You might also like
- Antisocial Article2Document11 pagesAntisocial Article2mimirozmiza7No ratings yet
- Guiding PrinciplesDocument17 pagesGuiding PrinciplesLuna ValoNo ratings yet
- 2021 1-s2.0-S2352250X21000014-mainDocument6 pages2021 1-s2.0-S2352250X21000014-mainMubarak MansoorNo ratings yet
- Personality DisorderDocument33 pagesPersonality DisorderIulia Moldovan100% (1)
- Anxiety and Depression in Adults With AutismDocument14 pagesAnxiety and Depression in Adults With AutismNyah RodriguesNo ratings yet
- ADHD És ASD Kapcsolata Cikk AngolulDocument17 pagesADHD És ASD Kapcsolata Cikk AngolulGerlei-Tóth GabriellaNo ratings yet
- Anxiety and Depression. Autism in AdultsDocument14 pagesAnxiety and Depression. Autism in AdultsEdl ZsuzsiNo ratings yet
- Hunger: Mentalization-based Treatments for Eating DisordersFrom EverandHunger: Mentalization-based Treatments for Eating DisordersRating: 1 out of 5 stars1/5 (1)
- Literature Review On Antisocial Personality DisorderDocument8 pagesLiterature Review On Antisocial Personality DisorderklbndecndNo ratings yet
- Differential Diagnosis and Comorbidity Distinguishing Autism From Other Mental Health Issues NeuropsychiatryDocument11 pagesDifferential Diagnosis and Comorbidity Distinguishing Autism From Other Mental Health Issues NeuropsychiatryJohn Bowen BrownNo ratings yet
- A-Hudson, Hall & Harkness (2019)Document11 pagesA-Hudson, Hall & Harkness (2019)Jordanitha BhsNo ratings yet
- Personality Traits in Adolescents With Eating Disorder A Meta-Analytic Review (2019)Document17 pagesPersonality Traits in Adolescents With Eating Disorder A Meta-Analytic Review (2019)evellynNo ratings yet
- Autism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childFrom EverandAutism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childNo ratings yet
- Autism Spectrum Disorder: Outcomes in Adulthood: ReviewDocument8 pagesAutism Spectrum Disorder: Outcomes in Adulthood: ReviewRosa Indah KusumawardaniNo ratings yet
- Coocurrencias y Edad en El Diagnóstioco de AutismoDocument14 pagesCoocurrencias y Edad en El Diagnóstioco de Autismopsi.danae.hardingNo ratings yet
- Co-Occurring Psychiatric Conditions in Autism Spectrum DisordersDocument23 pagesCo-Occurring Psychiatric Conditions in Autism Spectrum DisordersPAULANo ratings yet
- (2017) The Treatment of Antisocial Personality DisorderDocument8 pages(2017) The Treatment of Antisocial Personality DisorderAarón ParedesNo ratings yet
- Brainsci 11 00924 v3Document15 pagesBrainsci 11 00924 v3Tanvi ManjrekarNo ratings yet
- NIH Public AccessDocument13 pagesNIH Public AccessJuan Alberto GonzálezNo ratings yet
- 1 s2.0 S1056499316301274 MainDocument26 pages1 s2.0 S1056499316301274 MainDavidNo ratings yet
- The Natural History of Antisocial Personality Disorder PDFDocument6 pagesThe Natural History of Antisocial Personality Disorder PDFGustavo FigueroaNo ratings yet
- Visual attention to social and non-social objects across the autism spectrumFrom EverandVisual attention to social and non-social objects across the autism spectrumNo ratings yet
- Literature Review Paper For Depression and SuicideDocument6 pagesLiterature Review Paper For Depression and SuicideJohn AjopeNo ratings yet
- Child Psychology Psychiatry - 2012 - Simonoff - Severe mood problems in adolescents with autism spectrum disorderDocument10 pagesChild Psychology Psychiatry - 2012 - Simonoff - Severe mood problems in adolescents with autism spectrum disorderlidiaNo ratings yet
- Outcome in ADHD 33years Later 2012Document18 pagesOutcome in ADHD 33years Later 2012GOLDFINCHNo ratings yet
- Inflexibility Processes As Predictors of Social Functioning in Chronic PsychosisDocument12 pagesInflexibility Processes As Predictors of Social Functioning in Chronic PsychosisifclarinNo ratings yet
- Borderline Personality Disorder and Emotion DysregulationDocument14 pagesBorderline Personality Disorder and Emotion Dysregulationme13No ratings yet
- Cognitive Distortions Questionnaire CD Quest PDFDocument8 pagesCognitive Distortions Questionnaire CD Quest PDFMelissa JaegerNo ratings yet
- A Review of Oppositional Defiant and Conduct DisordersDocument9 pagesA Review of Oppositional Defiant and Conduct DisordersStiven GonzalezNo ratings yet
- Balázs-2018 ADHD and NSSI in Adolescents - Clinical SampleDocument10 pagesBalázs-2018 ADHD and NSSI in Adolescents - Clinical SampleAMBAR L RODRIGUEZ-ARAUDNo ratings yet
- The Wiley Handbook of Disruptive and Impulse-Control DisordersFrom EverandThe Wiley Handbook of Disruptive and Impulse-Control DisordersNo ratings yet
- Zuhaida Hussein Et Al. - 2021 - Loneliness and Health Outcomes Among Malaysian Older AdultsDocument8 pagesZuhaida Hussein Et Al. - 2021 - Loneliness and Health Outcomes Among Malaysian Older AdultsSyara Shazanna ZulkifliNo ratings yet
- Prevalence and Predictors of Depression Amongst ElderlyDocument4 pagesPrevalence and Predictors of Depression Amongst ElderlyDr.Wajid Habib (Doxxsab)No ratings yet
- Content ServerDocument39 pagesContent ServerSérgio FonsecaNo ratings yet
- Woods 2021Document10 pagesWoods 2021Tristan TzaraNo ratings yet
- d41586-021-02690-5-1 (1)Document2 pagesd41586-021-02690-5-1 (1)Gab ArguellesNo ratings yet
- Personality Disorder and Changes in Affect Consciousness: A 3-Year Follow-Up Study of Patients With Avoidant and Borderline Personality DisorderDocument18 pagesPersonality Disorder and Changes in Affect Consciousness: A 3-Year Follow-Up Study of Patients With Avoidant and Borderline Personality Disorderyeremias setyawanNo ratings yet
- ADHD Linked to Peer Problems From Childhood to AdolescenceDocument8 pagesADHD Linked to Peer Problems From Childhood to AdolescenceJúlia JanoviczNo ratings yet
- Comorbidity Between ADHD and Anxiety Disorders Across The LifespanDocument8 pagesComorbidity Between ADHD and Anxiety Disorders Across The LifespanRubíPeñaNo ratings yet
- Mental Health of Chinese StudentsDocument9 pagesMental Health of Chinese StudentsCamilleNo ratings yet
- Miklowitz, 2019, Early Intervention For Youth at High Risk For Bipolar Disorder - A Multisite Randomized Trial of Family-Focused TreatmentDocument18 pagesMiklowitz, 2019, Early Intervention For Youth at High Risk For Bipolar Disorder - A Multisite Randomized Trial of Family-Focused TreatmentcristianNo ratings yet
- Developmental and Clinical Predictors of Comorbidity For Youth With OCDDocument7 pagesDevelopmental and Clinical Predictors of Comorbidity For Youth With OCDViktória Papucsek LelkesNo ratings yet
- Medical and Psychiatric ComorbiditiesDocument6 pagesMedical and Psychiatric ComorbiditiesDini indrianyNo ratings yet
- 2015 Collishaw Annual Research Review Secular Trends in Child and Adolescent Mental.Document24 pages2015 Collishaw Annual Research Review Secular Trends in Child and Adolescent Mental.cosma.alina2127No ratings yet
- Attention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyDocument9 pagesAttention Deficit Hyperactivity Disorder in Nepal: A Qualitative StudyNijan KhatiwadaNo ratings yet
- Literature Review Personality DisorderDocument8 pagesLiterature Review Personality Disorderxfeivdsif100% (1)
- Vigorous Physical Activity, Mental Health, Perceived Stress, and Socializing Among College StudentsDocument18 pagesVigorous Physical Activity, Mental Health, Perceived Stress, and Socializing Among College Studentshanna.oravecz1No ratings yet
- Clinical characteristics of high-functioning youth with ASD (2013)Document11 pagesClinical characteristics of high-functioning youth with ASD (2013)Heniger MariannNo ratings yet
- The Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsDocument7 pagesThe Influence of Gender On Social Anxiety Spectrum Symptoms in A Sample of University StudentsGeorge WinchesterNo ratings yet
- Fpsyg 08 00454Document13 pagesFpsyg 08 00454mvoulkouNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptKc RiveraNo ratings yet
- A Prospective, Longitudinal, Study of Men With Borderline Personality Disorder With and Without Comorbid Antisocial Personality DisorderDocument13 pagesA Prospective, Longitudinal, Study of Men With Borderline Personality Disorder With and Without Comorbid Antisocial Personality DisorderJuan BacelarNo ratings yet
- Int J Geriat Psychiatry - 2006 - Lynch - Treatment of older adults with co‐morbid personality disorder and depression aDocument13 pagesInt J Geriat Psychiatry - 2006 - Lynch - Treatment of older adults with co‐morbid personality disorder and depression aJulieta AzevedoNo ratings yet
- How Information Processing Problems May Affect Psychotherapy for Adults with LD or ADHDDocument10 pagesHow Information Processing Problems May Affect Psychotherapy for Adults with LD or ADHDRosalinda RizzoNo ratings yet
- Personality Disorders in AdolescenceDocument2 pagesPersonality Disorders in AdolescenceMale BajoNo ratings yet
- Psychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesDocument9 pagesPsychiatric and Medical Correlates of DSM-5 Eating Disorders in A Nationally Representative Sample of Adults in The United StatesManny RosengallegosNo ratings yet
- A Literature Analysis On The Quality of Life in Adults With AutismDocument11 pagesA Literature Analysis On The Quality of Life in Adults With AutismPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Major Depressive Disorder in Children and Adolescents: Sandra Mullen, Pharmd, BCPPDocument9 pagesMajor Depressive Disorder in Children and Adolescents: Sandra Mullen, Pharmd, BCPPbogdancoticaNo ratings yet
- Studiu PsihoDocument42 pagesStudiu PsihoCarmenAlinaNo ratings yet
- Angeles, Los Angeles, CaliforniaDocument1 pageAngeles, Los Angeles, CaliforniaJohn Loyd AlcasidNo ratings yet
- Drug and Alcohol DependenceDocument8 pagesDrug and Alcohol DependenceAarón ParedesNo ratings yet
- 2021 Can Approaching Anxiety Like A Habit Lead To Novel TreatmentsDocument6 pages2021 Can Approaching Anxiety Like A Habit Lead To Novel TreatmentsAarón ParedesNo ratings yet
- 2022 Mindfulness-Based Programs Why, When, and How To AdaptDocument12 pages2022 Mindfulness-Based Programs Why, When, and How To AdaptAarón Paredes100% (1)
- Wittgenstein's Philosophical Investigations - Text and ContextDocument256 pagesWittgenstein's Philosophical Investigations - Text and ContextAarón ParedesNo ratings yet
- 2019 Quitting Starts in The Brain A Randomized Controlled Trial of App-Based Mindfulness Shows Decreases in Neural Responses To Smoking Cues That Predict Reductions in SmokingDocument8 pages2019 Quitting Starts in The Brain A Randomized Controlled Trial of App-Based Mindfulness Shows Decreases in Neural Responses To Smoking Cues That Predict Reductions in SmokingAarón ParedesNo ratings yet
- (2019) Antisocial Personality DisorderDocument8 pages(2019) Antisocial Personality DisorderAarón ParedesNo ratings yet
- Neuroadaptive processes in GABAergic and glutamatergic systems in benzodiazepine dependenceDocument25 pagesNeuroadaptive processes in GABAergic and glutamatergic systems in benzodiazepine dependenceAarón ParedesNo ratings yet
- (1998) - Benzodiazepine Dependence From Neural Circuits To Gene Expression.Document10 pages(1998) - Benzodiazepine Dependence From Neural Circuits To Gene Expression.Aarón ParedesNo ratings yet
- 2021 Clinical Efficacy and Psychological Mechanisms of An App-Based Digital Therapeutic For Generalized Anxiety DisorderRandomized Controlled TrialDocument18 pages2021 Clinical Efficacy and Psychological Mechanisms of An App-Based Digital Therapeutic For Generalized Anxiety DisorderRandomized Controlled TrialAarón ParedesNo ratings yet
- (2017) The Treatment of Antisocial Personality DisorderDocument8 pages(2017) The Treatment of Antisocial Personality DisorderAarón ParedesNo ratings yet
- Bipolar 3Document13 pagesBipolar 3rinaratnaNo ratings yet
- (2018) Antisocial Personality TraitsDocument5 pages(2018) Antisocial Personality TraitsAarón ParedesNo ratings yet
- (2018) Characteristics of Depressive and Bipolar Disorder Patients With Mixed FeaturesDocument10 pages(2018) Characteristics of Depressive and Bipolar Disorder Patients With Mixed FeaturesAarón ParedesNo ratings yet
- Bipolar 3Document13 pagesBipolar 3rinaratnaNo ratings yet
- (2010) - Effectively Detect Dependence On Benzodiazepines Among Community-Dwelling Seniors by Asking Only Two Questions.Document7 pages(2010) - Effectively Detect Dependence On Benzodiazepines Among Community-Dwelling Seniors by Asking Only Two Questions.Aarón ParedesNo ratings yet
- (2017) Mixed Features in Bipolar DisorderDocument7 pages(2017) Mixed Features in Bipolar DisorderAarón ParedesNo ratings yet
- (2018) - Biological Markers of Generalized Anxiety Disorder.Document9 pages(2018) - Biological Markers of Generalized Anxiety Disorder.Aarón ParedesNo ratings yet
- BZDP GuidelineDocument13 pagesBZDP GuidelinejjjjjNo ratings yet
- (2017) Mixed Features in Bipolar DisorderDocument7 pages(2017) Mixed Features in Bipolar DisorderAarón ParedesNo ratings yet
- (2018) - A Review of The Neurobiological Basis of Trauma-Related Dissociation and Its Relation To Cannabinoid - and Opioid-Mediated Stress ResponseDocument14 pages(2018) - A Review of The Neurobiological Basis of Trauma-Related Dissociation and Its Relation To Cannabinoid - and Opioid-Mediated Stress ResponseAarón ParedesNo ratings yet
- (2018) Characteristics of Depressive and Bipolar Disorder Patients With Mixed FeaturesDocument10 pages(2018) Characteristics of Depressive and Bipolar Disorder Patients With Mixed FeaturesAarón ParedesNo ratings yet
- (2018) Risks and Benefits of Medications For Panic Disorder A Comparison of SSRIs and BenzodiazepinesDocument11 pages(2018) Risks and Benefits of Medications For Panic Disorder A Comparison of SSRIs and BenzodiazepinesAarón ParedesNo ratings yet
- Memory Reconsolidation and Emotional Arousal in PsychotherapyDocument80 pagesMemory Reconsolidation and Emotional Arousal in PsychotherapyAarón ParedesNo ratings yet
- 2017 The Place of Antipsychotics in The Therapy of Anxiety Disorders and OCD DisordersDocument11 pages2017 The Place of Antipsychotics in The Therapy of Anxiety Disorders and OCD DisordersAarón ParedesNo ratings yet
- Sepede, (2018) - Efficacy and Safety of Atypical Antipsychotics in Bipolar Disorder With Comorbid Substance Dependence.Document11 pagesSepede, (2018) - Efficacy and Safety of Atypical Antipsychotics in Bipolar Disorder With Comorbid Substance Dependence.Aarón ParedesNo ratings yet
- (2019) - Trends and Factors in Antipsychotic Use of Outpatients With Anxiety Disorders in Taiwan, 2005-2013Document7 pages(2019) - Trends and Factors in Antipsychotic Use of Outpatients With Anxiety Disorders in Taiwan, 2005-2013Aarón ParedesNo ratings yet
- Memory Reconsolidation and Emotional Arousal in PsychotherapyDocument80 pagesMemory Reconsolidation and Emotional Arousal in PsychotherapyAarón ParedesNo ratings yet
- (2017) - Anxiety Disorders A Review of Current LiteratureDocument2 pages(2017) - Anxiety Disorders A Review of Current LiteratureAarón ParedesNo ratings yet
- Salloum, (2017) - Management of Comorbid Bipolar Disorder and Substance Use Disorders.Document12 pagesSalloum, (2017) - Management of Comorbid Bipolar Disorder and Substance Use Disorders.Aarón ParedesNo ratings yet
- Belazo Elastomeric Roof PaintDocument2 pagesBelazo Elastomeric Roof PaintrumahsketchNo ratings yet
- Waste Management in Vienna. MA 48Document12 pagesWaste Management in Vienna. MA 484rtttt4ttt44No ratings yet
- Ex 2013 1 (Recurrent)Document30 pagesEx 2013 1 (Recurrent)alh basharNo ratings yet
- Buckling TestDocument11 pagesBuckling Testsharusli100% (1)
- Rational Use of AntibioticsDocument35 pagesRational Use of AntibioticsRahul SharmaNo ratings yet
- PDM TempDocument2 pagesPDM Tempamit rajputNo ratings yet
- Bipolar I Disorder Case ExampleDocument6 pagesBipolar I Disorder Case ExampleGrape JuiceNo ratings yet
- Shangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Document2 pagesShangqiu Jinpeng Industrial Co., LTD.: Widely Used Waste Rubber Pyrolysis Equipment (XY-7)Salma FarooqNo ratings yet
- Guía de Instalación y Programación: Sistema de Seguridad de 32 ZonasDocument68 pagesGuía de Instalación y Programación: Sistema de Seguridad de 32 ZonasfernanfivNo ratings yet
- Miniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDocument4 pagesMiniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDenis CarlosNo ratings yet
- Mathematical Structures of The UniverseDocument228 pagesMathematical Structures of The UniverseMaki MajomNo ratings yet
- Chapter 3Document58 pagesChapter 3hasanNo ratings yet
- Material ManagementDocument106 pagesMaterial ManagementRomi AfriansyahNo ratings yet
- Quarter 1-Module 2 Modern ArtDocument20 pagesQuarter 1-Module 2 Modern ArtKimberly Trocio Kim100% (1)
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
- Module 2 Chem 1Document25 pagesModule 2 Chem 1melissa cabreraNo ratings yet
- HymssheetDocument4 pagesHymssheettoby_wardmanNo ratings yet
- Chapter 1 and 2Document67 pagesChapter 1 and 2Tle SupawidNo ratings yet
- AAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)Document3 pagesAAB 075323 EPDM Waterproofing Membrane (For RC Roof Build-Up Inc. Insulation)tewodrosNo ratings yet
- Factors to Consider in Reactor Design for Industrial ProcessesDocument3 pagesFactors to Consider in Reactor Design for Industrial Processesuma villashini100% (2)
- Melese Hotel ST ReportDocument74 pagesMelese Hotel ST ReportKidist MollaNo ratings yet
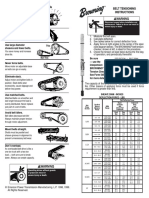
- Browning Belt Tension GaugeDocument2 pagesBrowning Belt Tension GaugeJasperken2xNo ratings yet
- What Is A Supply ChainDocument20 pagesWhat Is A Supply ChainThanh Binh Tran NguyenNo ratings yet
- Beneficiation of Cassiterite From Primary Tin OresDocument11 pagesBeneficiation of Cassiterite From Primary Tin OresSULMAGNo ratings yet
- Stabil Drill Roller ReamersDocument2 pagesStabil Drill Roller ReamersIMEDHAMMOUDANo ratings yet
- Estimation of Fabric Opacity by ScannerDocument7 pagesEstimation of Fabric Opacity by ScannerJatiKrismanadiNo ratings yet
- Rate Analysis-Norms 1Document10 pagesRate Analysis-Norms 1yamanta_rajNo ratings yet
- K2N Final Internship ReportDocument55 pagesK2N Final Internship ReportAceZeta0% (1)
- High Pressure Processing For Preservation of FoodsDocument36 pagesHigh Pressure Processing For Preservation of FoodsPravin Zine PatilNo ratings yet
- ISO 14000 - WikipediaDocument5 pagesISO 14000 - WikipediaalexokorieNo ratings yet