You might also like
- Pela) Orai/: Rawat) Ag Hatna B.S, NdarDocument7 pagesPela) Orai/: Rawat) Ag Hatna B.S, NdarLosta NataNo ratings yet
- Checklist - Education Loan-1Document2 pagesChecklist - Education Loan-1greggtldivisionNo ratings yet
- MFC PDFDocument5 pagesMFC PDFdipmipNo ratings yet
- Co So: e D The Ho Expe N Es Incurred in CODocument2 pagesCo So: e D The Ho Expe N Es Incurred in COJason Joseph AzuraNo ratings yet
- Philhealth Pre-Auth CataractDocument6 pagesPhilhealth Pre-Auth Cataractwmarasigan2610No ratings yet
- Glucagon Stimulation Test For Adults v1 Nhs UkDocument2 pagesGlucagon Stimulation Test For Adults v1 Nhs UkNavojit ChowdhuryNo ratings yet
- Daily Shift ReportDocument18 pagesDaily Shift ReportAlaa HamoudaNo ratings yet
- SEO-Optimized Medical Certificate for SeafarerDocument3 pagesSEO-Optimized Medical Certificate for SeafarerZeno PaulNo ratings yet
- Carrying Out of Doctors Order and Fdar Documentation (Cotabato Regional and Medical Center) InstructionsDocument6 pagesCarrying Out of Doctors Order and Fdar Documentation (Cotabato Regional and Medical Center) InstructionsMarielle ChuaNo ratings yet
- Citizenship c3 c4Document5 pagesCitizenship c3 c4yinjian0001No ratings yet
- Child Care LeaveDocument4 pagesChild Care LeaveponnarrasuNo ratings yet
- Prev Med Nov 2 2021Document13 pagesPrev Med Nov 2 2021Denise CedeñoNo ratings yet
- READY FOR YOUR MEDICAL EXAMDocument2 pagesREADY FOR YOUR MEDICAL EXAMTwela GranadaNo ratings yet
- BIR - Transfer Commitment FormDocument1 pageBIR - Transfer Commitment FormNiccaNo ratings yet
- Home Health Certification and Plan of CareDocument2 pagesHome Health Certification and Plan of CarelokohugpoNo ratings yet
- ICU Nurse's Notes on Donato AntonioDocument5 pagesICU Nurse's Notes on Donato AntonioAliyah Jewel JimenezNo ratings yet
- ,TB FL: Hafit (Nofth eDocument2 pages,TB FL: Hafit (Nofth eAdil AlkhawaldiNo ratings yet
- Prelims PaperDocument10 pagesPrelims PaperDeep PanaraNo ratings yet
- Hospital Daily Monitoring - Checklist PDFDocument3 pagesHospital Daily Monitoring - Checklist PDFMarriz Bustaliño TanNo ratings yet
- COVID Instant Order-62Document3 pagesCOVID Instant Order-62SanjayKumarReddyNo ratings yet
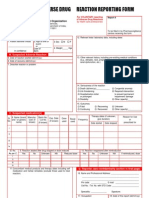
- ADR Form PDFDocument2 pagesADR Form PDFcompudoc111905No ratings yet
- 861298 نسخةDocument2 pages861298 نسخةAbdoNo ratings yet
- Pacio Vs Dohle Philman ManningDocument15 pagesPacio Vs Dohle Philman ManningAnne Ajednem100% (1)
- Circ15 2012 PDFDocument7 pagesCirc15 2012 PDFJanice Villaroya Jarales-YusonNo ratings yet
- Global Medical Center of Laguna Operational Manual Unit GuidelinesDocument4 pagesGlobal Medical Center of Laguna Operational Manual Unit GuidelinesRon OpulenciaNo ratings yet
- Boletin Del SNS 1955 OctDocument55 pagesBoletin Del SNS 1955 OctJorge Rojas FloresNo ratings yet
- Form 41Document1 pageForm 41Grace C.No ratings yet
- NUR 101 SimulationDocument8 pagesNUR 101 SimulationLora Bartlett100% (1)
- RJN Apollo Spectra Hospital-OMDocument8 pagesRJN Apollo Spectra Hospital-OMvaibhav sharmaNo ratings yet
- Referral LetterDocument2 pagesReferral LetterDevesh KhandareNo ratings yet
- SSS v. JarqueDocument9 pagesSSS v. JarqueBella SyNo ratings yet
- For Instructions, See Back of Form Form DR.1Document1 pageFor Instructions, See Back of Form Form DR.1Zach EdwardsNo ratings yet
- Catatan Perkembangan Pasien Terintegrasi (CPPT) : TGL PKL PPA Soap Nama Dan TTD PpaDocument34 pagesCatatan Perkembangan Pasien Terintegrasi (CPPT) : TGL PKL PPA Soap Nama Dan TTD PpahospitalNo ratings yet
- MotivationDocument22 pagesMotivationMOHAMMED SIDDIQNo ratings yet
- Transfusion SpecimenCollectionDocument5 pagesTransfusion SpecimenCollectionDominic EmerencianaNo ratings yet
- Peace Corps Report of Dental Examination - PC-OMS-1790 Dental 08/2009Document4 pagesPeace Corps Report of Dental Examination - PC-OMS-1790 Dental 08/2009Accessible Journal Media: Peace Corps DocumentsNo ratings yet
- Computer in Community Pharmacy 2Document16 pagesComputer in Community Pharmacy 2thakkarbineet12No ratings yet
- MTPTTP ED ProformaDocument3 pagesMTPTTP ED ProformaRajin MaahiNo ratings yet
- Opuni Sues Daily GuideDocument4 pagesOpuni Sues Daily GuideGhanaWeb EditorialNo ratings yet
- L/Epublic of Tije Tlbilippines: Tjjaguio LcitpDocument12 pagesL/Epublic of Tije Tlbilippines: Tjjaguio LcitpJP JimenezNo ratings yet
- AO 2016-0042 Annex H-6c Checklist For Review of Floor Plans - Level 3 HospitalDocument6 pagesAO 2016-0042 Annex H-6c Checklist For Review of Floor Plans - Level 3 HospitalNiel HagapeNo ratings yet
- hfw_e_435_Rt_2013 (1)Document2 pageshfw_e_435_Rt_2013 (1)Deepthi Chandra Shekar SuraNo ratings yet
- Personal Accident Claim Doctor's StatementDocument10 pagesPersonal Accident Claim Doctor's StatementIsa Rafiq Mohamed Abdul KhaderNo ratings yet
- Iso 649-1-1981Document12 pagesIso 649-1-1981Mahmoud MoussaNo ratings yet
- Bone Scan FormDocument2 pagesBone Scan FormBKNo ratings yet
- Maritime Workers Dispute Over Disability BenefitsDocument14 pagesMaritime Workers Dispute Over Disability BenefitsSabritoNo ratings yet
- R-Tinistry of Personnel, Public .Gi ",ievances Pensions Pensione, Rs WelfarejDocument2 pagesR-Tinistry of Personnel, Public .Gi ",ievances Pensions Pensione, Rs WelfarejNikhil BisuiNo ratings yet
- Interdisciplinary Plan of Care and Patient EducationDocument26 pagesInterdisciplinary Plan of Care and Patient Educationhuggr84629No ratings yet
- 'Rarus-Seugion Ttatiottatity-: HN RRDocument19 pages'Rarus-Seugion Ttatiottatity-: HN RRCATHERINE SIENNA ALTARNo ratings yet
- Kardex - Acute PancreatitisDocument5 pagesKardex - Acute PancreatitisKiara Denise TamayoNo ratings yet
- Iloilo Doctors' College Nursing Service KardexDocument4 pagesIloilo Doctors' College Nursing Service KardexKiara Denise TamayoNo ratings yet
- Physical Therapy Protocol For Knee Surgery RecoveryDocument9 pagesPhysical Therapy Protocol For Knee Surgery Recoveryحسين الخليفةNo ratings yet
- Capacity Competency 3-10-14Document3 pagesCapacity Competency 3-10-14api-256214553No ratings yet
- Stroger Hospital Intern GuideDocument43 pagesStroger Hospital Intern Guidesgod34No ratings yet
- (20-22398 17) Ex. A Credit Agreement Law DE 109Document5 pages(20-22398 17) Ex. A Credit Agreement Law DE 109larry-612445No ratings yet
- Form-1 Appl I Cat I Onfort R Ansferunderrul - 38post Almanual-I VDocument1 pageForm-1 Appl I Cat I Onfort R Ansferunderrul - 38post Almanual-I VRaj DhameliaNo ratings yet
- Hospital Negligence CaseDocument17 pagesHospital Negligence CasePrasad80% (5)
- Annex M AO 2013 0006 DO No. 185 N S 1996Document2 pagesAnnex M AO 2013 0006 DO No. 185 N S 1996Doodz ZablanNo ratings yet
- District: Mineral Foundation, KeonjharDocument5 pagesDistrict: Mineral Foundation, Keonjharf4msj2ghkpNo ratings yet
- Primary Management of PolytraumaFrom EverandPrimary Management of PolytraumaSuk-Kyung HongNo ratings yet
- Rishi Joy Therapy & Wellness Centre at MaralwadiDocument1 pageRishi Joy Therapy & Wellness Centre at MaralwadiPrathameshNo ratings yet
- Label 206035861Document1 pageLabel 206035861PrathameshNo ratings yet
- Ivpîyna K A Áatm Jel Iõivr Ivúy-SuciDocument77 pagesIvpîyna K A Áatm Jel Iõivr Ivúy-SuciPrathameshNo ratings yet
- TIP Nodal Officers - MH CircleDocument1 pageTIP Nodal Officers - MH CirclePrathameshNo ratings yet
- My Gratitude Journal: My Gratitude Journal: My Gratitude Journal: My Gratitude Journal: Date: Date: Date: DateDocument1 pageMy Gratitude Journal: My Gratitude Journal: My Gratitude Journal: My Gratitude Journal: Date: Date: Date: DatePrathameshNo ratings yet
- Morrnah N. Simeona Ho Oponopono PrayersDocument6 pagesMorrnah N. Simeona Ho Oponopono PrayersSese Seko100% (9)
- Beliefs and FeelingsDocument5 pagesBeliefs and FeelingsPrathameshNo ratings yet
- Reiki Tummo Distant Learning Student Data: (For Alumni Data and Certificate)Document2 pagesReiki Tummo Distant Learning Student Data: (For Alumni Data and Certificate)PrathameshNo ratings yet
- CreamicaDocument1 pageCreamicaPrathameshNo ratings yet
- Ho Oponopono The Easiest Way To LiveDocument8 pagesHo Oponopono The Easiest Way To LivePrathamesh100% (1)
- 10th Jan Nithyananda Third Eye ProcessDocument1 page10th Jan Nithyananda Third Eye ProcessPrathameshNo ratings yet
- In Concrete ReportDocument1 pageIn Concrete ReportSophia AmbunanNo ratings yet
- Economies of Scale CluffDocument8 pagesEconomies of Scale CluffJackson CluffNo ratings yet
- Agenda - Refractory Sector - DraftDocument2 pagesAgenda - Refractory Sector - DraftPothuraju PrudhiviNo ratings yet
- 12 Beaker Glass Pyrex 100mlDocument1 page12 Beaker Glass Pyrex 100mlzulfadli zainalNo ratings yet
- My - Statement - 01 Jul, 2023 - 09 Jul, 2023 - 8050668560Document13 pagesMy - Statement - 01 Jul, 2023 - 09 Jul, 2023 - 8050668560The HulkNo ratings yet
- Economic Resources and Basic QuestionsDocument2 pagesEconomic Resources and Basic QuestionsGine Bert Fariñas PalabricaNo ratings yet
- What Do I Owe? How Much Gas Did I Use?: Billing Period Aug 03, 2020 - Aug 27, 2020Document2 pagesWhat Do I Owe? How Much Gas Did I Use?: Billing Period Aug 03, 2020 - Aug 27, 2020Abe SimpsonNo ratings yet
- Strength Based Lean Six Sigma Book FlyerDocument2 pagesStrength Based Lean Six Sigma Book Flyerdsplus7741No ratings yet
- Hobart - HCM 300 Cutter MixerDocument26 pagesHobart - HCM 300 Cutter MixerEdgar Josue C. CosNo ratings yet
- Evoprotect 240: Technical Data SheetDocument3 pagesEvoprotect 240: Technical Data SheetJayadiNo ratings yet
- Cateora18ePPt Ch02 WH BKGRNDDocument53 pagesCateora18ePPt Ch02 WH BKGRNDbittu.abhishek99No ratings yet
- Value - At-Risk Vs Conditional Value-at-Risk in Risk Management and OptimizationDocument26 pagesValue - At-Risk Vs Conditional Value-at-Risk in Risk Management and OptimizationCyrielle DomgueNo ratings yet
- ST 200015Document12 pagesST 200015Jorge ArbelaezNo ratings yet
- SoftGel Capsule Part 2Document109 pagesSoftGel Capsule Part 2pharmashri53990% (1)
- Strictly Confidential: (For Internal and Restricted Use Only)Document27 pagesStrictly Confidential: (For Internal and Restricted Use Only)bhaiyarakeshNo ratings yet
- Basic Warp Knitting PrincipleDocument8 pagesBasic Warp Knitting PrincipleTamanna Ahmed100% (1)
- Session 2 PPT Demand-And-SupplyDocument53 pagesSession 2 PPT Demand-And-SupplyMuhammad AreebNo ratings yet
- Fully Automatic CNC Sprue Cutting Machines - 1103Document4 pagesFully Automatic CNC Sprue Cutting Machines - 1103salesNo ratings yet
- En Visual Testing ProcedureDocument7 pagesEn Visual Testing ProcedureAdham AhmedNo ratings yet
- Depreciation CVDocument71 pagesDepreciation CVRigine Pobe MorgadezNo ratings yet
- All Math Suite Bank Questions Without Answers or Explanation FromDocument1,081 pagesAll Math Suite Bank Questions Without Answers or Explanation Fromsasasa785236No ratings yet
- AE 11 Midterm Reviewer Mod 1Document3 pagesAE 11 Midterm Reviewer Mod 1Clarice NNo ratings yet
- Mercantile Law: Roll No. Total No. of Pages: 02 Total No. of Questions: 08 BBA (Sem.-5)Document2 pagesMercantile Law: Roll No. Total No. of Pages: 02 Total No. of Questions: 08 BBA (Sem.-5)Dhruv MittalNo ratings yet
- Contract Management in ProcurementDocument18 pagesContract Management in ProcurementSiampol FeepakphorNo ratings yet
- Twig Plush Pattern HackDocument15 pagesTwig Plush Pattern HackKainan FariasNo ratings yet
- Nursing Home Fatalities Update NYSDocument7 pagesNursing Home Fatalities Update NYSExsar MisaelNo ratings yet
- Simple Interest and Compound Interest Basic LevelDocument10 pagesSimple Interest and Compound Interest Basic LevelSubhash HandaNo ratings yet
- DIAPHRAGM WALL REPAIR METHOD STATEMENTDocument17 pagesDIAPHRAGM WALL REPAIR METHOD STATEMENTHemaNo ratings yet
- Identity Theft, Credit Reports, and You - Kalzumeus SoftwareDocument14 pagesIdentity Theft, Credit Reports, and You - Kalzumeus Softwarebjrfedor100% (1)
- 41 - 21-001 - AVK026 - Eng - v1-0 (1) - Check Valve Swing TypeDocument2 pages41 - 21-001 - AVK026 - Eng - v1-0 (1) - Check Valve Swing TypeBernard Bonnin CervantesNo ratings yet