You might also like
- Kinetik LengkapDocument133 pagesKinetik Lengkapreczky HasanNo ratings yet
- 02. Individualisasi DosisDocument30 pages02. Individualisasi DosisSoshi DaysNo ratings yet
- 2.1 Pharmacokinetics Distribution and MetabolismDocument4 pages2.1 Pharmacokinetics Distribution and MetabolismLloyd Selorio ArboledaNo ratings yet
- Pharmacology Block 1.4 - PharmacokineticsDocument9 pagesPharmacology Block 1.4 - Pharmacokineticsdaleng subNo ratings yet
- introduction (1) (1)Document56 pagesintroduction (1) (1)samrawitmekonnen16No ratings yet
- Biomedical Nanotechnology: Lecture 17: Nanopharmacology & Drug TargetingDocument65 pagesBiomedical Nanotechnology: Lecture 17: Nanopharmacology & Drug TargetingDURGA DEVI T 037 BMENo ratings yet
- Pharma Chapter 5 PDFDocument60 pagesPharma Chapter 5 PDF爾雅雷No ratings yet
- Lec1 - Introduction To Pharmacology - 1Document38 pagesLec1 - Introduction To Pharmacology - 1ABDALRHMAN ABU ZAIDNo ratings yet
- Pharmacokinetics InformationDocument31 pagesPharmacokinetics InformationSyeda Ayesha FarhanaNo ratings yet
- 1 General PharmacologyDocument29 pages1 General PharmacologyAli EllaffiNo ratings yet
- Onset VS, Duration of Action Onset: The Time Required For The Drug Before A Duration of Action: The Span of Time WhereDocument4 pagesOnset VS, Duration of Action Onset: The Time Required For The Drug Before A Duration of Action: The Span of Time WhereAmaetenNo ratings yet
- TDM UtsDocument285 pagesTDM Utsnabila auliaNo ratings yet
- (Medicalstudyzone - Com) Pharmacology Image BankDocument112 pages(Medicalstudyzone - Com) Pharmacology Image BanktktanvirNo ratings yet
- _ue_migdadiu1614592452789Document32 pages_ue_migdadiu1614592452789osama2010bNo ratings yet
- 1628771279-Oral MR Systems All Slides 06dec23Document69 pages1628771279-Oral MR Systems All Slides 06dec23Riya moreNo ratings yet
- Pharmacokinetic Models MultiDocument79 pagesPharmacokinetic Models Multiuday sainiNo ratings yet
- Integrated Therapy (part-1)(2)Document350 pagesIntegrated Therapy (part-1)(2)samuel mergaNo ratings yet
- Unit-3 BPDocument48 pagesUnit-3 BPShreyas ShreyuNo ratings yet
- Therapeutic Drug Monitoring GuideDocument12 pagesTherapeutic Drug Monitoring GuideSharon GabrielNo ratings yet
- Prof. Dr. Darius P. Zlotos: Drug Substance (Active Pharmaceutical Ingredient API)Document24 pagesProf. Dr. Darius P. Zlotos: Drug Substance (Active Pharmaceutical Ingredient API)Mirette AshrafNo ratings yet
- Introduction To BiopharmaceuticsDocument29 pagesIntroduction To Biopharmaceuticssameermomin133No ratings yet
- Introduction To Biopharmaceutics and PharmacokineticsDocument29 pagesIntroduction To Biopharmaceutics and PharmacokineticsNasima Begum100% (1)
- Pharmacokinetics LectureDocument3 pagesPharmacokinetics LectureChristine Annmarie TapawanNo ratings yet
- Cc2lab TDM Part1Document3 pagesCc2lab TDM Part1Krisiah Anne HernandezNo ratings yet
- Clinical - Pharmacokinetics 3rd Year BushDocument53 pagesClinical - Pharmacokinetics 3rd Year BushBaguma MichaelNo ratings yet
- Introduction and Overview: ObjectivesDocument17 pagesIntroduction and Overview: Objectivesandreani temeNo ratings yet
- Pharmacokinetics Student VersionDocument25 pagesPharmacokinetics Student VersionShuruq SanchezNo ratings yet
- Pharmacokinetic Models: Submitted To: Dr. Satyabrata BhanjaDocument85 pagesPharmacokinetic Models: Submitted To: Dr. Satyabrata BhanjaBandameedi RamuNo ratings yet
- Physicochemical Properties of The Drug Dosage Form Route of AdministrationDocument10 pagesPhysicochemical Properties of The Drug Dosage Form Route of AdministrationFfs AccsNo ratings yet
- Compartment Modelling Upto IV InfusionDocument42 pagesCompartment Modelling Upto IV Infusionuday sainiNo ratings yet
- Introduction to PharmacologyDocument59 pagesIntroduction to PharmacologyMoza AlanziNo ratings yet
- Principles of Clinical Pharmacology: Indications For Drug Therapy: Risk VersusDocument12 pagesPrinciples of Clinical Pharmacology: Indications For Drug Therapy: Risk VersusKenneth MiguelNo ratings yet
- Principles of Pharmacokinetics AbsorptionDocument10 pagesPrinciples of Pharmacokinetics AbsorptionMikmik DGNo ratings yet
- FarmakokinetikaDocument27 pagesFarmakokinetikaRanhie Pen'ned CendhirhieNo ratings yet
- PharmacologyDocument32 pagesPharmacologyHarleanne ParkNo ratings yet
- Drug Delivery SystemDocument78 pagesDrug Delivery SystemMd. Abu Bakar Siddique Tayef100% (1)
- Pharmacokinetic processes of drug absorption, distribution, metabolism and excretionDocument31 pagesPharmacokinetic processes of drug absorption, distribution, metabolism and excretionAli ElmehdawiNo ratings yet
- Bio PharmaceuticsDocument29 pagesBio Pharmaceuticsthedud123No ratings yet
- BioavailabilityDocument35 pagesBioavailabilityDr. Bharat JainNo ratings yet
- Per 1 - 4 Farmakologi UmumDocument98 pagesPer 1 - 4 Farmakologi UmumamaliahriskaikaNo ratings yet
- AbsorptionDocument84 pagesAbsorptionDr. Bharat JainNo ratings yet
- Unit 1, Part 4 Clin. PKDocument11 pagesUnit 1, Part 4 Clin. PKshammaNo ratings yet
- RUDs + PharmacokineticsDocument53 pagesRUDs + PharmacokineticsdaghameendoniaNo ratings yet
- Biopharmaceutics IntroductionDocument46 pagesBiopharmaceutics IntroductionMinal NadeemNo ratings yet
- Basic Concepts and Principles of PharmacokineticsDocument42 pagesBasic Concepts and Principles of PharmacokineticsSophia AgenyiNo ratings yet
- Anesthesia Pharmacology CompiledDocument106 pagesAnesthesia Pharmacology CompiledJovy Tan-AmodiaNo ratings yet
- 2021-8-31 PharmacokineticsDocument25 pages2021-8-31 PharmacokineticsNOT ZUXNo ratings yet
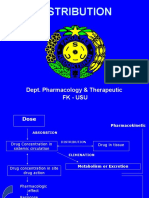
- Distribution: Dept. Pharmacology & Therapeutic FK - UsuDocument16 pagesDistribution: Dept. Pharmacology & Therapeutic FK - UsuSudirman ArbiNo ratings yet
- Concept of Drug Delivery SystemDocument60 pagesConcept of Drug Delivery SystemokNo ratings yet
- Clinical PharmacologDocument81 pagesClinical PharmacologSHILOTANo ratings yet
- 1 PHA6120 IntroductionDocument86 pages1 PHA6120 Introductionchristian redotaNo ratings yet
- Distribution: Dept. Pharmacology & Therapeutic FK - UsuDocument16 pagesDistribution: Dept. Pharmacology & Therapeutic FK - UsuagnesNo ratings yet
- Biopharmaceutics by Shehryar KhanDocument66 pagesBiopharmaceutics by Shehryar KhanAmna Saifullah100% (1)
- Cdds Unit 1.NddsDocument15 pagesCdds Unit 1.NddskblikithkumarNo ratings yet
- Adv. Biopharmaceutics All For VIvaDocument98 pagesAdv. Biopharmaceutics All For VIvaArvi KhanNo ratings yet
- Farmaco LectureDocument117 pagesFarmaco LectureanaNo ratings yet
- Pharmaco KineticsDocument427 pagesPharmaco KineticsMehrdad AvestaNo ratings yet
- Controlled Drug Delivery Systems 1.7Document35 pagesControlled Drug Delivery Systems 1.7sc5753972No ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Antihypertensive AgentsDocument1 pageAntihypertensive Agentschristian redotaNo ratings yet
- Lec1 Intro To Pharmacology PD PK FinalDocument112 pagesLec1 Intro To Pharmacology PD PK Finalchristian redotaNo ratings yet
- PHA6118 Course Orientation Portfolio 2TAY2022-23 Salonga ForRevision v3Document25 pagesPHA6118 Course Orientation Portfolio 2TAY2022-23 Salonga ForRevision v3christian redotaNo ratings yet
- 1 PHA6120 IntroductionDocument86 pages1 PHA6120 Introductionchristian redotaNo ratings yet
- (PHA6118 Lec) Introduction To PharmacologyDocument5 pages(PHA6118 Lec) Introduction To Pharmacologychristian redotaNo ratings yet
- Christian's interview on Baptist beliefsDocument1 pageChristian's interview on Baptist beliefschristian redotaNo ratings yet
- 32 Redota, Christian Activity 10Document23 pages32 Redota, Christian Activity 10christian redotaNo ratings yet
- Theology 1Document3 pagesTheology 1christian redotaNo ratings yet
- ASSIGNMENT1Document1 pageASSIGNMENT1christian redotaNo ratings yet
- 32 - Redota, Christian-Activity 3Document3 pages32 - Redota, Christian-Activity 3christian redotaNo ratings yet
- 32 Redota, Christian Activity 9Document1 page32 Redota, Christian Activity 9christian redotaNo ratings yet
- 32 Redota, Christian Acitivty 8Document1 page32 Redota, Christian Acitivty 8christian redotaNo ratings yet
- pH Measurement and Buffer Preparation LabDocument32 pagespH Measurement and Buffer Preparation Labchristian redotaNo ratings yet
- 32 Redota, Christian Activity 6Document5 pages32 Redota, Christian Activity 6christian redotaNo ratings yet
- EM Activity Flow IdentificationDocument3 pagesEM Activity Flow Identificationchristian redotaNo ratings yet
- pH Measurement and Buffer Preparation LabDocument32 pagespH Measurement and Buffer Preparation Labchristian redotaNo ratings yet
- REDOTA - Globalization Around UsDocument1 pageREDOTA - Globalization Around Uschristian redotaNo ratings yet
- Amino Acids and Peptides HoDocument17 pagesAmino Acids and Peptides Hochristian redotaNo ratings yet
- Intro HoDocument14 pagesIntro Hochristian redotaNo ratings yet
- Proteins HODocument16 pagesProteins HOchristian redotaNo ratings yet
- Suvarnaprashana Therapy in Children ConcDocument3 pagesSuvarnaprashana Therapy in Children ConcBhavana GangurdeNo ratings yet
- HSS - Summer 2020 - Syllabus - ANTH 1667Document7 pagesHSS - Summer 2020 - Syllabus - ANTH 1667Bruce JobseNo ratings yet
- Nursing Care Plan For LEUKEMIASDocument12 pagesNursing Care Plan For LEUKEMIASMaverick LimNo ratings yet
- Treating Cholestatic Liver Diseases with UDCA and BeyondDocument35 pagesTreating Cholestatic Liver Diseases with UDCA and BeyondalnyhilwanyNo ratings yet
- Heart Failure - A Life Time Pills ConsumptionDocument29 pagesHeart Failure - A Life Time Pills ConsumptionTania LadoNo ratings yet
- A Industrial Training ReportDocument23 pagesA Industrial Training ReportSuzan patelNo ratings yet
- Online Book Reviews: Stockley's Drug Interactions, Eleventh EditionDocument1 pageOnline Book Reviews: Stockley's Drug Interactions, Eleventh Editionkehie HananielNo ratings yet
- Different Routes of Nursing Medication AdministrationDocument13 pagesDifferent Routes of Nursing Medication AdministrationRonica MendozaNo ratings yet
- F3 (Gangguan Suasana Perasaan - Mood)Document41 pagesF3 (Gangguan Suasana Perasaan - Mood)Nabilla RizkyNo ratings yet
- Music For Pain Relief - Binaural Beats Instant Download PDFDocument1 pageMusic For Pain Relief - Binaural Beats Instant Download PDFIoannis ManNo ratings yet
- 1 Analgetik Ketorolac: No Golongan Obat Nama GenerikDocument44 pages1 Analgetik Ketorolac: No Golongan Obat Nama GenerikHayu Ajeng A RNo ratings yet
- Management of Refeeding Syndrome in Medical Inpatients: Clinical MedicineDocument18 pagesManagement of Refeeding Syndrome in Medical Inpatients: Clinical MedicineThay SousaNo ratings yet
- Depression Since Prozac An Argument For Authenticity 2167 1044 1000298Document8 pagesDepression Since Prozac An Argument For Authenticity 2167 1044 1000298M CNo ratings yet
- Huraira Ehsan F17-0848 Bs Accounting and Finance 7 Semester Corporate Governance Sir Shiraz Ahmed 23/1/21Document9 pagesHuraira Ehsan F17-0848 Bs Accounting and Finance 7 Semester Corporate Governance Sir Shiraz Ahmed 23/1/21huraira ehsanNo ratings yet
- Toronto Sick KidsDocument13 pagesToronto Sick KidsAnonymous AuJncFVWvNo ratings yet
- Brunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6Document1 pageBrunner and Suddarth's Textbook of Medical-Surgical Nursing 12th Ed. (Dragged) 6jamie carpioNo ratings yet
- OETreadingVol1 2Document148 pagesOETreadingVol1 2GeorgianNeagu100% (1)
- Case Study on Chronic Pain and DepressionDocument5 pagesCase Study on Chronic Pain and DepressionClinton MandelaNo ratings yet
- Trimetazidine medication guideDocument2 pagesTrimetazidine medication guideJULIANNE BAYHON100% (1)
- Algoritma Handling NyeriDocument21 pagesAlgoritma Handling Nyeriscan resepNo ratings yet
- CHAPTER V Dangerous Drugs Full PresentationDocument105 pagesCHAPTER V Dangerous Drugs Full PresentationMark Angelo BauiNo ratings yet
- 1 Sumreen Case ReportDocument4 pages1 Sumreen Case ReportNosheen JavedNo ratings yet
- PhcogRev 3 5 143Document11 pagesPhcogRev 3 5 143yermi atiNo ratings yet
- PCOL TRivias 2Document3 pagesPCOL TRivias 2Maria Izabelle QuemiNo ratings yet
- Strategi Obat BCS IIIDocument20 pagesStrategi Obat BCS IIIVennyNo ratings yet
- St. Paul College of Ilocos SurDocument5 pagesSt. Paul College of Ilocos SurKelsey MacaraigNo ratings yet
- Iontophoresis:: Iontophoresis Along With Various Drugs UsedDocument6 pagesIontophoresis:: Iontophoresis Along With Various Drugs UsedApoorvNo ratings yet
- Biologics Immunogenicity Causes and ConsequencesDocument12 pagesBiologics Immunogenicity Causes and ConsequencesWei Sheng ChongNo ratings yet
- Allergic Rhinitis VASDocument5 pagesAllergic Rhinitis VASxtineNo ratings yet
- DiclofenacDocument14 pagesDiclofenacAyunda Nur Faiz'zaNo ratings yet