Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Formulation and Evaluation of Antimicrobial
Mucoadhesive Dental Gel of Aerial Root
of Ficus Benghalensis L to Enhance
the Therapeutic Activity using Clove Oil
S.Janani1*, S.P.Senthil2, R.Senthamarai3
1
Post graduate Student, 2Guide & Head, 3Principal
Department of Pharmacognosy,
Periyar college of pharmaceutical sciences,
Tiruchirappalli, Tamilnadu, India
Abstract:- The main purpose of the research is to thus a diet high in simple sugar is a risk factor. Diabetes
develop and evaluate a dental gel containing a herbal mellitus, Sjogren syndrome, and certain drugs are all risk
medicine for the management of toothache. The factors for dry mouth. Antihistamines and antidepressants
ethanolic extract of aerial root of Ficus benghalensis was are two medications that reduce saliva production.Caries is a
prepared and it was evaluated for organoleptice Latin term that means "rottenness."[4].
properties, pH and phytochemical screening.
Antimicrobial activity of the extract was done against Four things are required for caries to form: a tooth
streptococcus mutans using well diffusion method. The surface (enamel or dentin), caries-causing bacteria,
gel was prepared using Carbopol, propylene glycol and fermentable carbohydrates (such as sucrose), and time. This
clove oil as a permeation enhancer. Six gel formulations is caused by food sticking to the teeth and the bacteria that
were prepared at two different grades and various make up dental plaque producing acid. Biofilm (dental
concentration of Carbopol. The formulations were plaque) that forms on the teeth and matures into cariogenic
evaluated for different parameters such as appearance, bacteria causes tooth decay (causingdecay). In the presence
pH, viscosity, spreadability. Theoptimizedbatchwas of fermentable carbohydrates such as sucrose, fructose, and
subjected to further studies via. drug content, stability glucose, certain bacteria in the biofilm produce acid [5-11].
testing, diffusion study to determine percent cumulative
release of drug from gel formulations and antimicrobial The mutans streptococci, commonly Streptococcus
study. From the antimicrobial study, it was observed the mutans, Streptococcus sobrinus, and Lactobacilli, are the
optimized formulation and marketed formulation microorganisms most commonly associated with dental
produced almost equal zone of inhibition. The evaluation cavities.Although there are many different types of oral
parameters of optimized batch indicate that the bacteria in the mouth, only a few are considered to be
prepared dental gel is stable, good drug delivery system responsible for dental caries: Among them are Lactobacillus
and contains antimicrobial agents for the prevention of species and Streptococcus mutans. Untreated dental caries
dental caries and management of tooth ache. can have a negative impact on one's quality of life due to
pain, discomfort, tooth loss, and poor oral function. [12].
Keywords:- Aerial root, Ficus benghalensis, clove oil, Pain defines, it is an “unpleasant sensory and emotional
dental gel, Carbopol. experience associated with actual or potential tissue
damage”.Dental pain is a common symptom of a variety of
I. INTRODUCTION dental diseases, including dental caries, and it has a major
impact on oral health-related quality of life[13,14].
The human teeth function to mechanically break down
items of food by cutting and crushing them in preparation Patients with tooth pain are generally afraid to take
for swallowing and digesting. The tooth is one of the body's pharmaceutical medicines, instead that preferring to use
most unique and complex anatomical and histological natural therapies because of their proven efficacy and safety
components.The deterioration of teeth caused by acids in all age groups.Some studies suggested that the natural
produced by bacteria is known as tooth decay, often known herbs can help to prevent the tooth decay and manage the
as cavities or caries. The cavities appearin different colours tooth ache[15]. The aerial root of Ficus benghalensis has the
ranging from yellow to black. Pain and eating difficulties are potent antimicrobial activity which is used for the
common symptoms [1,2]. Inflammation of the gum tissue prevention and treatment of dental plaque, dental caries and
around the tooth, tooth loss, infection, and abscess formation periodontitis.
are all possible complications.
Clove oil is a multipurpose oil that has gained
The cause of cavities is acid from bacteria dissolving considerable attention in dentistry due to its numerous
the hard tissues of the teeth (enamel, dentin and benefits. Clove oil has a wide range of biological activities,
cementum)[3].Whenever bacteria break down food particles including analgesics, antiseptics, antispasmodics, anti-
or sugar on the tooth surface, they produce acid. Simple neuralgics, carminatives, anti-infectious, disinfectant,
sugars in food are these bacteria's primary energy source and insecticide, stimulant, stomachic, and others[16].
IJISRT22MAY890 www.ijisrt.com 1066
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
coarse powder after drying in the shade. The preparation of
The goal of this study was to develop a dental gel successive solvent extracts was the first step in the process.
containing an extract of Ficus benghalensis aerial root and The dried coarsely powdered sample of Ficus benghalensis
clove oil, which acts as a permeation enhancer. (90g) was first extracted with petroleum ether (60-80◦ C)
using Soxhlet apparatus and then extracted with ethanol.
II. MATERIALS AND METHODS The extract was subjected to distillation by using simple
A. Materials distillation method. After that, a rotary vacuum evaporator
The aerial root collected from in and around was used to concentrate the extract [17].
Tiruchirappalli district, Tamilnadu. The collected aerial C. Preparation of Gel
roots were authenticated by Botanist, Dept. of Botany, Carbopol 940 and 974 were soaked in water for 24 hours
National College, Trichy. Carbopol, Triethanolamine and before being neutralized with triethanolamine to pH 6.8.
propylene glycol was a gift sample from Loba chemi, Prior to adding Carbopol, a weighed amount of methyl
Mumbai. Clove oil was purchased from MSM natural oil paraben and propyl paraben were added and thoroughly
and species, Kodaikanal.Streptococcus mutans- 25175 and mixed. To obtain a proper gel form, a measured amount of
Lactobacillus was purchased from MTCC, Chandihar, India. aerial root extract and clove oil were added to the prepared
Nutrient Agar medium, Nutrient broth, Gentamicin gel, followed by the required quantity of propylene glycol
antibiotic solution was purchased from Himedia, India. and stirred continuously [18]. To choose the best
B. Method of preparation of extract formulation, all of the prepared gels were subjected through
The aerial root of Ficus benghalensis was collected and an evaluation test.The various gel compositions were listed
subjected to shade dry.The material was grinded into a in the table 1.
S.NO Ingredients F1 F2 F3 F4 F5 F6
1 Extract of aerial root 2.5 g 2.5 g 2.5 g 2.5 g 2.5 g 2.5 g
2 Clove oil 0.3 ml 0.3 ml 0.3 ml 0.3 ml 0.3 ml 0.3 ml
3 Carbopol 940 0.4 g 0.6 g 0.8 g - - -
4 Carbopol 974 - - - 0.4 g 0.6 g 0.8 g
5 Propylene glycol 6 ml 6 ml 6 ml 6 ml 6 ml 6 ml
6 Methyl paraben 0.18 g 0.18 g 0.18 g 0.18 g 0.18 g 0.18 g
7 Propyl paraben 0.02 g 0.02 g 0.02 g 0.02 g 0.02 g 0.02 g
8 Triethanolamine q. s q. s q. s q. s q. s q. s
9 Distilled water q. s q. s q. s q. s q. s q. s
Table 1: Formulation of dental gel
III. EVALUATION G. Homogeneity
The gels were fixed in the container further they were
A. Physical appearance visually inspected for homogeneity and the presence of any
The physical appearance of the formulation was checked aggregate [19].
visually
H. Spread ability
B. Colour To determine the spread ability, 0.5g of gel formulation
The formulation’s colour was checked against a white placed between two horizontal smooth surface glass plates
background[19]. (20 cm x 20 cm), the spreading diameter was measured. The
initial diameter of the gel on the glass plate was measured in
C. Consistency centimetres. For 1 minute, another glass plate (weighing
The consistency was checked by applying on skin [19]. around 200 g) with the same dimensions was placed over the
D. Greasiness gel until no more expansion was detected. The upper plate
The greasiness was assisted by the application on to the was slowly removed, and the diameter of the circle formed
skin[19]. after the gel spreaded was measured in centimetres [20].
E. Odour I. Viscosity
The odour of the gels was evaluated by dissolving them The viscosities of the prepared gels were determined by
in water and smelling them[19]. using Brookfield viscometer spindle no 7 and spindle speed
60 rpm at 25◦ C. Viscosities were recorded at room
F. pH temperature [21].
2.5 grams of gel were precisely weighed and dispersed in
25 ml of distilled water. A digital pH meterwas used to J. Drug content
determine the pH of the dispersion [19]. To evaluate the drug content of the gel formulation, the
gel (10 mg) was dissolved in about 5-6 ml of phosphate
buffer (pH 6.8) and then sonicated for 15 minutes to obtain
IJISRT22MAY890 www.ijisrt.com 1067
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
complete solubility of the drug. The resulting solution was M. Release Kinetics
made up to 10 ml and filtered. The filtrate was then diluted The mechanism of drug release from the dental gel was
with phosphate buffer 10 times. The drug content was studied by fitting formulation diffusion data into model-
determined by spectro photometry [20]. dependent kinetics such as zero order, first order, Higuchi,
and Korsemeyer-Peppas equations.
K. Extrudability
The prepared gel was filled into a typical capped N. Ex-vivo study
collapsible aluminium tube and crimped closed at the end. Ex-vivo buccal permeation tests were performed on goat
The tubes' weights were calculated. After being sandwiched buccal skin. A 500ml beaker held 400ml of phosphate buffer
between two glass slides, the tubes were clamped. 500g of (pH 6.8) in the receptor compartment. The temperature was
weight was placed over the slides and then cap was kept at 37 ± 0.5°C and the solution was agitated at 900rpm.
removed. The amount of extruded gel was collected and The gel was placed in Goat buccal mucosal skin and it was
weighed. The percent of extruded gel was calculated [19]. tied to the one end of open-ended glass cylinder and then
dipped into freshly prepared phosphate buffer on magnetic
L. In-vitro diffusion study stirrer. Samples were taken from receptor medium at 0, 10,
1g of the formulation was placed in the donar 20, 30, 40, 50, 60 mins time interval. Periodically 5 ml of
compartment over an egg membrane that had been washed sample was withdrawn and same volume of fresh buffer was
and immersed in the diffusion medium for 24 hrs. The donar replaced in the medium.Using phosphate buffer 6.8 pH as a
compartment is dipped in the receptor compartment, which blank, all samples were spectrophotometrically analysed at
contains 400 ml of pH 6.8 phosphate buffer and the beaker 262nm.
holding diffusion medium (receptor compartment) is kept at
37◦ C with constant stirring at 22rpm using a magnetic O. Antimicrobial activity
stirrer. The study was carried out for 1 hour with 10 minutes Petri plates containing 20 ml nutrient agar media were
interval, 5 ml aliquots are removed from the diffusion injected with bacterial strains that had been cultured for 24
medium and replaced with same amount of new, pre hours (Streptococcus mutans and Lactobacillus).Wells were
warmed diffusion medium. The materials were tested cut and concentration of gel formulations were added. The
spectrophotometrically at 262 nm using a Shimadzu Double plates were then incubated for 24 hours at 37◦ C. The
beam UV-visible spectrophotometer [22]. diameter of the inhibition zone produced around the wells
was used to evaluate antibacterial activity [23,24].
IV. RESULTS
Formulations Appeara-nce pH Homogeneity Spreadability (g-cm/sec) Extruda-bility (%)
F1 Pale yellow 6.6±0.02 Good 18.32± 0.06 91.2± 0.21
F2 Pale yellow 6.8± 0.05 Very Good 16.25± 0.08 92.75± 0.31
F3 Pale yellow 6.7± 0.04 Good 15.78± 0.04 89.01± 0.52
F4 Pale yellow 6.7± 0.04 Good 18.68± 0.05 90.44± 0.45
F5 Pale yellow 6.8± 0.05 Very good 17.88± 0.09 93.13± 0.22
F6 Pale yellow 6.7± 0.03 Good 14.38± 0.05 88.5± 0.31
Table 2: Properties of dental gel
Formulations Viscosity (cps) Drug content (%) % Drug release
F1 8195± 45.12 91.3± 0.15 87.89± 0.55
F2 9450± 67.05 95.3± 0.12 93.10± 0.52
F3 9890± 68.09 93.4± 0.35 90.45± 0.25
F4 9286± 49.68 92.2± 0.13 92.05± 0.63
F5 9550± 55.12 95.5± 0.25 96.10± 0.07
F6 9800± 72.15 95.0± 0.41 94.89± 0.10
Table 3: Characterization of dental gel
IJISRT22MAY890 www.ijisrt.com 1068
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
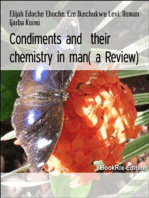
A. Diffusion study plot for formulations
In-vitro diffussion profile of formulations
120
Cumulative % drug release 100
80
60
40
20
0
0 10 20 30 40 50 60
Time (min)
F1 F2 F3 F4 F5 F6
Fig. 1: In-vitro diffusion profile of formulations
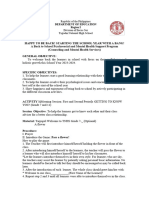
B. Antimicrobial activity
Antimicrobial activity gel formulations on Streptococcus mutans
Antimicrobial activity of gel formulations on Lactobacillus acidophilus
Fig. 2: Antimicrobial activity of formulations on organisms
Zone of inhibition of organisms
Formulation Zone of inhibition (S.mutans) Zone of inhibition (L.acidophilus)
F1 17.91± 0.05 15.23± 0.62
F2 21.6± 0.3 18.61± 0.3
F3 19.82± 0.4 17.62± 0.2
F4 18.52± 0.01 17.55± 0.1
F5 22.51± 0.1 20.42± 0.05
F6 20.02± 0.5 18.35± 0.1
Table 4: Zone of inhibition of organisms
IJISRT22MAY890 www.ijisrt.com 1069
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Zone of inhibiton (S.mutans)
25
Zone of inhibiton (mm)
20
15
10
0
F1 F2 F3 F4 F5 F6
Gel Formulations
Fig. 3: Zone of inhibition (Streptococcus mutans)
Zone of inhibition (L.acidophilus)
Zone of inhibition (mm)
25
20
15
10
0
F1 F2 F3 F4 F5 F6
Gel formulations
Fig. 4: Zone of inhibition (Lactobacillus acidophilus)
Comparison of Antimicrobial activity of the formulation F5 with marketed formulation
Antimicrobial activity on Streptococcus mutans
IJISRT22MAY890 www.ijisrt.com 1070
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Antimicrobial activity on Lactobacillus acidophilus
Fig. 5: Comparison of antimicrobial activity of F5 with marketed formulation
Microorganisms F5 Extract of aerial root Marketed
formulation
Streptococcus mutans 22.51± 0.1 23.32± 0.4 24.6± 1.1
Lactobacillus acidophilus 20.42± 0.05 21.01± 0.06 21.3± 0.2
Table 5: Comparison of Antimicrobial activity of F5 with marketed formulation
V. DISCUSSION The gel formulation of extract of aerial root of Ficus
benghalensis F5 shows good physicochemical properties as
The formulations were developed by using extract of well as good drug content compared to other formulations.
aerial root of Ficus benghalensisusing two grades of
Carbopol at varied concentrations. The formulation All the six formulations were subjected to
composition was shown in the Table 1. All the six batches of antimicrobial activity against Streptococcus mutans and
formulations were subjected to physicochemical evaluation. Lactobacillus acidophilus. From the report, it has shown that
The colour of all the formulations were pale yellow in formulation F5 has highest antimicrobial potential which is
colour. further compared with marketed formulation (Table No 4).
As shown in Table 2, the pH of all formulations ranged From the Table No 5, it was observed that optimized
from 6.6 to 6.8. This was considered to be closer to the pH formulation and marketed formulation produced almost
of the buccal cavity (6–7), suggesting that the gel equal zone of inhibition. Hence, optimized formulation F5
formulations will be irritation-free. has produced good antimicrobial effect.
The homogeneity of all formulations was shown in the VI. CONCLUSION
Table 2. All the formulations were homogeneous and free of
aggregates. The aerial root of Ficus benghalensis was found to
have antimicrobial activity against Streptococcus mutans
The Spreadability of prepared gels were found to be in and Lactobacillus acidophilus. The gel formulations
the range of 16.25 – 18.68 g-cm/sec, confirming that the gel developed from aerial root shows significant results so that
formulations were spread smoothly and uniformly. The tube it can be further used commercially to develop dental gels
extrudability of all formulations was good. after conducting theclinical trials on human beings.
However, more research is required to identify whether they
The drug content of gel formulations was ranged from can effectively replace synthetic antibiotics or be used in
91.3 to 95.5% Table 3. It indicates that there was no combination.
degradation of drug during the preparation process.
REFERENCES
The in-vitro drug release data for the formulation were
studied and shown in Table 3. The examination of the [1.] Laudenbach JM, Simon Z. Common dental and
regression coefficient value r2 forF5 indicated that the drug periodontal diseases: evaluation and management.
release followed diffusion mechanism. From release kinetic Medical Clinics. 2014 Nov 1;98(6):1239-60.
results, F5 was selected as the optimized [2.] World Health Organization. Oral health surveys: basic
formulationandKorsmeyer -Peppas model release exponent methods. World Health Organization; 2013.
‘n’ valuewas 1.106, thus it follows diffusion mechanism. [3.] Segura A, Boulter S, Clark M, Gereige R, Krol DM,
Among the six formulations F5 showed maximum drug Mouradian W, Quinonez R, Ramos-Gomez F, Slayton
release (96.10%). R, Keels MA. Maintaining and improving the oral
health of young children. Pediatrics. 2014 Dec
1;134(6):1224-9.
IJISRT22MAY890 www.ijisrt.com 1071
Volume 7, Issue 5, May – 2022 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
[4.] Segura A, Boulter S, Clark M, Gereige R, Krol DM, [19.] Shivhare UD, Jain KB, Mathur VB, Bhusari KP, Roy
Mouradian W, Quinonez R, Ramos-Gomez F, Slayton AA. Formulation development and evaluation of
R, Keels MA. Maintaining and improving the oral diclofenac sodium gel using water soluble
health of young children. Pediatrics. 2014 Dec polyacrylamide polymer. Digest journal of
1;134(6):1224-9. nanomaterials & biostructures (DJNB). 2009 Jun
[5.] Southam JC, Soames JV. Dental caries. Oral 1;4(2).
pathology. 1993;2. [20.] Helal DA, El-Rhman DA, Abdel-Halim SA, El-
[6.] Wong A, Young DA, Emmanouil DE, Wong LM, Nabarawi MA. Formulation and evaluation of
Waters AR, Booth MT. Raisins and oral health. Journal fluconazole topical gel. Int J Pharm Pharm Sci.
of food science. 2013 Jun;78(s1):A26-9. 2012;4(5):176-83.
[7.] Banerjee A, Pickard HM, Watson TF. Pickard's manual [21.] Aslani A, Ghannadi A, Najafi H. Design, formulation
of operative dentistry. Oxford university press; 2011 and evaluation of a mucoadhesive gel from Quercus
Jan 13. brantii L. and Coriandrum sativum L. as periodontal
[8.] Holloway PJ, Moore WJ. The role of sugar in the drug delivery. Advanced biomedical research. 2013;2.
aetiology of dental caries: 1. sugar and the antiquity of [22.] Bisht N, Goswami L, Kothiyal P. Preparation and
dental caries. Journal of dentistry. 1983 Sep evaluation of in-situ oral topical gel of levofloxacin by
1;11(3):189-90. using combination of polymers. Indian J Drugs.
[9.] Peres M, Heilmann A. Social inequalities in oral 2014;2(4):142-51.
health: from evidence to action. London: International [23.] Bauer AW, Roberts Jr CE, Kirby W. Single disc versus
Centre for Oral Health Inequalities Research & Policy. multiple disc and plate dilution techniques for
2015. antibiotic sensitivity testing. Antibiotics annual.
[10.] Marsh PD. Dental plaque as a biofilm and a microbial 1959;7:574-80.
community–implications for health and disease. [24.] Bauer AW, PERRY DM, KIRBY WM. Single-disk
InBMC Oral health 2006 Jun (Vol. 6, No. 1, pp. 1-7). antibiotic-sensitivity testing of staphylococci: An
BioMed Central. analysis of technique and results. AMA archives of
[11.] Marsh PD. Dental plaque as a biofilm and a microbial internal medicine. 1959 Aug 1;104(2):208-16.
community–implications for health and disease.
InBMC Oral health 2006 Jun (Vol. 6, No. 1, pp. 1-7).
BioMed Central.
[12.] Alshahrani I, Tikare S, Meer Z, Mustafa A,
Abdulwahab M, Sadatullah S. Prevalence of dental
caries among male students aged 15–17 years in
southern Asir, Saudi Arabia.The Saudi dental journal.
2018 Jul 1;30(3):214-8.
[13.] Mwesiga EK, Kaddumukasa M, Mugenyi L, Nakasujja
N. Classification and description of chronic pain
among HIV positive patients in Uganda. African
Health Sciences. 2019 Aug 20;19(2):1978-87.
[14.] Clementino MA, Gomes MC, Pinto-Sarmento TC,
Martins CC, Granville-Garcia AF, Paiva SM.
Perceived impact of dental pain on the quality of life of
preschool children and their families. PloS one. 2015
Jun 19;10(6):e0130602.
[15.] Ananthathavam K, Ramamurthy J. Treating
periodontitis with the use of essential oil and herbs.
Journal of Pharmacy and Pharmacology. 2014;4(1):39-
42.
[16.] Gupta NI, Patel AR, Ravindra RP. Design of akkalkara
(Spilanthesacmella) formulations for anti-microbial
and topical anti-inflammatory activities. International
Journal of Pharma and Bio Sciences. 2012;3(4):161-
70.
[17.] Talukdar SN, Rahman MB, Paul S. Screening of
Pharmacognostical, Phytochemical Profile and
Traditional Application of Ficus benghalensis. British
Journal of Pharmaceutical Research. 2015 Jan 1;8(3).
[18.] Pawar VA, Bhagat TB, Toshniwal MR, Mokashi ND,
Khandelwal KR. Formulation and evaluation of dental
gel containing essential oil of coriander against oral
pathogens. Int Res J Pharm. 2013;4(10):48-54.
IJISRT22MAY890 www.ijisrt.com 1072
You might also like
- 6422d2941ce0e5 46368121Document21 pages6422d2941ce0e5 46368121vijaynkl944434No ratings yet
- Downloadfile PDFDocument12 pagesDownloadfile PDFFrengkyNo ratings yet
- Olives and Olive Oil as Functional Foods: Bioactivity, Chemistry and ProcessingFrom EverandOlives and Olive Oil as Functional Foods: Bioactivity, Chemistry and ProcessingApostolos KiritsakisNo ratings yet
- Keywords:-Red Betel Leaf Extract, Mint Leaf ExtractDocument7 pagesKeywords:-Red Betel Leaf Extract, Mint Leaf ExtractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Aloe Vera Dental Gel Containing Clove Oil and Peppermint OilDocument5 pagesFormulation and Evaluation of Aloe Vera Dental Gel Containing Clove Oil and Peppermint OilInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- IntJPharmChemAnal 9 1 17 21Document5 pagesIntJPharmChemAnal 9 1 17 21windfragNo ratings yet
- (Ocimum Basilicum L.) Memiliki Aktivitas Antibakteri Yang Baik. Penelitian Ini BertujuanDocument9 pages(Ocimum Basilicum L.) Memiliki Aktivitas Antibakteri Yang Baik. Penelitian Ini BertujuanRaden LazuardiNo ratings yet
- Formulasi Pasta Gigi Gel Ekstrak Etanol Bawang Dayak (Eleutherine Bulbosa (Mill.) Urb.)Document8 pagesFormulasi Pasta Gigi Gel Ekstrak Etanol Bawang Dayak (Eleutherine Bulbosa (Mill.) Urb.)indah lestariNo ratings yet
- Evaluation of ToothpasteDocument8 pagesEvaluation of ToothpasteBINDUNo ratings yet
- Materi If OtDocument7 pagesMateri If OtNining FauziahNo ratings yet
- AsianJBiolLifeSci 12 1 172Document7 pagesAsianJBiolLifeSci 12 1 172Mahima SrivastavaNo ratings yet
- Formulasi Pasta Gigi Natrium BicarbonatDocument4 pagesFormulasi Pasta Gigi Natrium BicarbonatCut RifqaNo ratings yet
- Clinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmDocument7 pagesClinical Study Baccharis Dracunculifolia As Agent For The Control of BiofilmimamaptNo ratings yet
- Antimicrobial Efficacy of Commercially Available Toothpastes - An in Vitro StudyDocument7 pagesAntimicrobial Efficacy of Commercially Available Toothpastes - An in Vitro StudybiswasblrNo ratings yet
- Article 5Document9 pagesArticle 5techno gamersNo ratings yet
- Herbal Mouthwash A Compressive Study The ReviewDocument8 pagesHerbal Mouthwash A Compressive Study The ReviewMahima SrivastavaNo ratings yet
- Dragon Fruit PDFDocument4 pagesDragon Fruit PDFrikaNo ratings yet
- Mini Review SOJ Dental and Oral Disorder Natural Products in Oral Care, Why Use ThemDocument4 pagesMini Review SOJ Dental and Oral Disorder Natural Products in Oral Care, Why Use ThemNealNo ratings yet
- Characteristics of An Alternative Antibacterial Biomaterial For Mouthwash in The Absence of AlcoholDocument6 pagesCharacteristics of An Alternative Antibacterial Biomaterial For Mouthwash in The Absence of Alcoholsaila salsabilaNo ratings yet
- Jdod v2 Id1046Document7 pagesJdod v2 Id1046desti suci wulandariNo ratings yet
- IJNRD2305787Document15 pagesIJNRD2305787Mahima SrivastavaNo ratings yet
- The Use of Phytotherapy in Dentistry: Review StudyDocument10 pagesThe Use of Phytotherapy in Dentistry: Review StudyCristiane ccmNo ratings yet
- Mutiara Annisa, Bay Leaves, Toothpaste, Stain RemovelDocument11 pagesMutiara Annisa, Bay Leaves, Toothpaste, Stain RemovellydiasusantiNo ratings yet
- Review Literature On Toothpaste: AbstractDocument5 pagesReview Literature On Toothpaste: Abstractpiyush jainNo ratings yet
- Formulasi Dan Uji Aktivitas Antibakteri Streptococcus Mutans Dari Sediaan Mouthwash Ekstrak Daun Jambu Biji (Psidium Guajava L.)Document13 pagesFormulasi Dan Uji Aktivitas Antibakteri Streptococcus Mutans Dari Sediaan Mouthwash Ekstrak Daun Jambu Biji (Psidium Guajava L.)Hafifah Binti DjaeseNo ratings yet
- Amadi PresentationDocument14 pagesAmadi Presentationgelisar3sNo ratings yet
- Formulation and Evaluation of Herbal ToothpasteDocument8 pagesFormulation and Evaluation of Herbal ToothpasteIJRASETPublicationsNo ratings yet
- Formulation and Evaluation of Herbal Tooth Gel ContainingDocument6 pagesFormulation and Evaluation of Herbal Tooth Gel ContainingJohanna MonroyNo ratings yet
- An Invitro Study of Determination of Anti-Bacterial, Antioxidant, Anti-Inflammatory Potential of Piper Betel Essential OilDocument8 pagesAn Invitro Study of Determination of Anti-Bacterial, Antioxidant, Anti-Inflammatory Potential of Piper Betel Essential OilSaiful AbdulNo ratings yet
- EGG SHELL (Calcium Carbonate) and BAKING SODA (Sodium Bicarbonate)Document8 pagesEGG SHELL (Calcium Carbonate) and BAKING SODA (Sodium Bicarbonate)dinnes masubay100% (3)
- Design and Development of Tooth Paste Containing Alcoholic Extract of Psidium Guajava LeafDocument8 pagesDesign and Development of Tooth Paste Containing Alcoholic Extract of Psidium Guajava LeafMahewash PathanNo ratings yet
- Citrus JurnalDocument10 pagesCitrus Jurnalasti findaNo ratings yet
- (Ocimum Basilicum L.) Memiliki Aktivitas Antibakteri Yang Baik. Penelitian Ini BertujuanDocument9 pages(Ocimum Basilicum L.) Memiliki Aktivitas Antibakteri Yang Baik. Penelitian Ini BertujuanUlfa Kaka' TersaiiankNo ratings yet
- Ginger 3Document11 pagesGinger 3ian605No ratings yet
- Inhibitory Effects of Plant Extracts On Multi-Species Dental Biofilm Formation In-VitroDocument9 pagesInhibitory Effects of Plant Extracts On Multi-Species Dental Biofilm Formation In-VitroahmicphdNo ratings yet
- Review - MouthwashDocument6 pagesReview - MouthwashShriya SingiNo ratings yet
- MM - Ejgd 360 BlindDocument32 pagesMM - Ejgd 360 BlindMuhammad IhsanNo ratings yet
- Formulation and Evaluation of Tooth Gel From Aloe Vera Leaves ExtractDocument6 pagesFormulation and Evaluation of Tooth Gel From Aloe Vera Leaves Extractshafira putri pertiwiNo ratings yet
- Antibacterial Herbal Mouthwash Formulation and Evaluation Against Oral DisordersDocument10 pagesAntibacterial Herbal Mouthwash Formulation and Evaluation Against Oral DisordersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 4138 10812 1 PBDocument7 pages4138 10812 1 PBPsht RudiNo ratings yet
- Formulation and Development of Dental Gel Containing Clove Oil The Treatment Periodontal DiseasesDocument28 pagesFormulation and Development of Dental Gel Containing Clove Oil The Treatment Periodontal DiseasesVinayKumarNo ratings yet
- Fmicb 13 999839Document24 pagesFmicb 13 999839Miyyada AichaouiNo ratings yet
- IJCRT2202359Document10 pagesIJCRT2202359Jhaira Mae Heriz M. BuñoNo ratings yet
- Herbs in Dentistry: DR - Lahari BuggapatiDocument6 pagesHerbs in Dentistry: DR - Lahari BuggapatiDrDeepak PrasharNo ratings yet
- J Pak Dent Assoc 2011 20 3 163 170Document8 pagesJ Pak Dent Assoc 2011 20 3 163 170haseosamaNo ratings yet
- CT FinalsDocument8 pagesCT Finalsnoelah salcedoNo ratings yet
- Potential of Lauric Acid, Miristic Acid and Combination Gel As Inhibiting The Growth of Porphyromonas Gingivalis Bacteria in GingivitisDocument9 pagesPotential of Lauric Acid, Miristic Acid and Combination Gel As Inhibiting The Growth of Porphyromonas Gingivalis Bacteria in GingivitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effectiveness of Belimbing Wuluh (Averrhoa Blimbi L) Acid Extract As Mouthwash As An Alternative To Relieve GingivitisDocument6 pagesThe Effectiveness of Belimbing Wuluh (Averrhoa Blimbi L) Acid Extract As Mouthwash As An Alternative To Relieve GingivitisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- JPTCP - 943 29 E094Document10 pagesJPTCP - 943 29 E094Mahima SrivastavaNo ratings yet
- Naskah Bu Fith 03Document13 pagesNaskah Bu Fith 03Chitra Septinia AshidiqiNo ratings yet
- Jikki 172-185Document14 pagesJikki 172-185raihanul khairiNo ratings yet
- Wood 47 2 178Document11 pagesWood 47 2 178Dayanna CuevasNo ratings yet
- 11-Fitri Handayani PDFDocument11 pages11-Fitri Handayani PDFMarry Chen haoNo ratings yet
- 1011-Article Text-2835-1-10-20141115Document7 pages1011-Article Text-2835-1-10-20141115kattveneNo ratings yet
- Science Investigatory Project - FinalDocument10 pagesScience Investigatory Project - FinalErich Benedict ClerigoNo ratings yet
- Lamo ProjectDocument12 pagesLamo ProjectlameckomondiochiengNo ratings yet
- Publication 16Document7 pagesPublication 16Valentina CarreroNo ratings yet
- Metode Gradient AntimikrobaDocument18 pagesMetode Gradient AntimikrobaFatmawati NadhyaNo ratings yet
- Cyber Security Awareness and Educational Outcomes of Grade 4 LearnersDocument33 pagesCyber Security Awareness and Educational Outcomes of Grade 4 LearnersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Factors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaDocument6 pagesFactors Influencing The Use of Improved Maize Seed and Participation in The Seed Demonstration Program by Smallholder Farmers in Kwali Area Council Abuja, NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueDocument2 pagesParastomal Hernia: A Case Report, Repaired by Modified Laparascopic Sugarbaker TechniqueInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Health Care SystemDocument8 pagesSmart Health Care SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Blockchain Based Decentralized ApplicationDocument7 pagesBlockchain Based Decentralized ApplicationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Unmasking Phishing Threats Through Cutting-Edge Machine LearningDocument8 pagesUnmasking Phishing Threats Through Cutting-Edge Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Study Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoDocument6 pagesStudy Assessing Viability of Installing 20kw Solar Power For The Electrical & Electronic Engineering Department Rufus Giwa Polytechnic OwoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Industry That Capitalizes Off of Women's Insecurities?Document8 pagesAn Industry That Capitalizes Off of Women's Insecurities?International Journal of Innovative Science and Research TechnologyNo ratings yet
- Visual Water: An Integration of App and Web To Understand Chemical ElementsDocument5 pagesVisual Water: An Integration of App and Web To Understand Chemical ElementsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Insights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesDocument8 pagesInsights Into Nipah Virus: A Review of Epidemiology, Pathogenesis, and Therapeutic AdvancesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Smart Cities: Boosting Economic Growth Through Innovation and EfficiencyDocument19 pagesSmart Cities: Boosting Economic Growth Through Innovation and EfficiencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Parkinson's Detection Using Voice Features and Spiral DrawingsDocument5 pagesParkinson's Detection Using Voice Features and Spiral DrawingsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Impact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldDocument6 pagesImpact of Silver Nanoparticles Infused in Blood in A Stenosed Artery Under The Effect of Magnetic Field Imp. of Silver Nano. Inf. in Blood in A Sten. Art. Under The Eff. of Mag. FieldInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Compact and Wearable Ventilator System For Enhanced Patient CareDocument4 pagesCompact and Wearable Ventilator System For Enhanced Patient CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Air Quality Index Prediction Using Bi-LSTMDocument8 pagesAir Quality Index Prediction Using Bi-LSTMInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Predict The Heart Attack Possibilities Using Machine LearningDocument2 pagesPredict The Heart Attack Possibilities Using Machine LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolDocument31 pagesThe Relationship Between Teacher Reflective Practice and Students Engagement in The Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis On Mental Health Issues Among IndividualsDocument6 pagesAn Analysis On Mental Health Issues Among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Implications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewDocument6 pagesImplications of Adnexal Invasions in Primary Extramammary Paget's Disease: A Systematic ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation For Translating Global Languages Into Indian LanuagesDocument7 pagesHarnessing Open Innovation For Translating Global Languages Into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Keywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalDocument7 pagesKeywords:-Ibadhy Chooranam, Cataract, Kann Kasam,: Siddha Medicine, Kann NoigalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix Dactylifera) Leaf Fiber As A Main Component in Making An Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions On Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions On Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning For Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses For The Visually Impaired Using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonDocument14 pagesTerracing As An Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains - CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Anti-Aging Checklist - Cheat SheetDocument5 pagesAnti-Aging Checklist - Cheat SheetdrissNo ratings yet
- 4.iJGP - Case ReportDocument4 pages4.iJGP - Case Reportpalak GandhiNo ratings yet
- Method of Statement For GroutingDocument7 pagesMethod of Statement For GroutingCezar DasiNo ratings yet
- Full Download Test Bank For Health Psychology 3rd Edition Sanderson PDF Full ChapterDocument13 pagesFull Download Test Bank For Health Psychology 3rd Edition Sanderson PDF Full Chapterrequinneologic8yzqgt100% (17)
- Tanishqa Jogani - TAPMIDocument3 pagesTanishqa Jogani - TAPMITanishqa JoganiNo ratings yet
- Male Female PsychologyDocument38 pagesMale Female PsychologyParamjit SharmaNo ratings yet
- March/April 2002 Number 2 105-208 ©: Operative Dentistry, IncDocument108 pagesMarch/April 2002 Number 2 105-208 ©: Operative Dentistry, IncZulvan AviviNo ratings yet
- Silo - Tips - Standard Test Methods For Rubber Deterioration Cracking in An Ozone Controlled Environment 1Document11 pagesSilo - Tips - Standard Test Methods For Rubber Deterioration Cracking in An Ozone Controlled Environment 1Chanin NgudsuntearNo ratings yet
- Vineland Adaptive Behaviour Scales (VABS) - IIDocument6 pagesVineland Adaptive Behaviour Scales (VABS) - IIAlan Marsh67% (3)
- Medical Student Assessment Form in PDFDocument4 pagesMedical Student Assessment Form in PDFDanial S. SaktiNo ratings yet
- REBAMIPIDEDocument2 pagesREBAMIPIDEMary Grace AgataNo ratings yet
- Mhcet Mock Test-2Document29 pagesMhcet Mock Test-2Poonam UpadhyayNo ratings yet
- Memorix Anatomy 2Document1 pageMemorix Anatomy 2Sreedhar Tirunagari100% (1)
- A Differential Diagnosis For Any Condition The Universal DDX MnemonicDocument1 pageA Differential Diagnosis For Any Condition The Universal DDX MnemonicabdulghaniNo ratings yet
- FKG Catalogue 2015Document68 pagesFKG Catalogue 2015Septimiu TiplicaNo ratings yet
- Hopes For Speedy Rebound Dim: For Personal, Non-Commercial Use OnlyDocument32 pagesHopes For Speedy Rebound Dim: For Personal, Non-Commercial Use OnlyMiguel DiazNo ratings yet
- Lilac Illustrated Social Psychology PresentationDocument35 pagesLilac Illustrated Social Psychology PresentationGia GajasNo ratings yet
- Scholarship ApplicationDocument5 pagesScholarship ApplicationANDREASNo ratings yet
- Sop of Disinfection, CoatingDocument27 pagesSop of Disinfection, CoatingAhmed Quadri0% (1)
- Advocacy On Related Laws - 2019Document37 pagesAdvocacy On Related Laws - 2019Aileen Labastida BarcenasNo ratings yet
- Ingles 2Document21 pagesIngles 2Flor TrujilloNo ratings yet
- EFT Self Reflections Cycle Questions WorksheetDocument2 pagesEFT Self Reflections Cycle Questions WorksheetL.I. CubeNo ratings yet
- PsychosocialSupport2023 2024Document5 pagesPsychosocialSupport2023 2024Jasmin LicudineNo ratings yet
- Multidimensional PovertyDocument2 pagesMultidimensional PovertyJohn ClarenceNo ratings yet
- Red Cross CPR Guidelines PDFDocument31 pagesRed Cross CPR Guidelines PDFandrewh3No ratings yet
- NHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalDocument3 pagesNHS Dental Statistics For England 2018-19, Annual Report (PAS) - NHS DigitalRowayda NourNo ratings yet
- Sample Disaster Emergency Preparedness ManualDocument32 pagesSample Disaster Emergency Preparedness ManualAnn PerezNo ratings yet
- 5 INGREDIENTS - EbookDocument14 pages5 INGREDIENTS - EbookHeuler KretliNo ratings yet
- The Radiology Specialty Is Constantly ChangingDocument3 pagesThe Radiology Specialty Is Constantly ChangingLiora SochenNo ratings yet
- GP - Topik ACS Dr. Achmad PutraDocument64 pagesGP - Topik ACS Dr. Achmad Putrapuroxaair001No ratings yet
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (3)
- Meltdown: Nuclear disaster and the human cost of going criticalFrom EverandMeltdown: Nuclear disaster and the human cost of going criticalRating: 5 out of 5 stars5/5 (5)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableFrom EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableRating: 3.5 out of 5 stars3.5/5 (22)
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsFrom EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsRating: 4 out of 5 stars4/5 (146)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction, and the Science of Everyday LifeRating: 4 out of 5 stars4/5 (1)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- Handbook of Formulating Dermal Applications: A Definitive Practical GuideFrom EverandHandbook of Formulating Dermal Applications: A Definitive Practical GuideNo ratings yet
- Formulating, Packaging, and Marketing of Natural Cosmetic ProductsFrom EverandFormulating, Packaging, and Marketing of Natural Cosmetic ProductsNo ratings yet
- Science Goes Viral: Captivating Accounts of Science in Everyday LifeFrom EverandScience Goes Viral: Captivating Accounts of Science in Everyday LifeRating: 5 out of 5 stars5/5 (1)
- Bioplastics: A Home Inventors HandbookFrom EverandBioplastics: A Home Inventors HandbookRating: 4 out of 5 stars4/5 (2)
- Phase Equilibria in Chemical EngineeringFrom EverandPhase Equilibria in Chemical EngineeringRating: 4 out of 5 stars4/5 (11)
- AP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeFrom EverandAP® Chemistry Crash Course, For the 2020 Exam, Book + Online: Get a Higher Score in Less TimeRating: 5 out of 5 stars5/5 (1)
- A Perfect Red: Empire, Espionage, and the Quest for the Color of DesireFrom EverandA Perfect Red: Empire, Espionage, and the Quest for the Color of DesireRating: 4 out of 5 stars4/5 (129)
- Transformer: The Deep Chemistry of Life and DeathFrom EverandTransformer: The Deep Chemistry of Life and DeathRating: 4.5 out of 5 stars4.5/5 (13)