You might also like
- Firearm InjuriesDocument90 pagesFirearm InjuriesARIF-UR-REHMAN100% (7)
- Gunshot Wound AnalysisDocument62 pagesGunshot Wound AnalysisEfraim Tad-oNo ratings yet
- Legal MEdicineDocument29 pagesLegal MEdicineMuktar CabangcalaNo ratings yet
- Forensic BallisticsDocument56 pagesForensic BallisticsSherwin Anoba Cabutija86% (7)
- Forensic Ballistics NotesDocument35 pagesForensic Ballistics NotesKylaNo ratings yet
- Firearm Injury MechanismsDocument65 pagesFirearm Injury MechanismsOmnms Btcs67% (9)
- Forensic BallisticsDocument162 pagesForensic BallisticsDanJairusBorreros100% (1)
- Lesson 4. Branches of BallisticsDocument40 pagesLesson 4. Branches of BallisticsメサErickエリックNo ratings yet
- Firearm and Explosive InjuriesDocument6 pagesFirearm and Explosive InjuriesRahma Tya AnwarNo ratings yet
- Ballistics - PPT LECDocument61 pagesBallistics - PPT LECHarrison sajor100% (1)
- Gunshot and ShrapnelsDocument23 pagesGunshot and ShrapnelsYuendri IrawantoNo ratings yet
- Work Summary - Fire Fighting Department - 20 JULY 2023Document48 pagesWork Summary - Fire Fighting Department - 20 JULY 2023ahmed abdi100% (1)
- Caliber Pistol Parts and FunctionsDocument3 pagesCaliber Pistol Parts and FunctionsDean Mark Anacio80% (5)
- Crime Unit 2Document29 pagesCrime Unit 2Dimitri TaffinNo ratings yet
- Introduction to Forensic BallisticsDocument8 pagesIntroduction to Forensic BallisticssharlynfaithloquireNo ratings yet
- Ballistics AssignmentDocument17 pagesBallistics AssignmentPreetiNo ratings yet
- Forensic MedicineDocument5 pagesForensic MedicineAlyanna ChangNo ratings yet
- Firearm Injuries: FirearmsDocument8 pagesFirearm Injuries: FirearmsDipu KumarNo ratings yet
- GUNSHOT FATALITY CAUSESDocument8 pagesGUNSHOT FATALITY CAUSESPoh TseNo ratings yet
- 7 - Ballistic WoundDocument62 pages7 - Ballistic WoundWala AbdeljawadNo ratings yet
- Forensic Ballistics IntroductionDocument5 pagesForensic Ballistics Introductionisaiah bungalsoNo ratings yet
- FBALLI ReviewwerrrrrDocument14 pagesFBALLI Reviewwerrrrrisaiah bungalsoNo ratings yet
- Forensic Med Lecture 7 (Chapter 7 Firearm & Explosion)Document24 pagesForensic Med Lecture 7 (Chapter 7 Firearm & Explosion)MowlidAbdirahman Ali madaaleNo ratings yet
- Firearm Weapon Is An Instrument Which Discharges A Missile by TheDocument32 pagesFirearm Weapon Is An Instrument Which Discharges A Missile by TheMds UniNo ratings yet
- Firearm Injuries578 PDFDocument26 pagesFirearm Injuries578 PDFRio LorraineNo ratings yet
- Ballistics ReaderDocument8 pagesBallistics ReaderDana Althea AlgabreNo ratings yet
- Vienna Convention On Diplomatic RelationsDocument21 pagesVienna Convention On Diplomatic Relationsnikkibeverly73No ratings yet
- Practical Firearm Injuries and SpecimensDocument59 pagesPractical Firearm Injuries and SpecimensmariamNo ratings yet
- Wounds by Shotguns: by Dilnaaz Baig Roll No-8 Batch 2015 Ii MbbsDocument13 pagesWounds by Shotguns: by Dilnaaz Baig Roll No-8 Batch 2015 Ii Mbbsniraj_sdNo ratings yet
- Wound Ballistics: Wounding MechanismDocument6 pagesWound Ballistics: Wounding MechanismAnuNo ratings yet
- 22 - Firearm Injuries Part1Document19 pages22 - Firearm Injuries Part1zaheeerkhanNo ratings yet
- Gunshot WoundsDocument32 pagesGunshot WoundsFersal Alberca0% (1)
- Jarak TembakDocument3 pagesJarak Tembakanon_167078713No ratings yet
- For6 MidtermDocument103 pagesFor6 MidtermChristianJohn NunagNo ratings yet
- Firearm Forensics GuideDocument4 pagesFirearm Forensics GuideJordine UmayamNo ratings yet
- Firearm Injuries: Forensic MedicineDocument71 pagesFirearm Injuries: Forensic MedicineHamzaNo ratings yet
- FORENSIC BALLISTICSDocument77 pagesFORENSIC BALLISTICSKhael BurerosNo ratings yet
- Entrance WoundsDocument14 pagesEntrance WoundsAmy BCNo ratings yet
- Bullet Exsanguination Strangulation Myocardial InfarctionDocument5 pagesBullet Exsanguination Strangulation Myocardial InfarctionGenevieve TersolNo ratings yet
- UNIT VI. Gunpowder and ExplosivesDocument6 pagesUNIT VI. Gunpowder and ExplosivesMariz Althea Jem BrionesNo ratings yet
- Chapter IDocument26 pagesChapter IEy GrailNo ratings yet
- Fsci CH 17Document22 pagesFsci CH 17api-266860509No ratings yet
- Sci1-Cdi-Ppt-11 (Nov 8-12)Document30 pagesSci1-Cdi-Ppt-11 (Nov 8-12)Wilson SarmientoNo ratings yet
- Firearm Injury EstimationDocument24 pagesFirearm Injury EstimationShaban YasserNo ratings yet
- FCT Dry Lab 5Document4 pagesFCT Dry Lab 5warlaxx ng MUndoNo ratings yet
- Forensic BallisticDocument12 pagesForensic BallisticYash GuptaNo ratings yet
- Firearm Injuries - Rifled Weapons and Wounds: Rami NunuDocument16 pagesFirearm Injuries - Rifled Weapons and Wounds: Rami NunudoodiboodiNo ratings yet
- Wound BallisticsDocument47 pagesWound BallisticsSarah RepinNo ratings yet
- Gunshot Wounds On Clothing - Arma de FogoDocument5 pagesGunshot Wounds On Clothing - Arma de FogomahatmaportoNo ratings yet
- Forensic 103Document6 pagesForensic 103Francheska Kate LabiosNo ratings yet
- Forensic BallisticsDocument169 pagesForensic BallisticsCounter IntelligenceNo ratings yet
- Gunpowder & ExplosivesDocument5 pagesGunpowder & ExplosivesNora BuanNo ratings yet
- Gunshot & Shrapnel WoundsDocument11 pagesGunshot & Shrapnel WoundsAda Gay Olandia Serencio100% (1)
- Ballistics NotesDocument86 pagesBallistics NotesBharyn SildonNo ratings yet
- 284481465 Legal Medicine Gunshot WoundDocument26 pages284481465 Legal Medicine Gunshot WoundLanceNo ratings yet
- Forensic BallisticsDocument96 pagesForensic Ballisticsduladanica15No ratings yet
- Presenter: Dr. Siyum (Omfsr-Ii) Moderator: Dr. Tsegaye (Omfs, Consultant)Document75 pagesPresenter: Dr. Siyum (Omfsr-Ii) Moderator: Dr. Tsegaye (Omfs, Consultant)Siyum MathewosNo ratings yet
- Tugas Forensik - Sholeha Khuldy C014212155Document5 pagesTugas Forensik - Sholeha Khuldy C014212155Sholeha KhuldyNo ratings yet
- Assignment GSWDocument1 pageAssignment GSWBenjamin BayugaNo ratings yet
- Lesson 5 Mechanical Injury Part2 (SHARP Vs Bluntfirearm) (Copy) )Document48 pagesLesson 5 Mechanical Injury Part2 (SHARP Vs Bluntfirearm) (Copy) )mirabel IvanaliNo ratings yet
- Forensics BallisticssDocument36 pagesForensics BallisticssJessica De la CruzNo ratings yet
- MedicoDocument3 pagesMedicoATOLBA, Rizel D.No ratings yet
- Blaser Jagdwaffen GMBH D-88316 Isny GermanyDocument9 pagesBlaser Jagdwaffen GMBH D-88316 Isny GermanyJustinNo ratings yet
- 76mm Shipboard BrochureDocument2 pages76mm Shipboard BrochureCarakaNo ratings yet
- VISIO - Fire Alarm - 201207130855008633Document1 pageVISIO - Fire Alarm - 201207130855008633Savy PhanethNo ratings yet
- Disaster Readiness Module 1Document15 pagesDisaster Readiness Module 1Marvin MelisNo ratings yet
- People VS GensolaDocument3 pagesPeople VS GensolaLeonardo LawasNo ratings yet
- Annual Poster-Making Contest Entitled Apoy, Bagyo, Kalamidad: Dibuhong Pambata (ABKD)Document1 pageAnnual Poster-Making Contest Entitled Apoy, Bagyo, Kalamidad: Dibuhong Pambata (ABKD)Jocelyn Cortes IntanoNo ratings yet
- GO KKP English: DisasterDocument1 pageGO KKP English: DisasterPaRaDoX eLaKSaMaNaNo ratings yet
- 48 Fire Training CertificateDocument4 pages48 Fire Training CertificateHiyam GandhiNo ratings yet
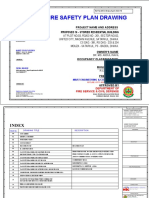
- Proposed Fire Safety Plan for 16-Storey Residential BuildingDocument18 pagesProposed Fire Safety Plan for 16-Storey Residential BuildingSofiqNo ratings yet
- GE8071-Disaster Management - by WWW - LearnEngineering.inDocument11 pagesGE8071-Disaster Management - by WWW - LearnEngineering.inDee pakNo ratings yet
- SEPSISDocument19 pagesSEPSISMUBIRU SAMUEL EDWARDNo ratings yet
- Risk Assessment Plan Sample TemplateDocument6 pagesRisk Assessment Plan Sample TemplateAbdulraheem SalmanNo ratings yet
- Report On Conduct of 2017 Fire Prevention Month MARCH 17-31, 2017Document2 pagesReport On Conduct of 2017 Fire Prevention Month MARCH 17-31, 2017LEAND ANTHONY CATAHUMBERNo ratings yet
- EX AT: Equipment CategoriesDocument2 pagesEX AT: Equipment CategoriesAminNo ratings yet
- MT Vesuvius EruptionDocument2 pagesMT Vesuvius Eruptionapi-614921940No ratings yet
- Class 4 - Modes of Liability - Sept 28Document29 pagesClass 4 - Modes of Liability - Sept 28Dora LopezNo ratings yet
- TONKSversion1 PlaintextDocument11 pagesTONKSversion1 PlaintextMartín FierroNo ratings yet
- Sako S20Document32 pagesSako S20OneMAN TwoWHEELSNo ratings yet
- WaW85 Clarifications and Corrections v1-2 Rev25 B&WDocument16 pagesWaW85 Clarifications and Corrections v1-2 Rev25 B&Wt1029No ratings yet
- Starsector - How To FightersDocument1 pageStarsector - How To FightersJefferson Rodrigo Fernandes PereiraNo ratings yet
- CSG FeoDocument36 pagesCSG FeoCarmelina Lao-ingNo ratings yet
- Strategic Goods Control Act - List HS Concordance (16 Apr 2008)Document519 pagesStrategic Goods Control Act - List HS Concordance (16 Apr 2008)Jason Quek100% (3)
- Bar GraphDocument8 pagesBar GraphAndreana EvansNo ratings yet
- CrimlawqnaDocument4 pagesCrimlawqnaJustine MontañezNo ratings yet
- NAA ItemNumber401505Document12 pagesNAA ItemNumber401505Jonathan ArmstrongNo ratings yet
- Weapons Tests and Evaluations The Best of Soldier of Fortune by Peter Kokalis - Gun Reviews Backed Up by Real TestingDocument2 pagesWeapons Tests and Evaluations The Best of Soldier of Fortune by Peter Kokalis - Gun Reviews Backed Up by Real Testinggot2bme43No ratings yet
- FFG Star Wars RPG EquipmentDocument44 pagesFFG Star Wars RPG EquipmentguiloNo ratings yet