You might also like
- Employee Leaves RecordDocument2 pagesEmployee Leaves RecordLizjasmine DimayaNo ratings yet
- Clerks' Mock Chart: ASMPH Year Level 8 Internal Medicine RotationDocument1 pageClerks' Mock Chart: ASMPH Year Level 8 Internal Medicine RotationMark MumarNo ratings yet
- 3.transport Allce Cert (Version 1Document1 page3.transport Allce Cert (Version 1Tushar ChaudharyNo ratings yet
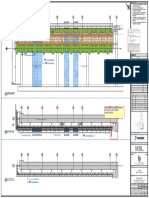
- Elevation: Tree Tree Tree TreeDocument1 pageElevation: Tree Tree Tree Treeahit1qNo ratings yet
- UNO-2.0 - 2.5-TL-OUTD-Quick Installation Guide EN-RevCDocument2 pagesUNO-2.0 - 2.5-TL-OUTD-Quick Installation Guide EN-RevCFabio Passos GuimaraesNo ratings yet
- 01 Greatness Guide WorkbookDocument114 pages01 Greatness Guide WorkbookE100% (2)
- Oral Health CardDocument2 pagesOral Health Cardgrace jay sarinasNo ratings yet
- Latur Fringe Area Dist: Latur: Sanctioned Growth Center Plan OFDocument1 pageLatur Fringe Area Dist: Latur: Sanctioned Growth Center Plan OFshaikh aslam nuroddinNo ratings yet
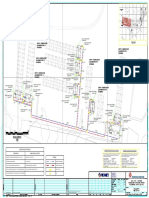
- (Scale - 1:200) Site Plan Key Plan: BLDG HT: 6.45 MT. A (Plot)Document3 pages(Scale - 1:200) Site Plan Key Plan: BLDG HT: 6.45 MT. A (Plot)ahit1qNo ratings yet
- Trial PlotDocument1 pageTrial PlotArmand Mikhail TempladoNo ratings yet
- Ea-679629 001 0000Document1 pageEa-679629 001 0000engrabbas75No ratings yet
- Ca-1231366 0002 0002Document1 pageCa-1231366 0002 0002Erfan KhanNo ratings yet
- HIRAC For Project Retubing ACHEDocument2 pagesHIRAC For Project Retubing ACHEragilNo ratings yet
- C27 Tier II Generator Set (EMCP3 and EMCP4) Electrical SystemDocument2 pagesC27 Tier II Generator Set (EMCP3 and EMCP4) Electrical SystemDaniel LopezNo ratings yet
- CTW320 Msy 00 El Abd 5002 01Document1 pageCTW320 Msy 00 El Abd 5002 01Jafffar MahasnehNo ratings yet
- Pages From PTS-21EN1004 - Final - Part 2 of 2 910-930Document21 pagesPages From PTS-21EN1004 - Final - Part 2 of 2 910-930Saim KhanNo ratings yet
- Saudia Aerospace Engineering Industries: Shop DrawingDocument1 pageSaudia Aerospace Engineering Industries: Shop Drawingmohammed luqmanNo ratings yet
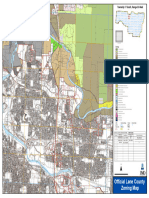
- Zoning 1703Document1 pageZoning 1703Eggs BenedictNo ratings yet
- Roald Dahl Biography QuestionsDocument1 pageRoald Dahl Biography QuestionsTornayNo ratings yet
- Smart Wealth Builder Brochure 010615Document16 pagesSmart Wealth Builder Brochure 010615VENU42908No ratings yet
- Nanded WaghalaDocument1 pageNanded Waghalavinay kumarNo ratings yet
- Seepage Area - Distance From Raja KaluveDocument1 pageSeepage Area - Distance From Raja KaluveV L HariNo ratings yet
- 2ND FLOORDocument1 page2ND FLOORShivam panditNo ratings yet
- ReadmeDocument1 pageReadmeRanto TumanggerNo ratings yet
- Masterlist Garantisadong PambataDocument1 pageMasterlist Garantisadong PambataNoli Mujar AtoleNo ratings yet
- Dma 2Document1 pageDma 2forupinkeyNo ratings yet
- L01 MBLC D05 Fad DWG 07PZ100 ZZ Ele1101 R01Document1 pageL01 MBLC D05 Fad DWG 07PZ100 ZZ Ele1101 R01Asif SafiNo ratings yet
- Diagrama c27 - 1Document2 pagesDiagrama c27 - 1Ramiro correaNo ratings yet
- Spmed Timesheet 2Document1 pageSpmed Timesheet 2api-355830788No ratings yet
- Spmed Timesheet 2Document1 pageSpmed Timesheet 2api-340778375No ratings yet
- Filed: United States District Court Western District of DwisionDocument4 pagesFiled: United States District Court Western District of DwisionEquality Case FilesNo ratings yet
- Spmed Timesheet Second SemesterDocument1 pageSpmed Timesheet Second Semesterapi-340688414No ratings yet
- Program TahfidzDocument2 pagesProgram Tahfidzanjar DevNo ratings yet
- Name of Student Average Remarks 1St Sem 2Nd Sem Gen. Ave.: Grade & Section Forsf5Document1 pageName of Student Average Remarks 1St Sem 2Nd Sem Gen. Ave.: Grade & Section Forsf5Dalope CstrNo ratings yet
- Daily Pre-Start Talk Crew MeetingDocument2 pagesDaily Pre-Start Talk Crew MeetingattaullaNo ratings yet
- A Pare Odata Pe Saftamana: G. RaneirDocument12 pagesA Pare Odata Pe Saftamana: G. RaneirvalentinpetzNo ratings yet
- MMW Form ChairMassageSignUpDocument1 pageMMW Form ChairMassageSignUpPawelNo ratings yet
- Owner Owner Consultant: BetterhomeDocument1 pageOwner Owner Consultant: BetterhomeMamado099No ratings yet
- Fatca Current AcDocument2 pagesFatca Current AcMedmacNo ratings yet
- Stren Exer Ngth/weigh Rcise HTS: Sets # Weight R Reps Wei Ight Reps Weight Reps Wei Ight RepsDocument1 pageStren Exer Ngth/weigh Rcise HTS: Sets # Weight R Reps Wei Ight Reps Weight Reps Wei Ight RepsPhong LeNo ratings yet
- Road 9.14M WIDE: 13.06 Color IndexDocument1 pageRoad 9.14M WIDE: 13.06 Color Indexmohammedjafar2508No ratings yet
- Hayagreevudu: (Children Series)Document13 pagesHayagreevudu: (Children Series)klllllllaNo ratings yet
- (Y) Manpower (Q) BD On Cartoning (N) BD On Capping (A) Bulk Unavailability (M) BD On FillingDocument1 page(Y) Manpower (Q) BD On Cartoning (N) BD On Capping (A) Bulk Unavailability (M) BD On FillingMikee FelipeNo ratings yet
- Student Convention RegistrationDocument2 pagesStudent Convention RegistrationAli NasserNo ratings yet
- DLF BHHK D B3 Z1 2001Document1 pageDLF BHHK D B3 Z1 2001praveenNo ratings yet
- Escala Grafica 1/200: TERMA 250 LTDocument1 pageEscala Grafica 1/200: TERMA 250 LTGarcía MarcoNo ratings yet
- S.F. 1164 - DibbleDocument1 pageS.F. 1164 - DibbleMN Senate Committee on Higher Education & Workforce DevelopmentNo ratings yet
- Lift Lobby 03Document1 pageLift Lobby 03PardhuRajuNo ratings yet
- Ward3 ANCSMD2023 24x36Document1 pageWard3 ANCSMD2023 24x36Nicolas DurandNo ratings yet
- 03.08.16 Karama HC Plans - Revision 1-Mezz PDFDocument1 page03.08.16 Karama HC Plans - Revision 1-Mezz PDFAshiq NishmaNo ratings yet
- Romanul - 1863 - 03 - 10Document4 pagesRomanul - 1863 - 03 - 10basharfanNo ratings yet
- 3 Top Price Action Signals PDFDocument12 pages3 Top Price Action Signals PDFhamidiNo ratings yet
- 500/2705/0 © UCLES 2015 Cambridge English Level 1 Certificate in ESOL InternationalDocument3 pages500/2705/0 © UCLES 2015 Cambridge English Level 1 Certificate in ESOL InternationalPaula Barucayo VerásteguiNo ratings yet
- MIL02 - Site 44: Datacenter Italy Caleppio Di Settala Strada Prov. 415Document1 pageMIL02 - Site 44: Datacenter Italy Caleppio Di Settala Strada Prov. 415Gino FilosaNo ratings yet
- Cambridge-English-First-2015-Sample-Paper-1-Writing v2Document3 pagesCambridge-English-First-2015-Sample-Paper-1-Writing v2Anonymous 720n5bBYKNo ratings yet
- Examen Muestra 1 Cambridge English First B2 Writing PDFDocument3 pagesExamen Muestra 1 Cambridge English First B2 Writing PDFRocio MuñozNo ratings yet
- Cambridge-English-First-2015-Sample-Paper-1-Writing v2 PDFDocument3 pagesCambridge-English-First-2015-Sample-Paper-1-Writing v2 PDFSoriaYTú0% (1)
- Cambridge-English-First-2015-Sample-Paper-1-Writing v2 PDFDocument3 pagesCambridge-English-First-2015-Sample-Paper-1-Writing v2 PDFSoriaYTúNo ratings yet
- 500/2705/0 © UCLES 2015 Cambridge English Level 1 Certificate in ESOL InternationalDocument3 pages500/2705/0 © UCLES 2015 Cambridge English Level 1 Certificate in ESOL InternationalsandraNo ratings yet
- Human Resource Title: Disinfection /fumigation Area Details: Annexure-IDocument1 pageHuman Resource Title: Disinfection /fumigation Area Details: Annexure-IGOMTINo ratings yet
- Et Antiparalytic IJNRD2202025Document13 pagesEt Antiparalytic IJNRD2202025GOMTINo ratings yet
- Human Resource Title: Rodent Control RecordDocument2 pagesHuman Resource Title: Rodent Control RecordGOMTINo ratings yet
- Employee uniform distribution log formatDocument1 pageEmployee uniform distribution log formatGOMTINo ratings yet
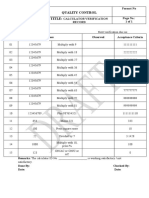
- Q - F - 008 Calculator Verification RecordDocument1 pageQ - F - 008 Calculator Verification RecordGOMTINo ratings yet
- XL Formula SheetDocument6 pagesXL Formula SheetGOMTINo ratings yet
- Power BI MCQ Quiz With Answer PDFDocument6 pagesPower BI MCQ Quiz With Answer PDFGOMTINo ratings yet
- TMVF 0 TDocument5 pagesTMVF 0 TGOMTINo ratings yet
- Excel Quiz - 40 Essential Excel QuestionsDocument35 pagesExcel Quiz - 40 Essential Excel QuestionsGOMTINo ratings yet
- Cleaning Validation MatrixDocument9 pagesCleaning Validation MatrixAbhiNo ratings yet
- Power BI Interview QuestionsDocument39 pagesPower BI Interview QuestionsGOMTINo ratings yet
- Date and time functions in DAXDocument27 pagesDate and time functions in DAXGOMTINo ratings yet
- 02 Defining Limits and Doing MACO Calculations by Pierre Devaux-1Document68 pages02 Defining Limits and Doing MACO Calculations by Pierre Devaux-1Apar Dholakia100% (1)
- 375-Article Text-1117-1-10-20180604Document7 pages375-Article Text-1117-1-10-20180604Mukesh KumarNo ratings yet
- VAL 020 Procedure For Cleaning Validation SampleDocument3 pagesVAL 020 Procedure For Cleaning Validation SampleGOMTINo ratings yet
- Cleaning Validation For The 21st Century - Acceptance Limits For APIs - Part IIDocument8 pagesCleaning Validation For The 21st Century - Acceptance Limits For APIs - Part IIdrs_mdu48No ratings yet
- Distributor AgreementDocument10 pagesDistributor Agreementsanket_hiremathNo ratings yet
- BSW, BS,,AF, BA and Metric Tool SizeDocument4 pagesBSW, BS,,AF, BA and Metric Tool SizeUNES100% (1)
- Document - University Admission SystemDocument100 pagesDocument - University Admission SystemNaresh SharmaNo ratings yet
- Career Profile: Nidhi PathakDocument4 pagesCareer Profile: Nidhi PathaknidhipathakNo ratings yet
- Rsa Netwitness Endpoint: Detect Unknown Threats. Reduce Dwell Time. Accelerate ResponseDocument8 pagesRsa Netwitness Endpoint: Detect Unknown Threats. Reduce Dwell Time. Accelerate ResponseRaghavNo ratings yet
- JBNBNBNBNBNBDocument4 pagesJBNBNBNBNBNBmaheshNo ratings yet
- Aviation Mechanic Powerplant Question Book1990Document112 pagesAviation Mechanic Powerplant Question Book1990LohnJittleNo ratings yet
- CasesDocument8 pagesCasesLinh TrịnhNo ratings yet
- Strengthening RC Structures with Steel Plate Bonding MethodsDocument29 pagesStrengthening RC Structures with Steel Plate Bonding MethodsSiti Rohani Isdris100% (1)
- Bhushan Steel LTD (BHUS IN) - Balance SheetDocument4 pagesBhushan Steel LTD (BHUS IN) - Balance SheetVamsi GunturuNo ratings yet
- Janachaitanya SouthDocument1 pageJanachaitanya SouthbharatchhayaNo ratings yet
- Drilling Products and Solutions CatalogDocument141 pagesDrilling Products and Solutions CatalogAlex Boz100% (1)
- More User Manuals OnDocument78 pagesMore User Manuals OnNicolae HincuNo ratings yet
- Develop Your Leadership SkillsDocument22 pagesDevelop Your Leadership Skillsektasharma123No ratings yet
- Athlete WaiverDocument1 pageAthlete WaiverRonan MurphyNo ratings yet
- LTE Data Analysis - Project Proposal N.2Document22 pagesLTE Data Analysis - Project Proposal N.2Syed SafwanNo ratings yet
- Updated Scar Management Practical Guidelines Non-IDocument10 pagesUpdated Scar Management Practical Guidelines Non-IChilo PrimaNo ratings yet
- PH of Fatty Quaternary Ammonium Chlorides: Standard Test Method ForDocument2 pagesPH of Fatty Quaternary Ammonium Chlorides: Standard Test Method ForAl7amdlellahNo ratings yet
- Natural Fibres For Composites in EthiopiaDocument12 pagesNatural Fibres For Composites in EthiopiaTolera AderieNo ratings yet
- Capital Harness XC LaunchDocument36 pagesCapital Harness XC LaunchnizarfebNo ratings yet
- Rate of Grease Penetration of Flexible Barrier Materials (Rapid Method)Document3 pagesRate of Grease Penetration of Flexible Barrier Materials (Rapid Method)DanZel Dan100% (1)
- The Influence of Culture Subculture On Consumer BehaviorDocument55 pagesThe Influence of Culture Subculture On Consumer Behaviorvijendra chanda100% (12)
- DRW Questions 2Document16 pagesDRW Questions 2Natasha Elena TarunadjajaNo ratings yet
- Collective Fleet Agreement TermsDocument25 pagesCollective Fleet Agreement TermskjdckncknsNo ratings yet
- Live Sound 101: Choosing Speakers and Setting Up a Sound SystemDocument14 pagesLive Sound 101: Choosing Speakers and Setting Up a Sound Systemohundper100% (1)
- Standards PoolsDocument26 pagesStandards PoolsKimMyPatZaNo ratings yet
- Coal Petroleum: Crude OilDocument25 pagesCoal Petroleum: Crude Oiljojo basenNo ratings yet
- Report of Six Months Industrial TrainingDocument38 pagesReport of Six Months Industrial TrainingJibran BashirNo ratings yet
- Re-registering a vehicle in Karnataka - A step-by-step guideDocument4 pagesRe-registering a vehicle in Karnataka - A step-by-step guideHidayathulla HasanNo ratings yet
- No or Islamic Bank OurStory EnglishDocument45 pagesNo or Islamic Bank OurStory EnglishTalib ZaidiNo ratings yet