhenso Victor Albites CondoriNo ratings yet
- Immunity WorksheetDocument4 pagesImmunity WorksheetShahd MohamedNo ratings yet