You might also like
- Nursing Care Plan For "Fluid and Electrolyte Imbalances"Document37 pagesNursing Care Plan For "Fluid and Electrolyte Imbalances"jhonroks90% (50)
- Obsessive-Compulsive Disorder (OCD) Screening ToolDocument2 pagesObsessive-Compulsive Disorder (OCD) Screening ToolManiya Dianne ReyesNo ratings yet
- Eat What You Love, Love What You Eat With Diabetes: A Mindful Eating Program for Thriving with Prediabetes or DiabetesFrom EverandEat What You Love, Love What You Eat With Diabetes: A Mindful Eating Program for Thriving with Prediabetes or DiabetesNo ratings yet
- Healing Codes: Grigori GrabovoiDocument47 pagesHealing Codes: Grigori GrabovoiPanther MelchizedekNo ratings yet
- DSMES Assessment Template (Chart 7)Document5 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Questionaire - Reasearch Group-2Document4 pagesQuestionaire - Reasearch Group-2Salah Ud DinNo ratings yet
- Hydration Questionnaire for TeensDocument10 pagesHydration Questionnaire for TeensChristina ValeriaNo ratings yet
- Rhinessa Women's Q EnglishDocument8 pagesRhinessa Women's Q EnglishDavis ShirleyNo ratings yet
- Mental health assessment formDocument6 pagesMental health assessment formalotfya100% (1)
- FxNA Intake Form FillableDocument20 pagesFxNA Intake Form Fillablepgp.suscripcionesNo ratings yet
- Dsmes Intervention Tracking Form: 8/15/1938 Participant 7Document1 pageDsmes Intervention Tracking Form: 8/15/1938 Participant 7Bryan MorteraNo ratings yet
- General, Medical and Health Information: Lifestyle & Diabetes QuestionnaireDocument10 pagesGeneral, Medical and Health Information: Lifestyle & Diabetes QuestionnairerizkymutiaNo ratings yet
- Patient'S ProfileDocument17 pagesPatient'S ProfileLucas JelmarNo ratings yet
- New Patient Registration FormDocument4 pagesNew Patient Registration Formapi-358908929No ratings yet
- Nutrition Consultation FormDocument7 pagesNutrition Consultation FormRD Finders and Personal Training100% (5)
- Bariatrics Weight Loss IntakeDocument12 pagesBariatrics Weight Loss IntakeErin abelsNo ratings yet
- Pre-diabetes lifestyle questionnaireDocument8 pagesPre-diabetes lifestyle questionnaireAndrei StefanNo ratings yet
- Client Intake FormDocument9 pagesClient Intake FormPrabha GuptaNo ratings yet
- Child Nutrition Assessment 1Document1 pageChild Nutrition Assessment 1SHAILAJA SORTENo ratings yet
- Personal health data for nursing studentDocument8 pagesPersonal health data for nursing studentJenny AjocNo ratings yet
- Health Questionnaire: MohamadDocument2 pagesHealth Questionnaire: MohamadMoh AmmNo ratings yet
- WeightLoss and Health Consultation FormDocument9 pagesWeightLoss and Health Consultation Formsam JayakaranNo ratings yet
- UW Autism Center Intake FormDocument10 pagesUW Autism Center Intake FormPrabha GuptaNo ratings yet
- Your Family Medical History Questionnaire: All About YouDocument5 pagesYour Family Medical History Questionnaire: All About YouLemuel Glenn BautistaNo ratings yet
- 1.annual Physical Therapy Visit For Aging Adult-Intake FormDocument5 pages1.annual Physical Therapy Visit For Aging Adult-Intake FormReza ANo ratings yet
- TIP - Blood Pressure - Adult - ENGLISH - 2020Document1 pageTIP - Blood Pressure - Adult - ENGLISH - 2020Sabrina RobertsNo ratings yet
- Patient Feedback QuestionnaireDocument2 pagesPatient Feedback QuestionnaireRanu AbhinavNo ratings yet
- New-Patient-Medical-History-Form-2023-03-29Document2 pagesNew-Patient-Medical-History-Form-2023-03-29Trouvaille medicoNo ratings yet
- Eat Fat Get Thin 21 Day PLanDocument33 pagesEat Fat Get Thin 21 Day PLanNone100% (1)
- General Assesmnet FormDocument3 pagesGeneral Assesmnet FormNoor FatimaNo ratings yet
- Weight Loss Resistance ProfileDocument4 pagesWeight Loss Resistance ProfileNadine TengcoNo ratings yet
- Brfss Round1 CountyDocument15 pagesBrfss Round1 CountyTeffyNo ratings yet
- PWS Nutrition MCukDocument33 pagesPWS Nutrition MCukMCuk2606No ratings yet
- A Lifetime of Good HealthDocument2 pagesA Lifetime of Good HealthAmy SNo ratings yet
- Patient Health History GuideDocument8 pagesPatient Health History GuideRalph Phillip CanillasNo ratings yet
- Six-Word Lessons to be Healthy Forever: 100 Lessons to Achieve and Sustain Lifelong HealthFrom EverandSix-Word Lessons to be Healthy Forever: 100 Lessons to Achieve and Sustain Lifelong HealthNo ratings yet
- AAAWM Community Survey 2019Document5 pagesAAAWM Community Survey 2019macoyo ormilloNo ratings yet
- Stop Dieting Start Thinning: 9 Golden Rules to Weight-Loss for People Who Love to EatFrom EverandStop Dieting Start Thinning: 9 Golden Rules to Weight-Loss for People Who Love to EatNo ratings yet
- Phase 9 Core Questionaire 508Document14 pagesPhase 9 Core Questionaire 508Bunda Happy 2023No ratings yet
- Survey Questionnaire 5-30-2013 FORM (Final) - DistributedDocument6 pagesSurvey Questionnaire 5-30-2013 FORM (Final) - Distributedom parkashNo ratings yet
- Ayurveda Wellness QuestionnaireDocument13 pagesAyurveda Wellness QuestionnaireNivetha.P 20CCA114No ratings yet
- DSMES Intervention Tracking (Chart 2)Document1 pageDSMES Intervention Tracking (Chart 2)Kitten MitsurugiNo ratings yet
- Caregiver Intake FormDocument16 pagesCaregiver Intake Formbtfd2ky4hhNo ratings yet
- Stay Healthy With Diabetes: Steps To Help YouDocument6 pagesStay Healthy With Diabetes: Steps To Help YoudgmtfmNo ratings yet
- Bonus Yale Food AddictionDocument2 pagesBonus Yale Food AddictionLeticia BarretoNo ratings yet
- Reverse DiabetesFrom EverandReverse DiabetesReader's DigestNo ratings yet
- Alabama Mental Health Intake & Evaluation: Current FunctioningDocument3 pagesAlabama Mental Health Intake & Evaluation: Current FunctioningRobertoTapiaHidalgoNo ratings yet
- The Healthy Smoothie Bible: Lose Weight, Detoxify, Fight Disease, and Live LongFrom EverandThe Healthy Smoothie Bible: Lose Weight, Detoxify, Fight Disease, and Live LongRating: 4 out of 5 stars4/5 (3)
- Diabetes Prevention For You and Your FamilyDocument24 pagesDiabetes Prevention For You and Your FamilySarfaraz ShahNo ratings yet
- 09 B Your Eating Habits PDFDocument1 page09 B Your Eating Habits PDFGhionna KelleyNo ratings yet
- The Gut RevelationDocument82 pagesThe Gut RevelationRajib DasNo ratings yet
- Nutrition Questionnaire ReviewDocument3 pagesNutrition Questionnaire Reviewseb_streitenbergerNo ratings yet
- Food System Assessment SurveyDocument2 pagesFood System Assessment SurveyBrian JohnstonNo ratings yet
- 4 Steps To Control Your Diabetes For Life Haitian CreoleDocument32 pages4 Steps To Control Your Diabetes For Life Haitian CreoleAn Seon YuNo ratings yet
- Eyes - Concise Medical SummaryDocument6 pagesEyes - Concise Medical SummaryAnand PatelNo ratings yet
- DIARRHEADocument39 pagesDIARRHEAJessa RedondoNo ratings yet
- DSMES Intervention Tracking Form (Chart 7) Bryan SignedDocument1 pageDSMES Intervention Tracking Form (Chart 7) Bryan SignedBryan MorteraNo ratings yet
- Instruction: Please Place A Tick in The Box Provided Or, Where Prompted, Write Briefly in The Space ProvidedDocument3 pagesInstruction: Please Place A Tick in The Box Provided Or, Where Prompted, Write Briefly in The Space ProvidedMark Anthony HenryNo ratings yet
- Skip To Main Content: o o o o o o o o o o o o o o o o o o o o o o o o oDocument10 pagesSkip To Main Content: o o o o o o o o o o o o o o o o o o o o o o o o oMike Kenji ShinodaNo ratings yet
- Protocolo de 3 Fases 2024Document305 pagesProtocolo de 3 Fases 2024Andreia TorresNo ratings yet
- Equality and Diversity Monitoring FormDocument2 pagesEquality and Diversity Monitoring FormsaikushalaNo ratings yet
- In-House Timesheet: Bryan F. M. Mortera IvDocument1 pageIn-House Timesheet: Bryan F. M. Mortera IvBryan MorteraNo ratings yet
- Patient List As of 09-01-2023 06 - 45 AMDocument20 pagesPatient List As of 09-01-2023 06 - 45 AMBryan MorteraNo ratings yet
- Bryan Florentino M. Mortera !V Sales and Operations: Name Working Hours 8 Department DATE SUBMITTED 8/08/2022Document5 pagesBryan Florentino M. Mortera !V Sales and Operations: Name Working Hours 8 Department DATE SUBMITTED 8/08/2022Bryan MorteraNo ratings yet
- Mortera, Bryan - 40hrsDocument1 pageMortera, Bryan - 40hrsBryan MorteraNo ratings yet
- Loreche-Amit V CDO MedicalDocument3 pagesLoreche-Amit V CDO MedicalJulia Camille RealNo ratings yet
- Corp CasesDocument15 pagesCorp CasesBryan MorteraNo ratings yet
- Patient List As of 09-01-2023 06 - 45 AMDocument20 pagesPatient List As of 09-01-2023 06 - 45 AMBryan MorteraNo ratings yet
- File Not Found!Document1 pageFile Not Found!Bryan MorteraNo ratings yet
- CPT Code 99091 BrewerDocument2 pagesCPT Code 99091 BrewerBryan MorteraNo ratings yet
- Updated DAR 4-24-23Document4 pagesUpdated DAR 4-24-23Bryan MorteraNo ratings yet
- In-House Timesheet: Bryan F. M. Mortera IvDocument1 pageIn-House Timesheet: Bryan F. M. Mortera IvBryan MorteraNo ratings yet
- CPT Code 99091 KovacDocument3 pagesCPT Code 99091 KovacBryan MorteraNo ratings yet
- WE 8-14-22 BryDocument1 pageWE 8-14-22 BryBryan MorteraNo ratings yet
- Dsmes Intervention Tracking Form: 8/15/1938 Participant 7Document1 pageDsmes Intervention Tracking Form: 8/15/1938 Participant 7Bryan MorteraNo ratings yet
- CPT Code 99091 ButlerDocument1 pageCPT Code 99091 ButlerBryan MorteraNo ratings yet
- CPT Code 99091 LathropDocument2 pagesCPT Code 99091 LathropBryan MorteraNo ratings yet
- Personal Data SheetDocument4 pagesPersonal Data SheetMitzie CañoNo ratings yet
- Updated DAR 4-24-23Document4 pagesUpdated DAR 4-24-23Bryan MorteraNo ratings yet
- Updated DAR 4-24-23Document4 pagesUpdated DAR 4-24-23Bryan MorteraNo ratings yet
- Weekly ActivityDocument5 pagesWeekly ActivityBryan MorteraNo ratings yet
- Updated DAR 4-24-23Document4 pagesUpdated DAR 4-24-23Bryan MorteraNo ratings yet
- Keefer, MichelleDocument1 pageKeefer, MichelleBryan MorteraNo ratings yet
- In-House Timesheet Tracking for Bryan MorteraDocument1 pageIn-House Timesheet Tracking for Bryan MorteraBryan MorteraNo ratings yet
- WE 8-14-22 BryDocument1 pageWE 8-14-22 BryBryan MorteraNo ratings yet
- DSMES Assessment Template (Chart 7)Document4 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- WE 8-14-22 BryDocument1 pageWE 8-14-22 BryBryan MorteraNo ratings yet
- Bass, PatriciaDocument1 pageBass, PatriciaBryan MorteraNo ratings yet
- DSMES Assessment Template (Chart 7)Document4 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- WE 8-14-22 BryDocument1 pageWE 8-14-22 BryBryan MorteraNo ratings yet
- In-House Timesheet Tracking for Bryan MorteraDocument1 pageIn-House Timesheet Tracking for Bryan MorteraBryan MorteraNo ratings yet
- Calcium and Phosphate Hormones: Vitamin D, Parathyroid Hormone, and Fibroblast Growth Factor 23Document11 pagesCalcium and Phosphate Hormones: Vitamin D, Parathyroid Hormone, and Fibroblast Growth Factor 23Handyka Vb GNo ratings yet
- SSC-CGL 2017 (PDFDrive - Com) PDFDocument152 pagesSSC-CGL 2017 (PDFDrive - Com) PDFSumit PandeyNo ratings yet
- DKA Guideline: Diagnosis and ManagementDocument4 pagesDKA Guideline: Diagnosis and ManagementHassen Kavi IsseNo ratings yet
- Ozone Therapy Reduces Oxidative Stress in Hashimoto's ThyroiditisDocument1 pageOzone Therapy Reduces Oxidative Stress in Hashimoto's ThyroiditisRegiane AmorimNo ratings yet
- Farmakokinetik - : Half LifeDocument50 pagesFarmakokinetik - : Half LifeHasna Nur FaridahNo ratings yet
- Performance Task 7 CCHMDocument3 pagesPerformance Task 7 CCHMHANNA CASANDRA GARCIANo ratings yet
- Suggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseDocument26 pagesSuggested Answers To Exercise, Reading To Learn and Cross-Topic ExerciseBernardNo ratings yet
- MIDC Hall Boisar Road Thane - 401501 Hba, Scre, TSH Self Swati Patil (40Y/F)Document5 pagesMIDC Hall Boisar Road Thane - 401501 Hba, Scre, TSH Self Swati Patil (40Y/F)TANUNo ratings yet
- Menopause - A Cardiometabolic Transition (Nappi Et Al., 2022)Document14 pagesMenopause - A Cardiometabolic Transition (Nappi Et Al., 2022)Susana RoyNo ratings yet
- LipidsDocument44 pagesLipidsMilena De CresentNo ratings yet
- Diagnosis of Canine Claw Disease - A Prospective Study of 24 DogsDocument9 pagesDiagnosis of Canine Claw Disease - A Prospective Study of 24 DogsjenNo ratings yet
- Sedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityDocument51 pagesSedative & Hypnotics: Prof. Hanan Hagar Pharmacology Department Medical College King Saud UniversityRose Ann Raquiza-PeranteNo ratings yet
- Human Anatomy and Physiology II: Biology 1414 Unit 8 Metabolism and NutritionDocument103 pagesHuman Anatomy and Physiology II: Biology 1414 Unit 8 Metabolism and Nutritionciroj25No ratings yet
- Fertilization: DR Sam ChimeDocument20 pagesFertilization: DR Sam ChimeJoshuaNo ratings yet
- Nahco3 AllopDocument3 pagesNahco3 AllopKurtt Evan ValinoNo ratings yet
- Endocrine System Communication and Target OrgansDocument19 pagesEndocrine System Communication and Target OrgansVENTURA, ANNIE M.No ratings yet
- Ratibrom 2Document2 pagesRatibrom 2Frontline0712No ratings yet
- DrugsDocument20 pagesDrugsLee Won100% (1)
- Uses of biochemical data in clinical diagnosis and managementDocument5 pagesUses of biochemical data in clinical diagnosis and managementnour achkarNo ratings yet
- PcolDocument1 pagePcolYnah CelesteNo ratings yet
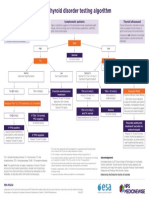
- NPS MedicineWise Thyroid Testing Algorithm v3Document1 pageNPS MedicineWise Thyroid Testing Algorithm v3Mikhael JHNo ratings yet
- 08 Jul 2023 Manipal LabReportDocument3 pages08 Jul 2023 Manipal LabReportMUKUL JANGIDNo ratings yet
- DextromethorphanDocument6 pagesDextromethorphanAbdelrhman AboodaNo ratings yet
- Expert Fat Loss GuideDocument66 pagesExpert Fat Loss GuideAmanda Rutllant100% (2)
- Week 6-8: Lipids and Nucleic Acids: 28 SEPTEMBER 2021 Ust Cloud CampusDocument21 pagesWeek 6-8: Lipids and Nucleic Acids: 28 SEPTEMBER 2021 Ust Cloud CampusEbina WhiteNo ratings yet
- Mispa I200 BrochureDocument2 pagesMispa I200 Brochurep11.sethiaNo ratings yet
- A Study to Assess the Effectiveness of Progressive Muscle Relaxation Technique on Dysmenorrhea Pain Management by Video Assisted Teaching among School Going Adolescent Girls at Roman Cathelic Matriculation High School, Vandavasi, Thiruvannamalai District, TamilnaduDocument2 pagesA Study to Assess the Effectiveness of Progressive Muscle Relaxation Technique on Dysmenorrhea Pain Management by Video Assisted Teaching among School Going Adolescent Girls at Roman Cathelic Matriculation High School, Vandavasi, Thiruvannamalai District, TamilnaduInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hemo 15Document2 pagesHemo 15ChureeshahNo ratings yet