You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Pregnancy TestDocument5 pagesPregnancy Testخالد محمد طه100% (1)
- Sinusitis AFP PDFDocument4 pagesSinusitis AFP PDFHendra SusantoNo ratings yet
- Psychoneuroimmunology 2Document3 pagesPsychoneuroimmunology 2bhasiNo ratings yet
- Psychoneuroimmunology Then and NowDocument18 pagesPsychoneuroimmunology Then and NowbhasiNo ratings yet
- Psychoneuroimmunology PDFDocument10 pagesPsychoneuroimmunology PDFRatu Nurul FadhilahNo ratings yet
- Stress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231Document7 pagesStress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231bhasiNo ratings yet
- Personality Coping Style and Constitutional NeuroimmunologyDocument6 pagesPersonality Coping Style and Constitutional NeuroimmunologybhasiNo ratings yet
- Psychoneuroimmunology Conditioning and Stress Ader20Conditioning20 20immunology20AnnRevPsy201993Document36 pagesPsychoneuroimmunology Conditioning and Stress Ader20Conditioning20 20immunology20AnnRevPsy201993bhasiNo ratings yet
- Biopsychosocial Aspects of Functional Gastrointestinal DisordersDocument15 pagesBiopsychosocial Aspects of Functional Gastrointestinal DisordersPedro LosadaNo ratings yet
- 2008 - Human PsychoneuroimmunologyDocument11 pages2008 - Human PsychoneuroimmunologybhasiNo ratings yet
- McDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFDocument9 pagesMcDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFCristian jimènezNo ratings yet
- The Association of Personality Traits and CopingDocument7 pagesThe Association of Personality Traits and CopingbhasiNo ratings yet
- ContentServer PDFDocument8 pagesContentServer PDFMaría Paula SierraNo ratings yet
- Psychoneuroimmunology 3Document21 pagesPsychoneuroimmunology 3bhasiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Personality Traits and Impaired Health-Related Quality of LifeDocument3 pagesPersonality Traits and Impaired Health-Related Quality of LifebhasiNo ratings yet
- Perceptual Style and Behavioral Pattern of Individuals - Cheng00-2Document9 pagesPerceptual Style and Behavioral Pattern of Individuals - Cheng00-2bhasiNo ratings yet
- The Association of Personality Traits and CopingDocument7 pagesThe Association of Personality Traits and CopingbhasiNo ratings yet
- Personality Coping Style and Constitutional NeuroimmunologyDocument6 pagesPersonality Coping Style and Constitutional NeuroimmunologybhasiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Psychosocial Aspects of The Functionalgastrointestinal DisordersDocument6 pagesPsychosocial Aspects of The Functionalgastrointestinal DisordersbhasiNo ratings yet
- Psychosocial Aspects of The Functionalgastrointestinal DisordersDocument6 pagesPsychosocial Aspects of The Functionalgastrointestinal DisordersbhasiNo ratings yet
- Stress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231Document7 pagesStress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231bhasiNo ratings yet
- Coping Flexibility, GI Symptoms, and Functional GI DisordersDocument4 pagesCoping Flexibility, GI Symptoms, and Functional GI DisordersbhasiNo ratings yet
- Functional Gastrointestinal Diseases and Psychological Maladjustment, Personality Traits and Quality of LifeDocument10 pagesFunctional Gastrointestinal Diseases and Psychological Maladjustment, Personality Traits and Quality of LifebhasiNo ratings yet
- From Music Making To Speaking - Engaging The Mirror Neuron System in AutismDocument8 pagesFrom Music Making To Speaking - Engaging The Mirror Neuron System in AutismbhasiNo ratings yet
- Irritable Bowel Byndrome Ibs PDFDocument15 pagesIrritable Bowel Byndrome Ibs PDFimuhammadfahmiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Learning With Individual-Interest Outcomes in Autism Spectrum DisorderDocument12 pagesLearning With Individual-Interest Outcomes in Autism Spectrum DisorderbhasiNo ratings yet
- Comparison of Personality Characteristics of Individuals With IBSDocument5 pagesComparison of Personality Characteristics of Individuals With IBSbhasiNo ratings yet
- From Music Making To Speaking - Engaging The Mirror Neuron System in AutismDocument8 pagesFrom Music Making To Speaking - Engaging The Mirror Neuron System in AutismbhasiNo ratings yet
- C1 Editable Quiz 3 - 0Document3 pagesC1 Editable Quiz 3 - 0Hiền Vũ Thị MaiNo ratings yet
- COVID-19 facts to share and dispel misinformationDocument2 pagesCOVID-19 facts to share and dispel misinformationanastacia arceNo ratings yet
- Ehlers-Danlos Panel: ExpertDocument17 pagesEhlers-Danlos Panel: ExpertMalika ButtNo ratings yet
- Aspen - EspenDocument38 pagesAspen - EspenJake BastoNo ratings yet
- STEM-19, Group 5-Topic No. 3Document3 pagesSTEM-19, Group 5-Topic No. 3Erwin Ranel ConstantinoNo ratings yet
- Detained Analysis of The Working of The OrganizationDocument10 pagesDetained Analysis of The Working of The OrganizationChin GeslaniNo ratings yet
- PRPDocument9 pagesPRPmutmainnah_kamilNo ratings yet
- Master Rotation PlanDocument21 pagesMaster Rotation PlanNeha Pandey SharmaNo ratings yet
- Covid-19 - PreventionDocument1 pageCovid-19 - PreventionKristel LavalleNo ratings yet
- NCP InfectionDocument3 pagesNCP InfectionPrince AhmirNo ratings yet
- Immediate Care of The NewbornDocument10 pagesImmediate Care of The NewbornRaffy100% (2)
- Minimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWDocument408 pagesMinimally Invasive Shoulder and Elbow Surgery - W. Levine, Et Al., (Informa, 2007) WWGeo SanchezNo ratings yet
- Comprehensive list of clinics and hospitals in a regionDocument184 pagesComprehensive list of clinics and hospitals in a regionMeera0% (1)
- Cupping/Hijama Times. 1 Issue: Section 3Document33 pagesCupping/Hijama Times. 1 Issue: Section 3Hala Elnouty78% (9)
- Merec Bulletin Vol15 No6Document4 pagesMerec Bulletin Vol15 No6n4dn4dNo ratings yet
- MelanomaDocument175 pagesMelanomaHelenaIbarraNo ratings yet
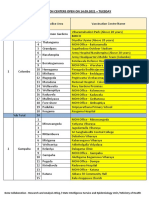
- Vaccination Centers On 14.09.2021Document8 pagesVaccination Centers On 14.09.2021Chanu On CTNo ratings yet
- HealthCarePersonnelExposedToHCV AlgorithmDocument2 pagesHealthCarePersonnelExposedToHCV Algorithmmmmaw mmNo ratings yet
- Four Square Step TestDocument2 pagesFour Square Step TestAnonymous igISmSUNo ratings yet
- Wound Care and Wound HealingDocument13 pagesWound Care and Wound Healingsusmisarkar28No ratings yet
- Early Beliefs & Practices: History of Nursing in The PhilippinesDocument11 pagesEarly Beliefs & Practices: History of Nursing in The PhilippinesJifford AbayonNo ratings yet
- FRM Patient View All ReportDocument1 pageFRM Patient View All ReportBeauty SinghNo ratings yet
- Indonesia Health Profile 2017Document474 pagesIndonesia Health Profile 2017Muhammad Aji MaulanaNo ratings yet
- Knowledge, Attitude and Practice Survey On Rabies in A Community in Sri LankaDocument36 pagesKnowledge, Attitude and Practice Survey On Rabies in A Community in Sri LankaGino C. MatibagNo ratings yet
- Dental Biofilm and Saliva Microbiome and Its Interplay With PDFDocument11 pagesDental Biofilm and Saliva Microbiome and Its Interplay With PDFGhimpu DanielaNo ratings yet
- Mengapa Biosecurity Menjadi Penting Pada Laboratorium Penyakit Infeksi ?Document10 pagesMengapa Biosecurity Menjadi Penting Pada Laboratorium Penyakit Infeksi ?AndyNo ratings yet
- Home Visit and Bag TechniqueDocument34 pagesHome Visit and Bag TechniqueEdralyn MatalangNo ratings yet
- P & G Purifier of Water - ReviewDocument2 pagesP & G Purifier of Water - ReviewjC HernandezNo ratings yet