You might also like
- Iron Adequacy During Pregnancy.11Document1 pageIron Adequacy During Pregnancy.11Em Wahyu ArNo ratings yet
- Andrews1999 MetbolDocument10 pagesAndrews1999 Metbolida ayu agung WijayantiNo ratings yet
- Calcium Bioavailability and Absorption: A Review1: Lindsay H. Allen, PH.D., R.DDocument26 pagesCalcium Bioavailability and Absorption: A Review1: Lindsay H. Allen, PH.D., R.DluisemrNo ratings yet
- Desordenes Del Magnesio RevisionDocument13 pagesDesordenes Del Magnesio RevisionjosedegibesNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFmigil66256No ratings yet
- Calcium - and - Calcium - Salts Elemental CalciumDocument5 pagesCalcium - and - Calcium - Salts Elemental Calciumfariha farheenNo ratings yet
- Monsen 1978Document8 pagesMonsen 1978MILENKA PAZ KOPORCIC ZUÑIGANo ratings yet
- 24 DC Calcium and Calcium SaltsDocument4 pages24 DC Calcium and Calcium SaltsSudhir ChughNo ratings yet
- Mcknight Et Al 2023 bf3 Catalyzed Intramolecular Fluorocarbamoylation of Alkynes Via Halide RecyclingDocument7 pagesMcknight Et Al 2023 bf3 Catalyzed Intramolecular Fluorocarbamoylation of Alkynes Via Halide Recyclingrizzo.lorenzo94No ratings yet
- Strategy To Achieve Iron Adequacy To Support Children's Growth and DevelopmentDocument36 pagesStrategy To Achieve Iron Adequacy To Support Children's Growth and DevelopmentJayantiNo ratings yet
- MusselByssusFibresATough ChapterDocument26 pagesMusselByssusFibresATough ChapterMental MohanNo ratings yet
- Diet and Therapy: Micronutrients: MINERALSDocument7 pagesDiet and Therapy: Micronutrients: MINERALSCHINGCHONG SLAYERNo ratings yet
- Reddy 2018Document6 pagesReddy 2018Yosoa OktavianusNo ratings yet
- Food and Nutrition MFN 004 Unit 10Document61 pagesFood and Nutrition MFN 004 Unit 10SHAHI'S CREATIONNo ratings yet
- Introduction and History of Dental CariesDocument112 pagesIntroduction and History of Dental Cariesrasagna reddyNo ratings yet
- Oral Iron Supplementation in Iron-Deficient Women-How Much and How OftenDocument9 pagesOral Iron Supplementation in Iron-Deficient Women-How Much and How Oftenshofa nur rahmannisaNo ratings yet
- GIN DSL2 - StudentDocument3 pagesGIN DSL2 - StudentjexshimadaNo ratings yet
- Chromium BrochureDocument2 pagesChromium BrochurevietvuducNo ratings yet
- Combination: The TreatmentDocument10 pagesCombination: The TreatmentAlinoor mondolNo ratings yet
- Comparison of Global Responses To Mild Deficiency and Excess Copper Levels in Arabidopsis SeedlingsDocument13 pagesComparison of Global Responses To Mild Deficiency and Excess Copper Levels in Arabidopsis SeedlingsAdrianNo ratings yet
- Ascorbic Acid: An Enhancing Factor in Iron AbsorptionDocument11 pagesAscorbic Acid: An Enhancing Factor in Iron AbsorptionТатьяна СаенкоNo ratings yet
- Quantitative Assessment of Enhanced Sintering ConceptsDocument9 pagesQuantitative Assessment of Enhanced Sintering ConceptsfarageNo ratings yet
- E Cient Vacuum-Deposited Perovskite Solar Cells With Stable Cubic Fa Ma PbiDocument9 pagesE Cient Vacuum-Deposited Perovskite Solar Cells With Stable Cubic Fa Ma PbiIsmael AnconaNo ratings yet
- A Ferrop BloodDocument2 pagesA Ferrop BloodAnaNo ratings yet
- Diseases of Hepatic Iron and Copper MetabolismDocument13 pagesDiseases of Hepatic Iron and Copper Metabolismputri riszaNo ratings yet
- A Tris - (Manganese (III) ) Corrole-Porphyrin-Corrole TriadDocument9 pagesA Tris - (Manganese (III) ) Corrole-Porphyrin-Corrole TriadMurugavel MuthuchamyNo ratings yet
- Iron Metabolism Chapter SummaryDocument3 pagesIron Metabolism Chapter SummaryAira UsiNo ratings yet
- Vitamins - It Must Be A Vital Organic Substance That Is Not An Energy-Producing Carbohydrate, Fat or Protein and Usually NecessaryDocument9 pagesVitamins - It Must Be A Vital Organic Substance That Is Not An Energy-Producing Carbohydrate, Fat or Protein and Usually NecessaryGia Espinosa OcbeñaNo ratings yet
- Iron Deficiency Anemia Risk Factors in ChildrenDocument19 pagesIron Deficiency Anemia Risk Factors in ChildrenNadiaa RamadhaniNo ratings yet
- Chemcomm: CommunicationDocument4 pagesChemcomm: CommunicationAntônio Neto MachadoNo ratings yet
- Understanding The Logistics For The Distribution of Heme in CellsDocument15 pagesUnderstanding The Logistics For The Distribution of Heme in CellsJosiel Nasc'mentoNo ratings yet
- Festing On Minerals Science 2010Document2 pagesFesting On Minerals Science 2010Simon BeardNo ratings yet
- Iron IVDocument7 pagesIron IVSiswanto H. AzwarNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFAleksandra AngelkovskaNo ratings yet
- The Kidney Dysfunction Epidemic, Part 1: CausesDocument6 pagesThe Kidney Dysfunction Epidemic, Part 1: CausesMuhammad Salah AliNo ratings yet
- Drug Study SacroilliacDocument3 pagesDrug Study SacroilliacRose Ann CuaresmaNo ratings yet
- 1976 Changes in Fecal Composition and Colonic Function Due To Cereal FiberDocument6 pages1976 Changes in Fecal Composition and Colonic Function Due To Cereal FiberMyriam CardenasNo ratings yet
- Calcium and Vitamin D Supplement Safety Fact SheetsDocument3 pagesCalcium and Vitamin D Supplement Safety Fact SheetsTaufikNo ratings yet
- (IM A) (Hema) IDA and Hypoproliferative Anemias-Dr. Perez 2 (Kim Villanueva)Document5 pages(IM A) (Hema) IDA and Hypoproliferative Anemias-Dr. Perez 2 (Kim Villanueva)NoreenNo ratings yet
- CarbohydrateDocument12 pagesCarbohydrateBinh KieuNo ratings yet
- PosterDocument1 pagePosteryaswanth27497No ratings yet
- SiabiDocument4 pagesSiabiReaccion quimicaNo ratings yet
- Siderophore-Based Iron Acquisition and Pathogen Control: Marcus Miethke and Mohamed A. MarahielDocument39 pagesSiderophore-Based Iron Acquisition and Pathogen Control: Marcus Miethke and Mohamed A. MarahielSergio A. ResendizNo ratings yet
- Medicines: A Short Review of Iron Metabolism and Pathophysiology of Iron DisordersDocument15 pagesMedicines: A Short Review of Iron Metabolism and Pathophysiology of Iron DisordersClaudiaNo ratings yet
- Quartz Disrupts Iron HomeostasisDocument11 pagesQuartz Disrupts Iron HomeostasisJocilene Dantas Torres NascimentoNo ratings yet
- Renal PDFDocument16 pagesRenal PDFsestramitaNo ratings yet
- The Contribution of The Large Intestine To Energy Supplies in Man1'2Document5 pagesThe Contribution of The Large Intestine To Energy Supplies in Man1'2gopnarayansamyakNo ratings yet
- Proteins and Protein MetabolismDocument9 pagesProteins and Protein MetabolismclaireNo ratings yet
- Improving feed efficiency with a combination of seaweed extracts and micronized clayDocument2 pagesImproving feed efficiency with a combination of seaweed extracts and micronized clayDrivailaNo ratings yet
- MindmapDocument1 pageMindmapSng Gim ChoonNo ratings yet
- Diagnosis and Management of Iron Deficiency Anemia in The 21st CenturyDocument8 pagesDiagnosis and Management of Iron Deficiency Anemia in The 21st CenturyNur AlamNo ratings yet
- Agronomic study on aluminum neutralization and phosphorus uptake in three Costa Rican soilsDocument13 pagesAgronomic study on aluminum neutralization and phosphorus uptake in three Costa Rican soilsGabriel CespedesNo ratings yet
- Mizrahi 2021Document14 pagesMizrahi 2021Nicolas PeñarandaNo ratings yet
- Adquisición de Hierro en Leishmania y Su Papel Crucial en La InfecciónDocument11 pagesAdquisición de Hierro en Leishmania y Su Papel Crucial en La InfecciónKatharina DPNo ratings yet
- FulltextDocument5 pagesFulltextkj44No ratings yet
- Engl, Reiser - 2020Document8 pagesEngl, Reiser - 2020franciscaNo ratings yet
- Associations of education level and dietary factors with anemia in pregnant womenDocument8 pagesAssociations of education level and dietary factors with anemia in pregnant womenAndi RahmadNo ratings yet
- Relationship Between Animal Protein & Hemoglobin in Pregnant WomenDocument6 pagesRelationship Between Animal Protein & Hemoglobin in Pregnant WomenAndi RahmadNo ratings yet
- 970 - WOF Missing The 2025 Global Targets Report ARTDocument242 pages970 - WOF Missing The 2025 Global Targets Report ARTAndi RahmadNo ratings yet
- 2020 Global Nutrition Report 2hrsskoDocument168 pages2020 Global Nutrition Report 2hrsskoAndi RahmadNo ratings yet
- 354-Article Text-920-1-10-20210630Document9 pages354-Article Text-920-1-10-20210630Andi RahmadNo ratings yet
- Dietary Pattern Change and Acculturation of Chinese Americans in PennsylvaniaDocument8 pagesDietary Pattern Change and Acculturation of Chinese Americans in PennsylvaniaAndi RahmadNo ratings yet
- Ideal cardiovascular health among populationsDocument2 pagesIdeal cardiovascular health among populationsAndi RahmadNo ratings yet
- The Impact of Globalization On Migration Processes Ramunė Čiarnienė, Vilmantė KumpikaitėDocument7 pagesThe Impact of Globalization On Migration Processes Ramunė Čiarnienė, Vilmantė KumpikaitėVic KeyNo ratings yet
- Family Size, Poverty and Social Exclusion: Evidence From Select Communities in Edo State, Nigeria Sunday Olufemi Akintelu, PHDDocument8 pagesFamily Size, Poverty and Social Exclusion: Evidence From Select Communities in Edo State, Nigeria Sunday Olufemi Akintelu, PHDAndi RahmadNo ratings yet
- Jurnal Mahasiwa Ilmu Administrasi Publik (JMIAP)Document11 pagesJurnal Mahasiwa Ilmu Administrasi Publik (JMIAP)Andi RahmadNo ratings yet
- Telaah Kritis Artikel Review SistematikDocument4 pagesTelaah Kritis Artikel Review SistematikNorbertus MacekaNo ratings yet
- Comments On Dietary Restriction, Okinawa Diet and Longevity: Clinical Section / DebateDocument3 pagesComments On Dietary Restriction, Okinawa Diet and Longevity: Clinical Section / DebateAndi RahmadNo ratings yet
- Okinawa: An Exception To The Social Gradient of Life Expectancy in JapanDocument5 pagesOkinawa: An Exception To The Social Gradient of Life Expectancy in JapanAndi RahmadNo ratings yet
- HIV/AIDS: Nutritional Implications and Impact On Human DevelopmentDocument5 pagesHIV/AIDS: Nutritional Implications and Impact On Human DevelopmentAndi RahmadNo ratings yet
- 237 665 3 PBDocument12 pages237 665 3 PBNers AnggaNo ratings yet
- Daftar Pustaka GizMolDocument1 pageDaftar Pustaka GizMolAndi RahmadNo ratings yet
- Vol. 2, No.5, Mei 2021Document6 pagesVol. 2, No.5, Mei 2021Andi RahmadNo ratings yet
- Is BIS Ready For Prime Time As The Gold Standard Measure?: January 2009Document6 pagesIs BIS Ready For Prime Time As The Gold Standard Measure?: January 2009Andi RahmadNo ratings yet
- Literature Review: The Affecting Factors of Low Coverage of Early Initiation Breastfeeding and Exclusive BreastfeeedingDocument8 pagesLiterature Review: The Affecting Factors of Low Coverage of Early Initiation Breastfeeding and Exclusive BreastfeeedingAndi RahmadNo ratings yet
- Torsvik2015 Article MotorDevelopmentRelatedToDuratDocument11 pagesTorsvik2015 Article MotorDevelopmentRelatedToDuratAndi RahmadNo ratings yet
- 85 1 147 1 10 20170210 PDFDocument8 pages85 1 147 1 10 20170210 PDFnunuyNo ratings yet
- 45-Article Text-301-1-10-20200731Document14 pages45-Article Text-301-1-10-20200731Andi RahmadNo ratings yet
- Prenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionDocument42 pagesPrenatal Development and Birth: The Developing Person Through The Life Span Kathleen Stassen Berger - Tenth EditionJoel PayneNo ratings yet
- Browne2018-A Guide To Policy Analysis As A Research MethodDocument14 pagesBrowne2018-A Guide To Policy Analysis As A Research MethodIzza Dinalhaque PranatasariNo ratings yet
- The Psychosocial Impact of Extreme Gaming On Indian Pubg Gamers: The Case of Pubg (Playerunknown'S Battlegrounds)Document8 pagesThe Psychosocial Impact of Extreme Gaming On Indian Pubg Gamers: The Case of Pubg (Playerunknown'S Battlegrounds)qhdpjqofoexsdfbsygNo ratings yet
- National Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesDocument11 pagesNational Children's Science Congress: NCSC 2022 and 2023 Focal Theme and Sub-ThemesnkhiangteNo ratings yet
- Parasitology SummaryDocument7 pagesParasitology Summaryshiner99100% (1)
- B. Bruce Myers, MD PHD FACSDocument5 pagesB. Bruce Myers, MD PHD FACSallison8844No ratings yet
- CASE 1 - Los AngelesDocument2 pagesCASE 1 - Los Angeleshyunsuk fhebieNo ratings yet
- Assignment On PrincipalDocument10 pagesAssignment On PrincipalmacmohitNo ratings yet
- Total Penectomy Urooncology 12thDocument10 pagesTotal Penectomy Urooncology 12thdr. Joko WibowoNo ratings yet
- Victoria DePonceau SPD ResumeDocument1 pageVictoria DePonceau SPD ResumeVictoria Leigh DePonceauNo ratings yet
- Acute Myeloid LeukemiaDocument14 pagesAcute Myeloid Leukemiaapi-247402827No ratings yet
- Glander DiseaseDocument1 pageGlander DiseaseAdams10No ratings yet
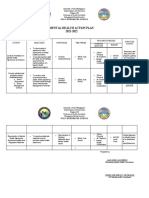
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
- Ibm India Benefits - Covid-19 Help Line & Doctor Tele-ConsultationDocument4 pagesIbm India Benefits - Covid-19 Help Line & Doctor Tele-ConsultationSushovan NandiNo ratings yet
- Efficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsDocument6 pagesEfficacy of Facet Block in Lumbar Facet Joint Syndrome PatientsthiagoNo ratings yet
- Proposal Project - PortfolioDocument21 pagesProposal Project - Portfolioapi-548552942No ratings yet
- Onsent To Hiropractic Reatment: BenefitsDocument2 pagesOnsent To Hiropractic Reatment: BenefitsRajender BishtNo ratings yet
- Summary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDocument34 pagesSummary of Consensus Statements On The Diagnosis and Management of COPD in The PhilippinesDivye GuptaNo ratings yet
- Mere WaliDocument7 pagesMere WaliMaliCk TaimoorNo ratings yet
- Cohort Study Meat Intake An Cancer RiskDocument8 pagesCohort Study Meat Intake An Cancer RiskHarunNo ratings yet
- Birth asphyxia causes and neonatal resuscitationDocument20 pagesBirth asphyxia causes and neonatal resuscitationinne_fNo ratings yet
- Theodore Millon On Rosenhan PaperDocument6 pagesTheodore Millon On Rosenhan PaperJuliette WarnesNo ratings yet
- SKF MSDS LGHP 2 PDFDocument5 pagesSKF MSDS LGHP 2 PDFMunkhnasan MonaNo ratings yet
- Drug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameterDocument5 pagesDrug Classification Indication Action and Pharmacokinetics Contraindication Adverse Effect Monitoring ParameteryssatNo ratings yet
- Midterm Surgery PYQsDocument77 pagesMidterm Surgery PYQs6vqk4z8wnhNo ratings yet
- Brain Teasers #1 Daniela On FireDocument3 pagesBrain Teasers #1 Daniela On FireEarl Cris RiggsNo ratings yet
- Dragon BoatDocument7 pagesDragon BoatandrewadrianNo ratings yet
- Determinants of optimal learning assessmentDocument1 pageDeterminants of optimal learning assessmentKenj PereñaNo ratings yet
- O and G Notes Notebank NumberedDocument173 pagesO and G Notes Notebank NumberedPerscitus Ali القحطانيNo ratings yet
- Biology InvestigatoryDocument6 pagesBiology InvestigatoryAananthan Jayvardan100% (2)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- CBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerFrom EverandCBT Strategies: CBT Strategies for Overcoming Panic, Fear, Depression, Anxiety, Worry, and AngerNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- How To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeFrom EverandHow To Understand Your Anger For Better Mental Health: How To Control Emotions And Eliminate Stress In Your LifeNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Inmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedFrom EverandInmersion Into The Shadown Effective Method Of Dark Psychology: How To Use The Best Persuasion Techniques To Achieve Your Best Goals And How To Protect Yourself From Being ManipulatedRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)