You might also like
- The Ideal Candida Diet Cookbook; The Superb Diet Guide To Alleviate Candida Symptoms And Restore Gut Health With Nutritious RecipesFrom EverandThe Ideal Candida Diet Cookbook; The Superb Diet Guide To Alleviate Candida Symptoms And Restore Gut Health With Nutritious RecipesNo ratings yet
- ClindamycinDocument2 pagesClindamycinCrissah LacernaNo ratings yet
- Herpes Simplex Varicella and Zoster: Clinical Manifestations and TreatmentFrom EverandHerpes Simplex Varicella and Zoster: Clinical Manifestations and TreatmentRating: 5 out of 5 stars5/5 (19)
- NCP & Drug Study (Karisha Guevarra)Document17 pagesNCP & Drug Study (Karisha Guevarra)Karisha GuevarraNo ratings yet
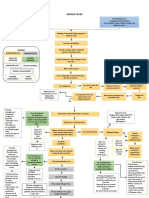
- Concept Map Dengue FeverDocument2 pagesConcept Map Dengue FeverChelsyann FerolinoNo ratings yet
- ICC AUDIT TOOL AND TRIAGE ALGORHYTHM DGMC - WPS PDF Convert PDFDocument40 pagesICC AUDIT TOOL AND TRIAGE ALGORHYTHM DGMC - WPS PDF Convert PDFWendy Dela PenaNo ratings yet
- Villamaria - Drug StudyDocument11 pagesVillamaria - Drug StudyHey LeunNo ratings yet
- Drugstudy 20Document9 pagesDrugstudy 20MahledJoy EnriquezNo ratings yet
- Monkeypox, Diagnosis and TreatmentDocument55 pagesMonkeypox, Diagnosis and TreatmentsamiNo ratings yet
- Risk For Infection - NCPDocument3 pagesRisk For Infection - NCPHamil BanagNo ratings yet
- Two Emergent Diseases-Communicable DiseasesDocument1 pageTwo Emergent Diseases-Communicable DiseasesmariaalmiramsaritaNo ratings yet
- DG2 KetorolacDocument1 pageDG2 KetorolacEkusu Yu ShunNo ratings yet
- Drug Study RyDocument30 pagesDrug Study RyRyrey Abraham PacamanaNo ratings yet
- Finals 3Document5 pagesFinals 3Fau Fau DheoboNo ratings yet
- MaravirocDocument1 pageMaravirocRhezaNo ratings yet
- Drug StudyDocument4 pagesDrug StudyRochelle TenederoNo ratings yet
- Viral Disease Handout 2007Document10 pagesViral Disease Handout 2007anon-19857No ratings yet
- Drug Name Dosage, Route, and Frequency Drug Action Indications Contraindicati ONS Adverse Effect Nursing Responsibilities Brand Name: AviraxDocument2 pagesDrug Name Dosage, Route, and Frequency Drug Action Indications Contraindicati ONS Adverse Effect Nursing Responsibilities Brand Name: AviraxAdhaNo ratings yet
- Electric Shock/Lightning Injury: Key QuestionsDocument2 pagesElectric Shock/Lightning Injury: Key QuestionsarniwiantiNo ratings yet
- Thrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (SeizuresDocument1 pageThrombolic, Thrombocytopenic Purpurvhemoclytic Uremic Syndrome (Seizuresgeorgeloto12No ratings yet
- Poster CovidDocument1 pagePoster CovidNikesh MNo ratings yet
- 10 ImmuneSystemMedicationsDocument7 pages10 ImmuneSystemMedicationsAlano S. LimgasNo ratings yet
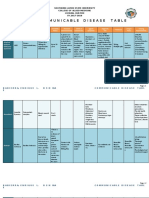
- CO Mmunicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Document12 pagesCO Mmunicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Enrique Lowe BabierraNo ratings yet
- Ceftriaxone SodiumDocument2 pagesCeftriaxone SodiumSTORAGE FILENo ratings yet
- Case ScenarioDocument10 pagesCase ScenarioFrincislyn CatabayNo ratings yet
- HSB Pneumonia Antibiotic AlgorithmDocument4 pagesHSB Pneumonia Antibiotic AlgorithmDr.Senthil KumarNo ratings yet
- Junio Covid-19 - Sanford GuideDocument8 pagesJunio Covid-19 - Sanford GuideEfraín Castilla MinayaNo ratings yet
- Drug TabulationDocument6 pagesDrug TabulationKANT JAMES D. MAHANNo ratings yet
- Rifaximin Drug StudyDocument4 pagesRifaximin Drug StudySTORAGE FILENo ratings yet
- NCP - Yeast InfectionDocument2 pagesNCP - Yeast InfectionChelzie Laserna100% (2)
- Cefuroxime (Drug Study)Document2 pagesCefuroxime (Drug Study)Rosebel LaguraNo ratings yet
- Smallpox Diagnostic Algorithm Poster 2 PagesDocument2 pagesSmallpox Diagnostic Algorithm Poster 2 PagesAnudeep DeekondaNo ratings yet
- Concept Mapping For COVID-19: BioethicsDocument5 pagesConcept Mapping For COVID-19: BioethicsHelen Fairodz AmoraNo ratings yet
- Covid-19, Sars Cov-2Document8 pagesCovid-19, Sars Cov-2siti lailatul mahmudahNo ratings yet
- Drug StudyyyyDocument3 pagesDrug StudyyyyNathalie kate petallarNo ratings yet
- National Kidney and Transplant Institute: East Avenue, Quezon CityDocument1 pageNational Kidney and Transplant Institute: East Avenue, Quezon CityLizette Oribe ReyNo ratings yet
- INFLUENZADocument4 pagesINFLUENZAJeanne CastroNo ratings yet
- Diarrhea PEDSDocument10 pagesDiarrhea PEDSOasis LimitedNo ratings yet
- Drug-Study PalivizumabDocument2 pagesDrug-Study PalivizumabIrize DenagaNo ratings yet
- Bibliography: Life Span - Philadelphia, PA 19103: F.A. Davis CompanyDocument5 pagesBibliography: Life Span - Philadelphia, PA 19103: F.A. Davis CompanyCarlos LleverNo ratings yet
- Concept Map RSVDocument1 pageConcept Map RSVNoemi GabayNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease: PediatricsDocument8 pagesRheumatic Fever and Rheumatic Heart Disease: PediatricsRea Dominique CabanillaNo ratings yet
- Ceftriaxone and CiprofloxacinDocument4 pagesCeftriaxone and CiprofloxacinRae DaWn VaLesNo ratings yet
- Drug StudyDocument2 pagesDrug StudyRoland YusteNo ratings yet
- Ear Problems: Key QuestionsDocument2 pagesEar Problems: Key QuestionsarniwiantiNo ratings yet
- Case Study BurnDocument3 pagesCase Study BurnInday BebeNo ratings yet
- Com +Nursing+Care+Plan+Chicken+PoxDocument2 pagesCom +Nursing+Care+Plan+Chicken+PoxDahl Obañana Erojo100% (1)
- Nursingcrib Com NURSING CARE PLAN Chicken Pox PDFDocument2 pagesNursingcrib Com NURSING CARE PLAN Chicken Pox PDFAkeroNo ratings yet
- Drug StudyDocument16 pagesDrug StudyAlessandra Franchesca CortezNo ratings yet
- NURSING CARE PLAN Chicken PoxDocument2 pagesNURSING CARE PLAN Chicken Poxderic87% (62)
- Demam Berdarah Dengue Pada AnakDocument70 pagesDemam Berdarah Dengue Pada AnakHarton MuhammadNo ratings yet
- Communicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Document11 pagesCommunicable Disease Table: Southern Luzon State University College of Allied Medicine Lucban, Quezon SY.2017-2018Casilda FranciscoNo ratings yet
- Drug Classification Indication of Use Mechanism of Action Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesDrug Classification Indication of Use Mechanism of Action Contraindication Side Effects Nursing ResponsibilitiesChlodette Eizl M. LaurenteNo ratings yet
- PEDIA - Drug Study & NCPDocument24 pagesPEDIA - Drug Study & NCPCzarina Mae Lomboy100% (1)
- Drug StudyDocument24 pagesDrug StudySittie Nashieva A. UsmanNo ratings yet
- Nursing Care Plan: WWW - Unp.edu - PHDocument4 pagesNursing Care Plan: WWW - Unp.edu - PHKrizha Angela Nicolas0% (1)
- DRUG STUDY (Ceftriaxone)Document2 pagesDRUG STUDY (Ceftriaxone)Avianna CalliopeNo ratings yet
- Drug Study QIDocument8 pagesDrug Study QImaeDonitaNo ratings yet
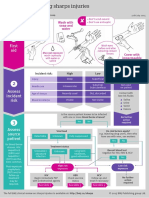
- Sharps Infographic Web Sm3Document1 pageSharps Infographic Web Sm3Genevieve Caecilia Linda KartonoNo ratings yet
- The EMERGENCY SEVERITY INDEXDocument4 pagesThe EMERGENCY SEVERITY INDEXWindyNo ratings yet
- Is - Iso-2631-2-2003Document14 pagesIs - Iso-2631-2-2003picottNo ratings yet
- Culata 3406E C15Document19 pagesCulata 3406E C15carlos moralesNo ratings yet
- (Pro-Forma) : WHEREAS, The RE Developer Is Authorized To Proceed To The Development Stage of Its RenewableDocument13 pages(Pro-Forma) : WHEREAS, The RE Developer Is Authorized To Proceed To The Development Stage of Its RenewableJoy AlamedaNo ratings yet
- 2372 - The Bermuda TriangleDocument97 pages2372 - The Bermuda TriangleRomain SuchetNo ratings yet
- L3 Role of EHO and AEHO in MalaysiaDocument37 pagesL3 Role of EHO and AEHO in MalaysiaNandakumaran SelvakumaranNo ratings yet
- A Brief Biography of Hazrat Shah Chirag Sahab HyderabadDocument5 pagesA Brief Biography of Hazrat Shah Chirag Sahab HyderabadMohammed Abdul Hafeez, B.Com., Hyderabad, India100% (1)
- Ia Masonry 17Document8 pagesIa Masonry 17Alliah Jane DelfinNo ratings yet
- ABPK2203 Perception and Emotion Module PDFDocument147 pagesABPK2203 Perception and Emotion Module PDFPhoebeilsie RaimiNo ratings yet
- 1354 Nigeria Country SuDocument48 pages1354 Nigeria Country Sudharmendra_kanthariaNo ratings yet
- More Serious Health ProblemsDocument3 pagesMore Serious Health ProblemsYassin KhanNo ratings yet
- AnnunakiDocument39 pagesAnnunakiCristian Stoica100% (10)
- Surface Active Agents - Detergents - Determination of Cationic-Active Matter ContentDocument14 pagesSurface Active Agents - Detergents - Determination of Cationic-Active Matter ContenttuanphamNo ratings yet
- Digit Private Car PolicyDocument15 pagesDigit Private Car PolicyLegal NoticeNo ratings yet
- Hannah SchizopreniaDocument5 pagesHannah SchizopreniaEliezah RodriguezNo ratings yet
- Latvian VocabularyDocument6 pagesLatvian Vocabularyparajms8778No ratings yet
- "View" "Slide Show.": Resources Chapter MenuDocument89 pages"View" "Slide Show.": Resources Chapter Menuelty TanNo ratings yet
- Additional Songs (Chords)Document8 pagesAdditional Songs (Chords)Ralph VelosoNo ratings yet
- Generator Merk MarelliDocument118 pagesGenerator Merk MarelliGurun Reinanto100% (2)
- Rabbit DiseasesDocument3 pagesRabbit DiseasescioceagabrielNo ratings yet
- Mock ExamDocument7 pagesMock ExamJoannaNo ratings yet
- The Hunter's Gonna Lay Low (Unknown) (Z-Library)Document55 pagesThe Hunter's Gonna Lay Low (Unknown) (Z-Library)mddgrcvNo ratings yet
- HI98308 ManualDocument2 pagesHI98308 ManualFùq Tất ỨqNo ratings yet
- Typical NotesDocument13 pagesTypical NotesDevang TripathiNo ratings yet
- AXi Series ManualDocument35 pagesAXi Series ManualRuben NinaNo ratings yet
- Thermo-Mechanical and Morphological Characterization of Needle Punched Non-Woven Banana Fiber Reinforced Polymer CompositesDocument13 pagesThermo-Mechanical and Morphological Characterization of Needle Punched Non-Woven Banana Fiber Reinforced Polymer CompositesRajeshwaranNo ratings yet
- 03 Welding Control Procedure - Asf QC WCP 001Document7 pages03 Welding Control Procedure - Asf QC WCP 001el_sharkawy2011100% (1)
- Gulf of Mannar Guide PDFDocument78 pagesGulf of Mannar Guide PDFDrVarghese Plavila JohnNo ratings yet
- MSDS Temprid SC365,4 - EngDocument10 pagesMSDS Temprid SC365,4 - EngArman AsnanNo ratings yet
- Chernobyl Poses More Risk Than Fukushima': Comisión Gestora de Las Pruebas de Acceso A La UniversidadDocument4 pagesChernobyl Poses More Risk Than Fukushima': Comisión Gestora de Las Pruebas de Acceso A La UniversidadUlyas HnyhNo ratings yet
- Body and Trim (Exterior)Document17 pagesBody and Trim (Exterior)Woong-Sub Lee0% (1)