You might also like
- AASM Scoring Manual Version 2.4 Berry Et Al. 2017Document89 pagesAASM Scoring Manual Version 2.4 Berry Et Al. 2017Jorge Borrani100% (4)
- Manual ID 800Document7 pagesManual ID 800akibae0% (1)
- Y625U - PCB Board Diagram PDFDocument2 pagesY625U - PCB Board Diagram PDFAlee LópezNo ratings yet
- Ch22 Presn PDFDocument34 pagesCh22 Presn PDFAlee LópezNo ratings yet
- Outline: - Error Correction Codes (Chapter 8) (Week 10 and 11)Document31 pagesOutline: - Error Correction Codes (Chapter 8) (Week 10 and 11)HarshaNo ratings yet
- High Frequency Voltage Controlled Ring Oscillators in Standard CMOSDocument18 pagesHigh Frequency Voltage Controlled Ring Oscillators in Standard CMOSKaan AyyildizNo ratings yet
- Introduction To Sigma Delta ConvertersDocument72 pagesIntroduction To Sigma Delta Convertershjtseng1974100% (1)
- High-Accuracy Readout Electronics For Piezoresistive Tactile SensorsDocument12 pagesHigh-Accuracy Readout Electronics For Piezoresistive Tactile SensorsMallikarjuna KorrapatiNo ratings yet
- FALLSEM2021-22 ECE2004 TH VL2021220101877 Reference Material I 09-09-2021 Smith Chart BasicDocument39 pagesFALLSEM2021-22 ECE2004 TH VL2021220101877 Reference Material I 09-09-2021 Smith Chart BasicTarun GopalanNo ratings yet
- ADC Part B ProgramsDocument12 pagesADC Part B ProgramsSahana ShaviNo ratings yet
- Effects of Frequency Characteristics of Reverberation Time On Listener EnvelopmentDocument6 pagesEffects of Frequency Characteristics of Reverberation Time On Listener EnvelopmentAlik RustamoffNo ratings yet
- Digital CommunicatiISI RAISED COSINEDocument15 pagesDigital CommunicatiISI RAISED COSINEMuhammad AwaisNo ratings yet
- Psoc Module Advanced Analog Design 11Document117 pagesPsoc Module Advanced Analog Design 11harsh100% (1)
- Probability Estimation Case Study: Molecular DynamicsDocument15 pagesProbability Estimation Case Study: Molecular DynamicsAlee LópezNo ratings yet
- Useful Formula Sheet and TablesDocument6 pagesUseful Formula Sheet and Tablesreuel nareshNo ratings yet
- Matlab Programs & OutputDocument71 pagesMatlab Programs & Outputajaiuchiha2003No ratings yet
- Guest 5Document68 pagesGuest 5api-3697260No ratings yet
- Frequency Response and Bode PlotsDocument43 pagesFrequency Response and Bode Plotszulusiphosi9No ratings yet
- L9-1 PidDocument14 pagesL9-1 PidTrần Kế HưngNo ratings yet
- Assignment 1 - Btech 10040 21Document14 pagesAssignment 1 - Btech 10040 21gvjbhknlkmNo ratings yet
- Signal Generator For Mikro Electronic CircuitsDocument31 pagesSignal Generator For Mikro Electronic CircuitsTeam PowerNo ratings yet
- Inverter Applications: - Motor DrivesDocument49 pagesInverter Applications: - Motor DrivesrajapeeeNo ratings yet
- Timing and Signalling Characteristics 36133-f10 - sA.7-A.8Document1,311 pagesTiming and Signalling Characteristics 36133-f10 - sA.7-A.8Luis Enrique GalloNo ratings yet
- Finite Word-Length EffectsDocument8 pagesFinite Word-Length EffectsRupali NerkarNo ratings yet
- Communication System MatlabDocument21 pagesCommunication System MatlabEysha qureshiNo ratings yet
- Function Approximation Case Study: Smart SensorDocument10 pagesFunction Approximation Case Study: Smart SensorAlee LópezNo ratings yet
- Response and Stability Analysis in Frequency DomainDocument54 pagesResponse and Stability Analysis in Frequency DomainMYNAMENo ratings yet
- Lecture10 Ee720 Jitter PDFDocument25 pagesLecture10 Ee720 Jitter PDFMohamed MegahedNo ratings yet
- Module - 4-4 - Multi-Stage AmplifiersDocument24 pagesModule - 4-4 - Multi-Stage AmplifiersshoukatawaisaliNo ratings yet
- EITN90 Radar and Remote SensingDocument41 pagesEITN90 Radar and Remote Sensingtdtiog hohdedkkNo ratings yet
- Multi-Band Antenna For Different Wireless ApplicationsDocument4 pagesMulti-Band Antenna For Different Wireless Applicationsamira moumedNo ratings yet
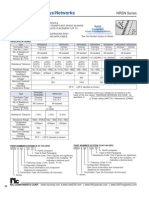
- NIC Components NRSN SeriesDocument5 pagesNIC Components NRSN SeriesNICCompNo ratings yet
- First and Second Order Filters: Ts asa s ωDocument66 pagesFirst and Second Order Filters: Ts asa s ωDilshan AnanthNo ratings yet
- Adc DacDocument15 pagesAdc Dackranthi59No ratings yet
- Chapter 5 (Frequency Response)Document79 pagesChapter 5 (Frequency Response)Nischal MaharjanNo ratings yet
- CiontrolLecturePartII 2020Document80 pagesCiontrolLecturePartII 2020Adithya RaoNo ratings yet
- EEE 1121 AC RevisedDocument109 pagesEEE 1121 AC RevisedMahiya KulsumNo ratings yet
- EN-ISO 17640: 2018 - EN-ISO 11666:2018: ScopeDocument4 pagesEN-ISO 17640: 2018 - EN-ISO 11666:2018: ScopeThomas SchotsNo ratings yet
- Developing and Testing Phased Array Ultrasonic TransducersDocument27 pagesDeveloping and Testing Phased Array Ultrasonic TransducersscribdmustaphaNo ratings yet
- Project 2 Report: ELEG 6913Document9 pagesProject 2 Report: ELEG 6913KirtikumarNo ratings yet
- Lec8 Numerical Distance ProtectionDocument24 pagesLec8 Numerical Distance ProtectionEVTNo ratings yet
- Chapter 8 (Lead Compensation)Document54 pagesChapter 8 (Lead Compensation)Nischal MaharjanNo ratings yet
- Shearail Punching Shear Reinforcement BS8110 Design Manual SO GBGBDocument10 pagesShearail Punching Shear Reinforcement BS8110 Design Manual SO GBGBNaziemi AhmadNo ratings yet
- Part IVDocument87 pagesPart IVAbel TayeNo ratings yet
- DSP5Document24 pagesDSP5udz76852No ratings yet
- S3979, S3931, S3932, S1352, S3270: One-Dimensional PSDDocument4 pagesS3979, S3931, S3932, S1352, S3270: One-Dimensional PSDSeba RodNo ratings yet
- Samsung Plasma Training ManualDocument57 pagesSamsung Plasma Training ManualLeonel AntonioNo ratings yet
- Chapter 9 17112020 070516pmDocument17 pagesChapter 9 17112020 070516pmR M RNo ratings yet
- MATH 174: Numerical Analysis: 1 Semester AY 2010-2011Document20 pagesMATH 174: Numerical Analysis: 1 Semester AY 2010-2011Joel Adrian SimbahanNo ratings yet
- Computation of Scattering Using The Finite Difference Time Domain (FDTD) MethodDocument7 pagesComputation of Scattering Using The Finite Difference Time Domain (FDTD) MethodAndyNo ratings yet
- S3979, S3931, S3932, S1352, S3270: One-Dimensional PSDDocument4 pagesS3979, S3931, S3932, S1352, S3270: One-Dimensional PSDmoyali25176750No ratings yet
- Experiment-1: Introduction To Optical Fiber CommunicationDocument37 pagesExperiment-1: Introduction To Optical Fiber CommunicationPallav KumarNo ratings yet
- %dit Ifft: All All 'Enter No of Points' 'Enter Array in Bit Reversal Order'Document8 pages%dit Ifft: All All 'Enter No of Points' 'Enter Array in Bit Reversal Order'Saravana JaiNo ratings yet
- BEE4223 Power Electronics & Drives SystemsDocument40 pagesBEE4223 Power Electronics & Drives Systemsmalathynarayani100% (1)
- Proteccionnes LDocument685 pagesProteccionnes LDarwinPeñafielNo ratings yet
- Product Specifications: MethodsDocument16 pagesProduct Specifications: Methodsgem1144aaNo ratings yet
- Gra 06 05Document12 pagesGra 06 05احمد ياسرNo ratings yet
- Vinodkumar Jagdale: NESGI, E & TC Department, Naigaon, PuneDocument62 pagesVinodkumar Jagdale: NESGI, E & TC Department, Naigaon, Punevk2you009No ratings yet
- Comparative Analysis Effect of Operating Time On Loss and Gain Characteristics of Quantum Dot Laser Using Group Iii NitridesDocument18 pagesComparative Analysis Effect of Operating Time On Loss and Gain Characteristics of Quantum Dot Laser Using Group Iii NitridesMd. Nawab Siraj Ud DaulaNo ratings yet
- Lec 1 Introduction Frequencty ResponseDocument61 pagesLec 1 Introduction Frequencty ResponseAli AhmadNo ratings yet
- Topic 7 Linear Regreation CHP14Document21 pagesTopic 7 Linear Regreation CHP14Natasha Mgt JoharNo ratings yet
- Impulse Responses of Ideal FiltersDocument25 pagesImpulse Responses of Ideal FiltersGhubaida HassaniNo ratings yet
- YogaDocument2 pagesYogaAlee LópezNo ratings yet
- Ch9 Presnedit PDFDocument22 pagesCh9 Presnedit PDFAlee LópezNo ratings yet
- Supervised Hebbian LearningDocument14 pagesSupervised Hebbian LearningAlee LópezNo ratings yet
- Prediction Case Study: Magnetic LevitationDocument15 pagesPrediction Case Study: Magnetic LevitationAlee LópezNo ratings yet
- Ch8 Presn PDFDocument24 pagesCh8 Presn PDFAlee LópezNo ratings yet
- Widrow-Hoff Learning: (LMS Algorithm)Document26 pagesWidrow-Hoff Learning: (LMS Algorithm)Alee LópezNo ratings yet
- Clustering Case Study: Forest Cover TypesDocument10 pagesClustering Case Study: Forest Cover TypesAlee LópezNo ratings yet
- Ch9 Presn PDFDocument22 pagesCh9 Presn PDFAlee LópezNo ratings yet
- Ch14 Presn PDFDocument47 pagesCh14 Presn PDFAlee LópezNo ratings yet
- Ch6 Presn PDFDocument24 pagesCh6 Presn PDFAlee LópezNo ratings yet
- Probability Estimation Case Study: Molecular DynamicsDocument15 pagesProbability Estimation Case Study: Molecular DynamicsAlee LópezNo ratings yet
- Widrow-Hoff Learning: (LMS Algorithm)Document26 pagesWidrow-Hoff Learning: (LMS Algorithm)Alee LópezNo ratings yet
- Ch19 Presn PDFDocument30 pagesCh19 Presn PDFAlee LópezNo ratings yet
- Ch22 Presn PDFDocument34 pagesCh22 Presn PDFAlee LópezNo ratings yet
- Ch17 Presn PDFDocument29 pagesCh17 Presn PDFAlee LópezNo ratings yet
- Function Approximation Case Study: Smart SensorDocument10 pagesFunction Approximation Case Study: Smart SensorAlee LópezNo ratings yet
- Ch12 Presn PDFDocument31 pagesCh12 Presn PDFAlee LópezNo ratings yet
- Understanding RF Circuits With Multisim 10Document136 pagesUnderstanding RF Circuits With Multisim 10DiegoNo ratings yet
- Hameg HM8131-2Document3 pagesHameg HM8131-2Fran Moreno0% (1)
- An Introduction To Neonatal EEGDocument8 pagesAn Introduction To Neonatal EEGfilzahnur joharNo ratings yet
- Ipc Notes PDFDocument19 pagesIpc Notes PDFdhruvNo ratings yet
- Preboard EST 2ndbatch April2015 SetBDocument15 pagesPreboard EST 2ndbatch April2015 SetBGeorge Ezar N. Quiriado100% (1)
- EEEB123 - Chapter 9 Sinusoids and PhasorsDocument79 pagesEEEB123 - Chapter 9 Sinusoids and PhasorsMuhammad Umair Felix0% (1)
- EXPT 03 - Digital Modulation - ASKDocument7 pagesEXPT 03 - Digital Modulation - ASKanika tabassumNo ratings yet
- Simple Self-Oscillating Class D Amplifier With Full Output Filter ControlDocument9 pagesSimple Self-Oscillating Class D Amplifier With Full Output Filter ControlEliecerNo ratings yet
- Introduction To Power QualityDocument13 pagesIntroduction To Power QualityShantanu gargNo ratings yet
- Amplitude Modulat ION: Communications Lab (EE351)Document5 pagesAmplitude Modulat ION: Communications Lab (EE351)Priyesh PandeyNo ratings yet
- MANUAL COMMUNICATION LAB-II, KEC-651,2020-21, Even SemDocument18 pagesMANUAL COMMUNICATION LAB-II, KEC-651,2020-21, Even SemPiyushNo ratings yet
- Noise Analysis and Control On Motor Starting and Accelerating of Electric BusDocument7 pagesNoise Analysis and Control On Motor Starting and Accelerating of Electric BusPhil's ChannelNo ratings yet
- Lecture 9 EEDocument14 pagesLecture 9 EESwati SharmaNo ratings yet
- Modeling of Definite Time Over-Current Relay With Auto Re-Closer Using MATLABDocument5 pagesModeling of Definite Time Over-Current Relay With Auto Re-Closer Using MATLABHayat Ansari100% (1)
- Assgmient 21 Objetives:: Single-Slope ADC ArchitectureDocument4 pagesAssgmient 21 Objetives:: Single-Slope ADC ArchitectureRodrigo TavarezNo ratings yet
- Een 202 Lab 9 ReportDocument6 pagesEen 202 Lab 9 Reportapi-296881750No ratings yet
- Shock Pulse Monitoring: ApplicationsDocument18 pagesShock Pulse Monitoring: Applicationshari krishna100% (1)
- Virtualizer 3D Fx2000: User ManualDocument28 pagesVirtualizer 3D Fx2000: User ManualTomás PGNo ratings yet
- Ebook - Electronics Explained - Transistor CircuitsDocument11 pagesEbook - Electronics Explained - Transistor CircuitsDhuvi LuvioNo ratings yet
- Physical Training of Greek-Roman Style Wrestlers (12-14 Years) by Cross Fit MeansDocument2 pagesPhysical Training of Greek-Roman Style Wrestlers (12-14 Years) by Cross Fit MeansAgache GigelNo ratings yet
- Modulation Solutions For Nematicon PropagationDocument10 pagesModulation Solutions For Nematicon PropagationIsmael ArceNo ratings yet
- Lecture 1e: Elementary Signals: Signals and Systems (Eeeb233)Document48 pagesLecture 1e: Elementary Signals: Signals and Systems (Eeeb233)Siti Nur DiniNo ratings yet
- Laboratory 2 ReportDocument40 pagesLaboratory 2 ReportRn NatNo ratings yet
- Section 3.1, Fundamental of TransmissionDocument53 pagesSection 3.1, Fundamental of Transmissionneeraj kumar singhNo ratings yet
- Applied Acoustics: Sahir Masmoudi, Abderrahim El Mahi, Saïd TurkiDocument9 pagesApplied Acoustics: Sahir Masmoudi, Abderrahim El Mahi, Saïd TurkiWilliams Marcel Caceres FerreiraNo ratings yet
- BEE MCQ Unit IIIDocument10 pagesBEE MCQ Unit IIIUmesh PatilNo ratings yet
- A Precision, Low-Cost Vibrating Sample MagnetometerDocument11 pagesA Precision, Low-Cost Vibrating Sample Magnetometervleventv100% (1)
- R Rec BT.656 5 200712 I!!pdf eDocument16 pagesR Rec BT.656 5 200712 I!!pdf eRenzo SattiNo ratings yet