100% found this document useful (2 votes)
2K views1 pageFlexible Work Arrangement Agreement
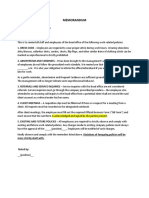
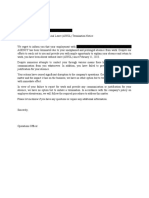
This document outlines a flexible work arrangement agreement between an employee and their employer. It includes the employee's name, address, contact information, position, proposed work schedule including days/week, hours/day and rest periods. The dates of effectivity and expiration of the agreement are also provided. The employee certifies the arrangement was reached after consultation and agrees to it voluntarily considering ongoing losses from COVID-19. The employer's representative and employee sign to finalize the agreement.
Uploaded by
LeulaDianneCantosCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
100% found this document useful (2 votes)
2K views1 pageFlexible Work Arrangement Agreement
This document outlines a flexible work arrangement agreement between an employee and their employer. It includes the employee's name, address, contact information, position, proposed work schedule including days/week, hours/day and rest periods. The dates of effectivity and expiration of the agreement are also provided. The employee certifies the arrangement was reached after consultation and agrees to it voluntarily considering ongoing losses from COVID-19. The employer's representative and employee sign to finalize the agreement.
Uploaded by
LeulaDianneCantosCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd