You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Psychoneuroimmunology 2Document3 pagesPsychoneuroimmunology 2bhasiNo ratings yet
- Psychoneuroimmunology Then and NowDocument18 pagesPsychoneuroimmunology Then and NowbhasiNo ratings yet
- Psychoneuroimmunology PDFDocument10 pagesPsychoneuroimmunology PDFRatu Nurul FadhilahNo ratings yet
- Stress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231Document7 pagesStress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231bhasiNo ratings yet
- Personality Coping Style and Constitutional NeuroimmunologyDocument6 pagesPersonality Coping Style and Constitutional NeuroimmunologybhasiNo ratings yet
- Psychoneuroimmunology Conditioning and Stress Ader20Conditioning20 20immunology20AnnRevPsy201993Document36 pagesPsychoneuroimmunology Conditioning and Stress Ader20Conditioning20 20immunology20AnnRevPsy201993bhasiNo ratings yet
- Biopsychosocial Aspects of Functional Gastrointestinal DisordersDocument15 pagesBiopsychosocial Aspects of Functional Gastrointestinal DisordersPedro LosadaNo ratings yet
- 2008 - Human PsychoneuroimmunologyDocument11 pages2008 - Human PsychoneuroimmunologybhasiNo ratings yet
- McDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFDocument9 pagesMcDonald, Et Al., P. (2013) - Psychoneuroimmunology and Cancer PDFCristian jimènezNo ratings yet
- The Association of Personality Traits and CopingDocument7 pagesThe Association of Personality Traits and CopingbhasiNo ratings yet
- ContentServer PDFDocument8 pagesContentServer PDFMaría Paula SierraNo ratings yet
- Psychoneuroimmunology 3Document21 pagesPsychoneuroimmunology 3bhasiNo ratings yet
- Psychosocial Aspects of The Functionalgastrointestinal DisordersDocument6 pagesPsychosocial Aspects of The Functionalgastrointestinal DisordersbhasiNo ratings yet
- Personality Traits and Impaired Health-Related Quality of LifeDocument3 pagesPersonality Traits and Impaired Health-Related Quality of LifebhasiNo ratings yet
- Perceptual Style and Behavioral Pattern of Individuals - Cheng00-2Document9 pagesPerceptual Style and Behavioral Pattern of Individuals - Cheng00-2bhasiNo ratings yet
- The Association of Personality Traits and CopingDocument7 pagesThe Association of Personality Traits and CopingbhasiNo ratings yet
- Personality Coping Style and Constitutional NeuroimmunologyDocument6 pagesPersonality Coping Style and Constitutional NeuroimmunologybhasiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Psychological Issues in Inflammatory Bowel DiseaseDocument12 pagesPsychological Issues in Inflammatory Bowel DiseasebhasiNo ratings yet
- Stress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231Document7 pagesStress, Coping, and Immunologic Relevance - An Empirical Literature Review-JMedSci393107-2895197 - 080231bhasiNo ratings yet
- Comparison of Personality Characteristics of Individuals With IBSDocument5 pagesComparison of Personality Characteristics of Individuals With IBSbhasiNo ratings yet
- Psychosocial Aspects of The Functionalgastrointestinal DisordersDocument6 pagesPsychosocial Aspects of The Functionalgastrointestinal DisordersbhasiNo ratings yet
- From Music Making To Speaking - Engaging The Mirror Neuron System in AutismDocument8 pagesFrom Music Making To Speaking - Engaging The Mirror Neuron System in AutismbhasiNo ratings yet
- Coping Flexibility, GI Symptoms, and Functional GI DisordersDocument4 pagesCoping Flexibility, GI Symptoms, and Functional GI DisordersbhasiNo ratings yet
- Irritable Bowel Byndrome Ibs PDFDocument15 pagesIrritable Bowel Byndrome Ibs PDFimuhammadfahmiNo ratings yet
- Learning With Individual-Interest Outcomes in Autism Spectrum DisorderDocument12 pagesLearning With Individual-Interest Outcomes in Autism Spectrum DisorderbhasiNo ratings yet
- Exploration of Concomitant Psychiatric Disorders in Children With ASDDocument8 pagesExploration of Concomitant Psychiatric Disorders in Children With ASDbhasiNo ratings yet
- From Music Making To Speaking - Engaging The Mirror Neuron System in AutismDocument8 pagesFrom Music Making To Speaking - Engaging The Mirror Neuron System in AutismbhasiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Anal FissureDocument1 pageAnal Fissureshailesh284No ratings yet
- Male and Female Urinary Systems GuideDocument8 pagesMale and Female Urinary Systems Guideclaraenze mendozaNo ratings yet
- Module 8 Postpartum Stage Mercado Sibal IIIDocument13 pagesModule 8 Postpartum Stage Mercado Sibal IIIFrancisco Sibal IIINo ratings yet
- Fecal AnalysisDocument8 pagesFecal AnalysisMafie BarreiroNo ratings yet
- NCP For Impaired MobilityDocument4 pagesNCP For Impaired MobilityBettinaFernandoNo ratings yet
- Dross Man 2016Document5 pagesDross Man 2016Erna MiraniNo ratings yet
- Drug StudyDocument7 pagesDrug StudyKarol Ann RodriguezNo ratings yet
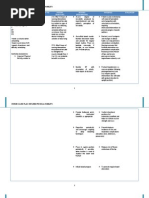
- Constipation NCP Nursing Care PlanDocument2 pagesConstipation NCP Nursing Care PlanLeizel Apolonio0% (1)
- Legendary Chinese Healing HerbsDocument164 pagesLegendary Chinese Healing HerbsLucas gabriel assis100% (6)
- May 30, 2014 Strathmore TimesDocument28 pagesMay 30, 2014 Strathmore TimesStrathmore TimesNo ratings yet
- Post Partum Assessment NCM 107 Care of Mother Child Adolescent Well Client Rle Skills LabDocument10 pagesPost Partum Assessment NCM 107 Care of Mother Child Adolescent Well Client Rle Skills Labskz19914No ratings yet
- Atsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanDocument24 pagesAtsp Re:: DR Gillian Jackson DR Fran Bennett DR Tom HannanSagarJobanNo ratings yet
- Rectal Cancer Case StudyDocument16 pagesRectal Cancer Case StudyIkenna Okpala100% (2)
- Case HirschsprungDocument29 pagesCase HirschsprungPriscila StevanniNo ratings yet
- ENEMADocument4 pagesENEMAMariah Alexis EncinaNo ratings yet
- Colace (Docusate Sodium)Document1 pageColace (Docusate Sodium)E100% (1)
- Dog and Cat Health SecretsDocument70 pagesDog and Cat Health SecretsIvana Dasović100% (1)
- Management of Cancer PatientsDocument10 pagesManagement of Cancer Patientswieka mawieNo ratings yet
- Bowel Management Following Spinal Cord InjuryDocument24 pagesBowel Management Following Spinal Cord InjuryBogdan PuscalauNo ratings yet
- Managing Rectal Pain Through Nursing InterventionsDocument2 pagesManaging Rectal Pain Through Nursing InterventionsJames Conrad SalengaNo ratings yet
- Art of Public Speaking 12th Edition Stephen Lucas Solutions ManualDocument35 pagesArt of Public Speaking 12th Edition Stephen Lucas Solutions Manualbeech.bouncerc4a995% (20)
- Essentials of Internal MedicineDocument832 pagesEssentials of Internal MedicineEmanuelMC100% (75)
- Bowel Training Guide for Constipation, Diarrhea and IrregularityDocument2 pagesBowel Training Guide for Constipation, Diarrhea and Irregularitydickie.gdrNo ratings yet
- Nursing Care Plan: Epidural Hematoma Post CraniotomyDocument14 pagesNursing Care Plan: Epidural Hematoma Post CraniotomyTepperoni78% (23)
- Sinclair2011 PDFDocument10 pagesSinclair2011 PDFAulia ZahraniNo ratings yet
- PNP HS MS FORM NO. 2014-01 medical history reportDocument4 pagesPNP HS MS FORM NO. 2014-01 medical history reportjames antonioNo ratings yet
- Stuck Up!!! - Case Report of A Rectal Foreign BodyDocument6 pagesStuck Up!!! - Case Report of A Rectal Foreign BodyIJAR JOURNALNo ratings yet
- Essential Procedures in Normal PregnancyDocument34 pagesEssential Procedures in Normal PregnancysenyorakathNo ratings yet
- Download ebook Ferris Clinical Advisor 2019 Pdf full chapter pdfDocument67 pagesDownload ebook Ferris Clinical Advisor 2019 Pdf full chapter pdfjohn.nelsen658100% (23)
- EnemaDocument62 pagesEnemaArlyn Mendenilla100% (2)