You might also like
- The Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesFrom EverandThe Perfect Ic Diet Cookbook The Complete Nutrition Guide To Healing Chronic Pelvic Pain And Managing Symptoms Of Interstitial Cystitis With Delectable And Nourishing RecipesNo ratings yet
- Female Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionFrom EverandFemale Arousal and Orgasm: Anatomy, Physiology, Behaviour and EvolutionNo ratings yet
- Almitrine Bismesylate Drug OverviewDocument6 pagesAlmitrine Bismesylate Drug OverviewjeremyescaraNo ratings yet
- UI-Pharmacothrapy Handbook 11th Edition 2021Document8 pagesUI-Pharmacothrapy Handbook 11th Edition 2021pbs4yvxjndNo ratings yet
- Risk Factors and Complications of Acute PancreatitisDocument2 pagesRisk Factors and Complications of Acute Pancreatitissalome carpioNo ratings yet
- Treating Overactive Bladder NaturallyDocument53 pagesTreating Overactive Bladder NaturallyTô Hoàng DũngNo ratings yet
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument1 pageNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar Izzo100% (1)
- Inkontinensia Urin: Dr. Adhi Permana, SPPDDocument35 pagesInkontinensia Urin: Dr. Adhi Permana, SPPDTiara KhairinaNo ratings yet
- Cefuroxime and Tramadol Nursing ResponsibilitiesDocument3 pagesCefuroxime and Tramadol Nursing ResponsibilitiesElle RosalesNo ratings yet
- Nursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationDocument1 pageNursing Responsibilities Adverse Effect Indication / Contraindication Mechanism of Action Drug Name IndicationOmar IzzoNo ratings yet
- Ketorolac DRUG STUDYDocument3 pagesKetorolac DRUG STUDYA.No ratings yet
- 7 Drug StudyDocument8 pages7 Drug Studyjannaelemento11No ratings yet
- DD Billous VomittingDocument2 pagesDD Billous VomittingdewiswahyuNo ratings yet
- Asfixia perinatal, compendiumDocument7 pagesAsfixia perinatal, compendiumClaudia LópezNo ratings yet
- Generic Name: Dosage: Capsule:250 MG, 500 MG ROUTE: Oral Frequency: 250-1000 MG Every 6 Hours Maximum:4g/ DayDocument3 pagesGeneric Name: Dosage: Capsule:250 MG, 500 MG ROUTE: Oral Frequency: 250-1000 MG Every 6 Hours Maximum:4g/ DayNicole Anne TungolNo ratings yet
- Types of Urinary IncontinenceDocument1 pageTypes of Urinary Incontinencehrg79qzwc2No ratings yet
- Urinary IncontinenceDocument14 pagesUrinary Incontinencehussain AltaherNo ratings yet
- Cancer 2Document8 pagesCancer 2Viktoria Leeahna LehNo ratings yet
- University of Saint Louis: Tuguegarao City, Cagayan 3500Document4 pagesUniversity of Saint Louis: Tuguegarao City, Cagayan 3500JM RomiasNo ratings yet
- Lower GI Bleeding Case StudyDocument14 pagesLower GI Bleeding Case StudyKevin Cloyd BragasNo ratings yet
- DEFINITION-Intussusception-is-a-serious-condition-that-occurs-when-a-portion-of-the-intestine-invaginates-or-telescopes-into-an-adjacent-segment-of-the-intestine-causing-obstruction-ischemia-anDocument13 pagesDEFINITION-Intussusception-is-a-serious-condition-that-occurs-when-a-portion-of-the-intestine-invaginates-or-telescopes-into-an-adjacent-segment-of-the-intestine-causing-obstruction-ischemia-anwydiake3No ratings yet
- Urinary Tract Infection in PregnancyDocument49 pagesUrinary Tract Infection in PregnancyBALMERA, DANIELLA B.No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Planmjoie_baby6568470100% (6)
- How Is Urine Formed?: How Does The Kidney Conserve Water?Document11 pagesHow Is Urine Formed?: How Does The Kidney Conserve Water?Riik JésùsNo ratings yet
- Buscopan PDF Drugs MedicineDocument1 pageBuscopan PDF Drugs MedicineRj AmarNo ratings yet
- Selectively: Inhibitors Inhibit Serotonin Reuptake and Elicit An Antidepressan T ResponseDocument2 pagesSelectively: Inhibitors Inhibit Serotonin Reuptake and Elicit An Antidepressan T ResponseDanii LuvNo ratings yet
- Small Bowel Obstruction System - DisorderDocument1 pageSmall Bowel Obstruction System - DisorderMarina Wasem Netzlaff0% (1)
- Drug Study Cefazolin Module 13Document1 pageDrug Study Cefazolin Module 13Daryl Joy Cortez100% (1)
- Midwifery Pharmacologic Notes: Generic Name: OxytocinDocument1 pageMidwifery Pharmacologic Notes: Generic Name: OxytocinYsabelle De GuzmanNo ratings yet
- Drug StudyDocument7 pagesDrug StudyEvangeline Anne MacanasNo ratings yet
- Generic Name (Brand Name) Methergine (Methylergonovine Maleate)Document3 pagesGeneric Name (Brand Name) Methergine (Methylergonovine Maleate)jennix_030883% (6)
- Intussusception Group 4Document47 pagesIntussusception Group 4Robert DomingoNo ratings yet
- Chapter 82 Urinary IncontinenceDocument8 pagesChapter 82 Urinary IncontinenceNaronana AliNo ratings yet
- NCP FinalDocument6 pagesNCP FinalWanwan PraybeytNo ratings yet
- Drug Study NSD.Document11 pagesDrug Study NSD.Aleanne Lucero Dela Torre100% (1)
- Modul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaDocument22 pagesModul 4 Urin Incontinence: Group 14 Problem Base Learning Medical Faculty Muslim University of IndonesiaYhaya 'Dzulhijjahyanti'No ratings yet
- OxytocinDocument1 pageOxytocinjangomanaloNo ratings yet
- Assessment Planning Intervention Rationale Evaluation Urinary InconsistencyDocument1 pageAssessment Planning Intervention Rationale Evaluation Urinary InconsistencyCharles PonceNo ratings yet
- DR Drug StudyDocument6 pagesDR Drug Studyslashmortred100% (5)
- Drug Study LeukemiaDocument12 pagesDrug Study LeukemiaLiana CervantesNo ratings yet
- Bladder Dysfunction Causes and Management OptionsDocument76 pagesBladder Dysfunction Causes and Management OptionsakuphysioNo ratings yet
- Drug StudyDocument14 pagesDrug Studysyd1975% (8)
- Neurogenic Bladder UrethritisDocument2 pagesNeurogenic Bladder UrethritisOlivia LowellNo ratings yet
- Oxytocin Drug Study for Labor Augmentation and Postpartum BleedingDocument3 pagesOxytocin Drug Study for Labor Augmentation and Postpartum BleedingJustin AncogNo ratings yet
- Generic/Trade Name Drug Class Drug Action Side Effects Routes of Administration and Time (If IV) Why Would A Patient Need This Drug?Document7 pagesGeneric/Trade Name Drug Class Drug Action Side Effects Routes of Administration and Time (If IV) Why Would A Patient Need This Drug?Sraddha PatelNo ratings yet
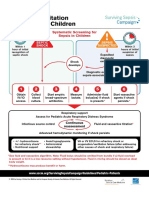
- Initial Resuscitation Algorithm For Children - Pdf.aspxDocument2 pagesInitial Resuscitation Algorithm For Children - Pdf.aspxasniatkoNo ratings yet
- INC URI: Ontinen TIA NEDocument11 pagesINC URI: Ontinen TIA NEsagaNo ratings yet
- Drug Study (Oxytocin & HNBB)Document6 pagesDrug Study (Oxytocin & HNBB)NE TdrNo ratings yet
- Pathophysiology - UtiDocument2 pagesPathophysiology - UtiAyessa Marie BarbosaNo ratings yet
- Drug Study 1st HalfDocument4 pagesDrug Study 1st HalfHanna SeNo ratings yet
- NCP GbsDocument2 pagesNCP GbsJaylord VerazonNo ratings yet
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- The Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;From EverandThe Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;No ratings yet
- Anesthesia: A Topical Update – Thoracic, Cardiac, Neuro, ICU, and Interesting CasesFrom EverandAnesthesia: A Topical Update – Thoracic, Cardiac, Neuro, ICU, and Interesting CasesRating: 5 out of 5 stars5/5 (1)
- Advances in Metabolic Disorders: Volume 3From EverandAdvances in Metabolic Disorders: Volume 3Rachmiel LevineNo ratings yet
- Contents of Powerpoint PresentationDocument2 pagesContents of Powerpoint PresentationJane Mae JesoroNo ratings yet
- Jesoro, Jane Mae P. 2BSN2 This is 64 years old right-handed dominant Caucasian female who presents with a complaint of left shoulder pain and loss of motion. The patient states that she was involved in a motor vehiDocument2 pagesJesoro, Jane Mae P. 2BSN2 This is 64 years old right-handed dominant Caucasian female who presents with a complaint of left shoulder pain and loss of motion. The patient states that she was involved in a motor vehiJane Mae JesoroNo ratings yet
- Sids DoxDocument9 pagesSids DoxJane Mae JesoroNo ratings yet
- Sids DoxDocument9 pagesSids DoxJane Mae JesoroNo ratings yet
- Transcultural Health TranscriptDocument4 pagesTranscultural Health TranscriptJane Mae JesoroNo ratings yet
- Quiz - Transcultural HealthDocument3 pagesQuiz - Transcultural HealthJane Mae JesoroNo ratings yet
- Personality Disorders 1Document20 pagesPersonality Disorders 1Jane Mae JesoroNo ratings yet
- Clinical instructors rate nursing students' skillsDocument2 pagesClinical instructors rate nursing students' skillsJane Mae JesoroNo ratings yet
- Template NCM 113 RLE - Post Activity ReportDocument4 pagesTemplate NCM 113 RLE - Post Activity ReportJane Mae JesoroNo ratings yet
- Cerebral PalsyDocument2 pagesCerebral PalsyJane Mae JesoroNo ratings yet
- Clinical instructors rate nursing students' skillsDocument2 pagesClinical instructors rate nursing students' skillsJane Mae JesoroNo ratings yet
- Cleft LipDocument2 pagesCleft LipJane Mae JesoroNo ratings yet
- Hydrocephalus: A Case StudyDocument19 pagesHydrocephalus: A Case StudyJane Mae JesoroNo ratings yet
- Ischialgia Case Report by GaluhDocument22 pagesIschialgia Case Report by GaluhDwi Ulfa AnnisaNo ratings yet
- (Grade 9) MAPEH (Health) - Drugs (2nd)Document3 pages(Grade 9) MAPEH (Health) - Drugs (2nd)KenNo ratings yet
- Nursing Care Plan - Constipation (Antepartum)Document2 pagesNursing Care Plan - Constipation (Antepartum)kaimimiyaNo ratings yet
- Ear Disorder Multiple Choice Questions-RationaleDocument5 pagesEar Disorder Multiple Choice Questions-Rationalemydewyboy83% (6)
- EBPG European Best Practice Guidelines on Haemodialysis Part 2Document43 pagesEBPG European Best Practice Guidelines on Haemodialysis Part 2Владимир Ильич ЛенинNo ratings yet
- Medical AbbreviationDocument13 pagesMedical AbbreviationRaf Luis100% (1)
- Diff Diag PDFDocument16 pagesDiff Diag PDFDana Ysabelle IbarraNo ratings yet
- Supraglottic Airway Devices A Review in A New Era of Airway Management 2155 6148 1000647Document9 pagesSupraglottic Airway Devices A Review in A New Era of Airway Management 2155 6148 1000647Riris SihotangNo ratings yet
- NCP4Document4 pagesNCP4Noreen GyleNo ratings yet
- Ice TherapyDocument5 pagesIce TherapyDiane CastillonNo ratings yet
- 22 - Disease Biology PDFDocument28 pages22 - Disease Biology PDFashutosh samalNo ratings yet
- Lymphoma NPRDocument5 pagesLymphoma NPRHavier EsparagueraNo ratings yet
- Unit 3 Part 2 Rheumatoid ArthritisDocument10 pagesUnit 3 Part 2 Rheumatoid ArthritisReman AlingasaNo ratings yet
- Cleaning of OtDocument7 pagesCleaning of Otvinod balajiNo ratings yet
- Assessment 011 1Document12 pagesAssessment 011 1ManawNo ratings yet
- Convulsive Disorders: Presenters: Kabwe Chanda EliasDocument30 pagesConvulsive Disorders: Presenters: Kabwe Chanda EliasHomeground entertainmentNo ratings yet
- Doctors Missed Call ReportDocument18 pagesDoctors Missed Call ReportVijaykumar MankaniNo ratings yet
- Jose RDocument17 pagesJose RMineTagraNo ratings yet
- HERBOLOGY-WPS OfficeDocument110 pagesHERBOLOGY-WPS OfficeVijay KumarNo ratings yet
- Recommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of PediatricsDocument2 pagesRecommendations For Preventive Pediatric Health Care: Bright Futures/American Academy of Pediatricsdidit21No ratings yet
- Prostate Biopsy - UpToDateDocument47 pagesProstate Biopsy - UpToDateCésar Aguirre RomeroNo ratings yet
- 3.guía CLSI Documento H3 - A6Document56 pages3.guía CLSI Documento H3 - A6Majo Tovar67% (3)
- Early clinical exposure in the Neonatology unitDocument17 pagesEarly clinical exposure in the Neonatology unitPentolNo ratings yet
- Neoplasia (Part 1)Document30 pagesNeoplasia (Part 1)يوسف الفيتوريNo ratings yet
- Plasmodium Parasite Life Cycle and SpeciesDocument36 pagesPlasmodium Parasite Life Cycle and SpeciesHibaaq AxmedNo ratings yet
- Rated Review ExamplesDocument41 pagesRated Review ExamplesMaria AspriNo ratings yet
- The Five Commandments of Infectious Disease ControlDocument2 pagesThe Five Commandments of Infectious Disease ControlCarol ReedNo ratings yet
- The rate of infusion is 15 mL/hrDocument48 pagesThe rate of infusion is 15 mL/hrUnihealth Southwoods NursingNo ratings yet
- Monthlyshot December 1Document10 pagesMonthlyshot December 1api-308247685No ratings yet
- Adam VitalDocument5 pagesAdam VitalAdam Vital HospitalNo ratings yet