You might also like
- Med Surg RevDocument14 pagesMed Surg RevSamantha VeraNo ratings yet
- Bmed Concept MapDocument2 pagesBmed Concept Mapapi-247954649No ratings yet
- Med Surg 2 - 10 Nursing Care of Clients With Biliary DisordersDocument4 pagesMed Surg 2 - 10 Nursing Care of Clients With Biliary DisordersMaxinne RoseñoNo ratings yet
- Psychiatric Nursing Bullets Neurotransmission TheoryDocument4 pagesPsychiatric Nursing Bullets Neurotransmission TheoryDefensor Pison Gringgo100% (1)
- SBARQ FormDocument1 pageSBARQ FormTracy100% (5)
- Presented By: Anjani.S.Kamal 1 Year MSC (N)Document23 pagesPresented By: Anjani.S.Kamal 1 Year MSC (N)shubham vermaNo ratings yet
- FAELDONEA - B. Concept MapDocument1 pageFAELDONEA - B. Concept MapPatricia Jean FaeldoneaNo ratings yet
- Quiz 1 Med Surg SummerDocument8 pagesQuiz 1 Med Surg SummerMc Harris VinasoyNo ratings yet
- Review On Peripheral IV FluidsDocument37 pagesReview On Peripheral IV FluidsWoot RootNo ratings yet
- Sample: Duquesne University School of Nursing Care Map TemplateDocument6 pagesSample: Duquesne University School of Nursing Care Map TemplateDevin Nikole BlattnerNo ratings yet
- Pharmacotherapy of - Benign Prostatic HyperplasiaDocument4 pagesPharmacotherapy of - Benign Prostatic HyperplasiaBaarid HamidiNo ratings yet
- Diagnosis Schizophrenia 2Document1 pageDiagnosis Schizophrenia 2Bukola OgunnaikeNo ratings yet
- Arf NotesDocument28 pagesArf NotesEllen Hennings100% (1)
- System Disorder: Renal CalculiDocument1 pageSystem Disorder: Renal CalculiHolly DeckelmanNo ratings yet
- Final Coaching DrugsDocument8 pagesFinal Coaching DrugsSherlyn BesasNo ratings yet
- Endocrine MedicationsDocument47 pagesEndocrine MedicationsAamir AzizNo ratings yet
- Blood PanelsDocument7 pagesBlood Panelslisalov100% (1)
- Conflict PresentationDocument19 pagesConflict Presentationapi-231905851No ratings yet
- Pneumonia Cheat Sheet: by ViaDocument3 pagesPneumonia Cheat Sheet: by ViaGayle MarieNo ratings yet
- Chronic Renal FailureDocument7 pagesChronic Renal Failuretantalizin marieNo ratings yet
- Completed Concept MapDocument4 pagesCompleted Concept Mapapi-607361848No ratings yet
- CHF Concept MapDocument1 pageCHF Concept MapChristy Wegner Cooper100% (4)
- O Insert Picture Here From Slide: Heart Failure Heart FailureDocument4 pagesO Insert Picture Here From Slide: Heart Failure Heart FailureAlec Xavier MirandaNo ratings yet
- Cardiac Pre Class Minilecture Lewis 10-2018-2Document27 pagesCardiac Pre Class Minilecture Lewis 10-2018-2Jasmine LiraNo ratings yet
- Electrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionDocument6 pagesElectrolyte Imbalance Cause Signs and Symptoms Intervention ConnectionmkninnyNo ratings yet
- Case Simu 101Document5 pagesCase Simu 101Princess Levie CenizaNo ratings yet
- LasixDocument1 pageLasixKatie McPeek100% (2)
- Cardiovascular Pharmacology OutlineDocument11 pagesCardiovascular Pharmacology OutlineLhay de OcampoNo ratings yet
- ETOH Case StudyDocument5 pagesETOH Case StudyCharme Jean RaygonNo ratings yet
- Lec-4 Upper and Lower Git DisordersDocument101 pagesLec-4 Upper and Lower Git DisordersSaher YasinNo ratings yet
- Clinical Medication WorksheetDocument1 pageClinical Medication WorksheetSrkocher100% (1)
- Guide To Diabetes MedicationsDocument2 pagesGuide To Diabetes MedicationsJianhua ShiNo ratings yet
- Case Study Skin IntegrityDocument3 pagesCase Study Skin IntegrityTraci VanOss100% (1)
- Invega+Sustenna PiDocument18 pagesInvega+Sustenna PiMaal AbrarNo ratings yet
- Medsurg ReviewDocument34 pagesMedsurg ReviewestberryNo ratings yet
- Pharmacology of AntimycobacterialDocument7 pagesPharmacology of Antimycobacterialselflessdoctor100% (1)
- Comprehensive Nursing Assessment For Care Plan: AllergiesDocument14 pagesComprehensive Nursing Assessment For Care Plan: AllergiesBrittany ShrewsburyNo ratings yet
- Sirs & ModsDocument5 pagesSirs & Modsmarlou agananNo ratings yet
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Maladaptive Patterns of Behavior A. AnxietyDocument19 pagesMaladaptive Patterns of Behavior A. AnxietyTeal OtterNo ratings yet
- Introduction To Nursing PharmacologyDocument97 pagesIntroduction To Nursing PharmacologyLiel TorresNo ratings yet
- Go Green for Wellness: Smoothies, Juices, Green Recipes: Practical Advice for Achieving Good HealthFrom EverandGo Green for Wellness: Smoothies, Juices, Green Recipes: Practical Advice for Achieving Good HealthNo ratings yet
- BL ChartDocument10 pagesBL ChartElizabeth Durkee NeilNo ratings yet
- Addison Vs CushingsDocument1 pageAddison Vs CushingsChris ZantiraNo ratings yet
- NR 446 Week 6 ATI Weekly Tips Mental HealthDocument16 pagesNR 446 Week 6 ATI Weekly Tips Mental HealthChristine LansdownNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- TMendoza CriticalCareConceptMap2Document5 pagesTMendoza CriticalCareConceptMap2Theresa Fernandez Mendoza0% (1)
- Concept Map CholesectomyDocument3 pagesConcept Map CholesectomyDoreen Claire100% (1)
- 201103-Fkg-Drugs Act On Cardiovascular SystemDocument19 pages201103-Fkg-Drugs Act On Cardiovascular SystemEidelen Lovani Sembiring100% (1)
- Non Alcoholic Fatty Liver DiseaseDocument219 pagesNon Alcoholic Fatty Liver DiseaseAlwiNo ratings yet
- Heart Muscle Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHeart Muscle Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Medication - ALT-Template - Enoxaparin SodiumDocument1 pageMedication - ALT-Template - Enoxaparin SodiumNancyAmissahNo ratings yet
- Adrenal Insufficiency and Addison's DiseaseDocument8 pagesAdrenal Insufficiency and Addison's DiseaseyancefinceNo ratings yet
- Meds For HypertensionDocument3 pagesMeds For HypertensionZonicsNo ratings yet
- EclampsiaDocument56 pagesEclampsiagalihtrimuninggarNo ratings yet
- 2017 Fluid and Electrolytes LECTURE NOTESDocument34 pages2017 Fluid and Electrolytes LECTURE NOTESHarley Justiniani Dela CruzNo ratings yet
- Alterations in VentilationDocument10 pagesAlterations in VentilationCharisma Pastor100% (1)
- Metabolic DisturbancesDocument34 pagesMetabolic DisturbancesKyle DapulagNo ratings yet
- Comprehensive Exam in Nursing Part 3Document40 pagesComprehensive Exam in Nursing Part 3Ariane-Gay Cristobal Duran100% (1)
- Acute Pain Related Multiple Physical Injury AEB Pain Scale of 4/10 andDocument5 pagesAcute Pain Related Multiple Physical Injury AEB Pain Scale of 4/10 andAriane-Gay Cristobal DuranNo ratings yet
- Spicy Caribbean Sauce Spicy Caribbean SauceDocument2 pagesSpicy Caribbean Sauce Spicy Caribbean SauceAriane-Gay Cristobal DuranNo ratings yet
- Equipments Purpose Top of Emergency TrolleyDocument41 pagesEquipments Purpose Top of Emergency TrolleyAriane-Gay Cristobal DuranNo ratings yet
- DescriptionDocument1 pageDescriptionAriane-Gay Cristobal DuranNo ratings yet
- Comprehensive Exam in Nursing Part 2Document41 pagesComprehensive Exam in Nursing Part 2Ariane-Gay Cristobal DuranNo ratings yet
- NursesDocument1 pageNursesAriane-Gay Cristobal DuranNo ratings yet
- Comprehensive Exam in Nursing Part 1Document36 pagesComprehensive Exam in Nursing Part 1Ariane-Gay Cristobal DuranNo ratings yet
- Chapter 20 Module Schizophrenia and Other PsychosisDocument5 pagesChapter 20 Module Schizophrenia and Other PsychosisAriane-Gay Cristobal DuranNo ratings yet
- Module 08 Day 9 UNIT V EDUCTIONDocument7 pagesModule 08 Day 9 UNIT V EDUCTIONAriane-Gay Cristobal DuranNo ratings yet
- Movie Viewing Guides in NCM 117 RleDocument2 pagesMovie Viewing Guides in NCM 117 RleAriane-Gay Cristobal DuranNo ratings yet
- Chapter 13 Module CrisisDocument3 pagesChapter 13 Module CrisisAriane-Gay Cristobal DuranNo ratings yet
- Metabolic Disorders PowerpointDocument48 pagesMetabolic Disorders PowerpointJamesNo ratings yet
- Nursing Care Management of Clients With Gastrointestinal DisordersDocument50 pagesNursing Care Management of Clients With Gastrointestinal DisordersAriane-Gay Cristobal DuranNo ratings yet
- Module 07 Day 8 UNIT V OPPOSITIONAL INFERENCEDocument5 pagesModule 07 Day 8 UNIT V OPPOSITIONAL INFERENCEAriane-Gay Cristobal DuranNo ratings yet
- Meaning of Judgment and PropositionsDocument9 pagesMeaning of Judgment and PropositionsAriane-Gay Cristobal DuranNo ratings yet
- Thyroid-Gland 2Document12 pagesThyroid-Gland 2Ariane-Gay Cristobal DuranNo ratings yet
- Diabetes InsipidusDocument60 pagesDiabetes Insipidusperie_md100% (1)
- Diabetes InsipidusDocument48 pagesDiabetes InsipidusAhmed Fraz MamoonNo ratings yet
- Ms. Nicole Nathalie R. Sumabat, RN: BSN 3-B (Group 4)Document124 pagesMs. Nicole Nathalie R. Sumabat, RN: BSN 3-B (Group 4)Ariane-Gay Cristobal DuranNo ratings yet
- Unit Ii: Introduction To Logic: Subtopic 1: The Meaning of LogicDocument4 pagesUnit Ii: Introduction To Logic: Subtopic 1: The Meaning of LogicAriane-Gay Cristobal DuranNo ratings yet
- Module 08 Day 9 UNIT V EDUCTION 3Document7 pagesModule 08 Day 9 UNIT V EDUCTION 3Ariane-Gay Cristobal DuranNo ratings yet
- Chapter 12 Module AbuseDocument3 pagesChapter 12 Module AbuseAriane-Gay Cristobal DuranNo ratings yet
- Function and Regulation of Hormones Hormones: Small Lobules of Compound Gland)Document11 pagesFunction and Regulation of Hormones Hormones: Small Lobules of Compound Gland)Ariane-Gay Cristobal DuranNo ratings yet
- Instructions Only, You May Remove It Arial 11 No Bold Text Remove Italic Text Convert It in PDF (Output Name Format: Group No., Psychassessmenttool)Document24 pagesInstructions Only, You May Remove It Arial 11 No Bold Text Remove Italic Text Convert It in PDF (Output Name Format: Group No., Psychassessmenttool)Ariane-Gay Cristobal DuranNo ratings yet
- Chapter 5 Module Adjustive MechanismDocument3 pagesChapter 5 Module Adjustive MechanismAriane-Gay Cristobal DuranNo ratings yet
- School of Health and Natural Sciences Nursing Department Bayombong, Nueva VizcayaDocument20 pagesSchool of Health and Natural Sciences Nursing Department Bayombong, Nueva VizcayaAriane-Gay Cristobal DuranNo ratings yet
- Chapter 18 Module Mood DisorderDocument6 pagesChapter 18 Module Mood DisorderAriane-Gay Cristobal DuranNo ratings yet
- Module SuctioningDocument25 pagesModule SuctioningAriane-Gay Cristobal DuranNo ratings yet
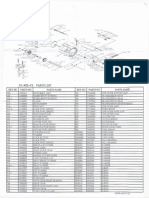
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Design Guide For Overhead CranesDocument3 pagesDesign Guide For Overhead CranesralluinNo ratings yet
- Caps Fet Physical Science WebbbbDocument170 pagesCaps Fet Physical Science WebbbbWonder Bee NzamaNo ratings yet
- Last Voyage of Somebody The Sailor The SailorDocument581 pagesLast Voyage of Somebody The Sailor The SailorDelia Ungureanu50% (2)
- Phy Interface Pci Express Sata Usb31 Architectures Ver43 PDFDocument99 pagesPhy Interface Pci Express Sata Usb31 Architectures Ver43 PDFRaj Shekhar ReddyNo ratings yet
- Magellan 8300Document540 pagesMagellan 8300Fleming AlexanderNo ratings yet
- Cavinkare Private LimitedDocument4 pagesCavinkare Private LimitedRohit TrivediNo ratings yet
- Ready. Set. IELTS. Idioms.Document45 pagesReady. Set. IELTS. Idioms.Renatochka BakirovaNo ratings yet
- Kompilasi Soal Paket BDocument10 pagesKompilasi Soal Paket Babdul wahidNo ratings yet
- Competency Based Learning Materials: Housekeeping NciiDocument54 pagesCompetency Based Learning Materials: Housekeeping NciiNickolodian AsuncionNo ratings yet
- NMRDocument135 pagesNMRKhan Sameer100% (1)
- Server Preparation Details LinuxDocument9 pagesServer Preparation Details Linuxbharatreddy9No ratings yet
- MGT-01 (14.03.23) - QPDocument19 pagesMGT-01 (14.03.23) - QPSrinivas VakaNo ratings yet
- Literature Review Topics RadiographyDocument8 pagesLiterature Review Topics Radiographyea7w32b0100% (1)
- 1.2. Types of Bank: Dhruba Koirala National Law CollegeDocument38 pages1.2. Types of Bank: Dhruba Koirala National Law CollegeMadan ShresthaNo ratings yet
- Math10 q2 Week1 Module1 Polynomial-Functions For-ReproductionDocument32 pagesMath10 q2 Week1 Module1 Polynomial-Functions For-ReproductionChaz grant borromeo89% (9)
- Gerry Mulligan DiscographyDocument491 pagesGerry Mulligan DiscographyIan SinclairNo ratings yet
- Past:: Simple Indefinite Continuous Perfect Perfect ContinuousDocument12 pagesPast:: Simple Indefinite Continuous Perfect Perfect ContinuousAhmed Abd El HafeezNo ratings yet
- Type Italian Characters - Online Italian KeyboardDocument3 pagesType Italian Characters - Online Italian KeyboardGabriel PereiraNo ratings yet
- Twinmotion 2016 Edition Full CrackDocument3 pagesTwinmotion 2016 Edition Full CrackGivi Andriyanto0% (1)
- Probability Practice QuesDocument9 pagesProbability Practice QuesYamu HiadeenNo ratings yet
- 2 - ARM Cotex-M3 - IntroductionDocument124 pages2 - ARM Cotex-M3 - IntroductionNghĩa VũNo ratings yet
- Case Study-Cereal PartnersDocument5 pagesCase Study-Cereal PartnersTariq MehmoodNo ratings yet
- PIRCHLDocument227 pagesPIRCHLapi-3703916No ratings yet
- Test Method of Flammability of Interior Materials For AutomobilesDocument17 pagesTest Method of Flammability of Interior Materials For AutomobilesKarthic BhrabuNo ratings yet
- Cost ActivityDocument6 pagesCost ActivityDeepak PahujaNo ratings yet
- XDM-100 IOM SDH A00 4-5 enDocument334 pagesXDM-100 IOM SDH A00 4-5 endilipgulatiNo ratings yet
- PRACTICES AND CHALLENGES IN THE IMPLEMENTATION OF BASIC EDUCATION LEARNING CONTINUITY PLAN-Authored By: Reynaldo C. CruzDocument71 pagesPRACTICES AND CHALLENGES IN THE IMPLEMENTATION OF BASIC EDUCATION LEARNING CONTINUITY PLAN-Authored By: Reynaldo C. CruzInternational Intellectual Online PublicationsNo ratings yet
- Oops MCQ (Unit-1)Document7 pagesOops MCQ (Unit-1)Jee Va Ps86% (14)
- Prologue: Managerial Accounting and The Business EnvironmentDocument156 pagesPrologue: Managerial Accounting and The Business EnvironmentMarcus MonocayNo ratings yet