You might also like
- Intro To The Philosophy of The Human Person - CH 3-1 One's Limitations and Possibilities For TranscendenceDocument39 pagesIntro To The Philosophy of The Human Person - CH 3-1 One's Limitations and Possibilities For TranscendenceEdgar Banquel100% (6)
- Social Psychology Chapter 18 NotesDocument8 pagesSocial Psychology Chapter 18 Notessarah44smith50% (2)
- Student Workbook Week #2Document9 pagesStudent Workbook Week #2Teja Babia-YoungNo ratings yet
- MS HS Safety PlanDocument4 pagesMS HS Safety PlanmorNo ratings yet
- Depression ScreeningToolDocument3 pagesDepression ScreeningToolBrasa Y. de AlmiraNo ratings yet
- MSPSSDocument3 pagesMSPSSTanvi ManjrekarNo ratings yet
- Mental Health: Health 7 Third Grading PeriodDocument50 pagesMental Health: Health 7 Third Grading Periodjdatu19100% (1)
- GABISAN - IBT-Student-Survey-QuestionnaireDocument2 pagesGABISAN - IBT-Student-Survey-QuestionnaireAkisa GabisanNo ratings yet
- Managing Stress: Coping in A Fast-Paced WorldDocument17 pagesManaging Stress: Coping in A Fast-Paced WorldhatanoloveNo ratings yet
- Counselling SkillsDocument40 pagesCounselling SkillsPrabhnoorNo ratings yet
- Difficult ConversationsDocument22 pagesDifficult ConversationsShraä Chäudhäri PätilNo ratings yet
- Per Dev Pointers To Review 1stDocument5 pagesPer Dev Pointers To Review 1stHakuzen KairoNo ratings yet
- Multidimensional Scale of Perceived Social Support (MSPSS) - Scale Items and Scoring InformationDocument3 pagesMultidimensional Scale of Perceived Social Support (MSPSS) - Scale Items and Scoring InformationAna-Maria ChiricNo ratings yet
- Lesson 9 and Lesson 10Document17 pagesLesson 9 and Lesson 10Nathalie RuazolNo ratings yet
- Week 6 Stress Management 27032024 125617pmDocument14 pagesWeek 6 Stress Management 27032024 125617pmAbdul hanan MalikNo ratings yet
- FRM 1-F43 Healthy Beginnings Progress Record - William BrunneDocument2 pagesFRM 1-F43 Healthy Beginnings Progress Record - William Brunnevelinec04No ratings yet
- Ethics Module CompilationDocument129 pagesEthics Module CompilationMariella BalagtasNo ratings yet
- QUESTIONNAIREDocument2 pagesQUESTIONNAIREKerbyNo ratings yet
- Rowan AppendixDocument4 pagesRowan AppendixVille SalmensuuNo ratings yet
- Do It NOW Habit Program Day # 2 - : Illusion - Fear of SuccessDocument5 pagesDo It NOW Habit Program Day # 2 - : Illusion - Fear of SuccessLudovic Tsondo MewoutouNo ratings yet
- Geriatric PhlebotomyDocument4 pagesGeriatric PhlebotomyNanda Dyah Ayu100% (1)
- How To Handle Difficult People - Pocket GuideDocument8 pagesHow To Handle Difficult People - Pocket GuideAngel SorianoNo ratings yet
- Crucial Conversations 160217195837 PDFDocument244 pagesCrucial Conversations 160217195837 PDFShashank Nema100% (2)
- How You Can Help Someone With Depression: Fact SheetDocument2 pagesHow You Can Help Someone With Depression: Fact SheetBailey YeeNo ratings yet
- Support StrategiesDocument1 pageSupport StrategiesMary Angelie AmbojiaNo ratings yet
- Self-Actuali ZationDocument5 pagesSelf-Actuali ZationRittici Colie PepitoNo ratings yet
- Coping With Loss FinalDocument100 pagesCoping With Loss Finalpfighterer100% (3)
- From Difficult To Effective PeopleDocument92 pagesFrom Difficult To Effective Peopleharold carbonelNo ratings yet
- Mark Walsh - People UnpleasingDocument79 pagesMark Walsh - People UnpleasingchucknpNo ratings yet
- FRM 1-F43 Healthy Beginnings Progress Record 2Document2 pagesFRM 1-F43 Healthy Beginnings Progress Record 2velinec04No ratings yet
- M2 Johari Window WorksheetDocument4 pagesM2 Johari Window WorksheetMariven VelardeNo ratings yet
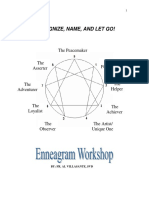
- Recognize, Name, and Let Go!: The Peacemaker The Perfectionist The AsserterDocument36 pagesRecognize, Name, and Let Go!: The Peacemaker The Perfectionist The AsserterEmmeliza Labella100% (1)
- Psychological First Aid: Supporting People in The Aftermath of Crisis EventsDocument47 pagesPsychological First Aid: Supporting People in The Aftermath of Crisis EventsLadymae Barneso SamalNo ratings yet
- Child & Adolescent Thoery ReviewDocument75 pagesChild & Adolescent Thoery ReviewAlphaMaleYoongiNo ratings yet
- The Role of Parents in Inclusive SettingDocument33 pagesThe Role of Parents in Inclusive SettingSansui Labartinos CobarrubiasNo ratings yet
- Seminar On Stress Mangament at M-4 18-11-08 (16.11)Document151 pagesSeminar On Stress Mangament at M-4 18-11-08 (16.11)Laiba WarisNo ratings yet
- Type 9Document15 pagesType 9pundirNo ratings yet
- Why Adults Should Learn To Kids : - 9 ReasonsDocument5 pagesWhy Adults Should Learn To Kids : - 9 Reasonsclary herondaleNo ratings yet
- CounteringDepression 5ResilienceBuildingBlocksDocument8 pagesCounteringDepression 5ResilienceBuildingBlocksmetacognizantNo ratings yet
- V7WK66jPQjO8Os06beAk 5 Step To Stop People PleasingDocument14 pagesV7WK66jPQjO8Os06beAk 5 Step To Stop People PleasingBelosnezhkaNo ratings yet
- Bystander and AllyDocument13 pagesBystander and AllyArkadyuti Ghosh RoyNo ratings yet
- PER DEV POINTERS TO REVIEW 1st 1Document5 pagesPER DEV POINTERS TO REVIEW 1st 1sieNo ratings yet
- Adler PresentationDocument11 pagesAdler PresentationJoanne ChuaNo ratings yet
- Helping Children and Adolescents Cope With Traumatic EventsDocument2 pagesHelping Children and Adolescents Cope With Traumatic Eventstatiana martinezNo ratings yet
- RM Practical ScalesDocument12 pagesRM Practical ScalesAPOORVA PANDEYNo ratings yet
- Personality Type 6Document6 pagesPersonality Type 6Den PaccotNo ratings yet
- The Process of Grief PDFDocument6 pagesThe Process of Grief PDFnicoletagr2744100% (1)
- Assertiveness Is Frequently MisunderstoodDocument6 pagesAssertiveness Is Frequently MisunderstoodsarayooNo ratings yet
- Anger Management: Presented By: Lolita V. Bucot RGCDocument54 pagesAnger Management: Presented By: Lolita V. Bucot RGCResty FloresNo ratings yet
- FRM 1-F43 Healthy Beginnings Progress Record - Arrian HuntDocument2 pagesFRM 1-F43 Healthy Beginnings Progress Record - Arrian Huntvelinec04No ratings yet
- Trauma and Mental HealthDocument1 pageTrauma and Mental Healthyoungresearcher2023No ratings yet
- Alabama Mental Health Intake & Evaluation: Current FunctioningDocument3 pagesAlabama Mental Health Intake & Evaluation: Current FunctioningRobertoTapiaHidalgoNo ratings yet
- Agreeableness: Compassion & Politeness: Lecture Notes 5Document8 pagesAgreeableness: Compassion & Politeness: Lecture Notes 5Danilo PesicNo ratings yet
- Gen 002 Sas 11Document3 pagesGen 002 Sas 11Jeame100% (1)
- 09 Student Inventory FormDocument3 pages09 Student Inventory FormJay-ar ArtocillaNo ratings yet
- Menjadi Teman Baik: Mencegah "Self Harm"Document28 pagesMenjadi Teman Baik: Mencegah "Self Harm"nina arianyNo ratings yet
- Grief WorkbookDocument21 pagesGrief Workbookkathie76No ratings yet
- 7 SelfsoothingDocument4 pages7 Selfsoothingmarilyne.rNo ratings yet
- Headington - After A Critical IncindentDocument2 pagesHeadington - After A Critical IncindentjohnzatkowskyNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptYeremias EdwinNo ratings yet
- Position Summary:: Cook Helper 1Document3 pagesPosition Summary:: Cook Helper 1O LalaNo ratings yet
- Essential Newborn CareDocument14 pagesEssential Newborn CareJam Corros100% (1)
- Breakingnewsenglish: China Coronavirus Heightens Global Alarm True / FalseDocument2 pagesBreakingnewsenglish: China Coronavirus Heightens Global Alarm True / FalseElenNo ratings yet
- Checklist - Applying A Sterile Gown and Performing Closed GlovingDocument1 pageChecklist - Applying A Sterile Gown and Performing Closed GlovingDonaJeanNo ratings yet
- Neck Disability Index Ndi Editable 1Document2 pagesNeck Disability Index Ndi Editable 1api-512652362No ratings yet
- Science Technology and Society Is Social Networking Boon in Society?Document12 pagesScience Technology and Society Is Social Networking Boon in Society?Jubilea PresentacionNo ratings yet
- China Paint - Golden Flower Supreme Wall Finish (Material Data) (English)Document7 pagesChina Paint - Golden Flower Supreme Wall Finish (Material Data) (English)TMNo ratings yet
- Nose, Mouth, Throat and NeckDocument58 pagesNose, Mouth, Throat and NeckGloriaCoronado90% (10)
- ACI 369R-11 Guide For Seismic Rehabilitation of Existing Concrete Frame BuildingsDocument39 pagesACI 369R-11 Guide For Seismic Rehabilitation of Existing Concrete Frame Buildingsperezleon.rdNo ratings yet
- Mass Communication Project Topics With Materials in CameroonDocument7 pagesMass Communication Project Topics With Materials in CameroonHashmi SutariyaNo ratings yet
- PSM AllenDocument210 pagesPSM AllenDeeptiNo ratings yet
- Oxidation Pond: Presented by Pawan R. Jadhao Under The Guidance of Joshi MademDocument18 pagesOxidation Pond: Presented by Pawan R. Jadhao Under The Guidance of Joshi MademdhanushNo ratings yet
- Evacuation, Relocation & HibernationDocument27 pagesEvacuation, Relocation & HibernationIts Mind's Eye100% (1)
- Cymbopogon Citratus (Lemon Grass), Garlic Clove Skin, and Azadirachta Indica (NeemDocument29 pagesCymbopogon Citratus (Lemon Grass), Garlic Clove Skin, and Azadirachta Indica (NeemJohn Drake TagavillaNo ratings yet
- The Silencing The Self ScaleDocument4 pagesThe Silencing The Self ScaleHarsiddhi ThakralNo ratings yet
- A Project Report: SubjectDocument11 pagesA Project Report: SubjectAkhter MalikNo ratings yet
- APRIL 2021 JAMS FRIDAY - MauricioDocument8 pagesAPRIL 2021 JAMS FRIDAY - MauricioDanikaNo ratings yet
- Industrial Traning Report AT: Glaxosmithkline Consumer Health Care LTDDocument4 pagesIndustrial Traning Report AT: Glaxosmithkline Consumer Health Care LTDno1guessmeNo ratings yet
- Ebook Family Interventions in Mental Health - (PG 18 - 80)Document63 pagesEbook Family Interventions in Mental Health - (PG 18 - 80)daniladaneta queensaNo ratings yet
- Current Analysis of Hangings That Deviates From Recently Published StudiesDocument7 pagesCurrent Analysis of Hangings That Deviates From Recently Published StudiesWAN MOHAMMAD HAFIZ BIN WAN RAZALINo ratings yet
- Dentoalveolar Surgery 1 05Document76 pagesDentoalveolar Surgery 1 05I Putu Aditya Putra WirawanNo ratings yet
- Unit 3 HSE Mark Scheme Jan 2022Document18 pagesUnit 3 HSE Mark Scheme Jan 2022jamilaakhatunnNo ratings yet
- Rubber Seed Cleansing Oil Formulation and Its Efficacy of Makeup RemoverDocument10 pagesRubber Seed Cleansing Oil Formulation and Its Efficacy of Makeup RemoverCHINTHIA RAHADI PUTRINo ratings yet
- Essays For Academic WritingDocument79 pagesEssays For Academic Writingasma rajabNo ratings yet
- Sacral OMM GuideDocument4 pagesSacral OMM GuideSameer AkhtarNo ratings yet
- PDET Webinar2 FinalDocument36 pagesPDET Webinar2 FinalEr WinNo ratings yet
- Three Months From The Date of Engagement To Manage The COVID-19 Wards atDocument8 pagesThree Months From The Date of Engagement To Manage The COVID-19 Wards atKumar ReddyNo ratings yet
- Dorothea Orem Is A Nurse Theorist Who Pioneered The SelfDocument14 pagesDorothea Orem Is A Nurse Theorist Who Pioneered The SelfAthira PSNo ratings yet