You might also like
- 2.health AssessmentDocument7 pages2.health Assessment2BGrp3Plaza, Anna MaeNo ratings yet
- Reviewer HA LECTURE Assignments CompilationDocument5 pagesReviewer HA LECTURE Assignments CompilationAmbot sa ImoNo ratings yet
- Respiratory Assessment & DiagnosticsDocument9 pagesRespiratory Assessment & DiagnosticsAngellene GraceNo ratings yet
- Pneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsDocument34 pagesPneumonia Nursing Care Plans - 10 Nursing Diagnosis - NurseslabsMenard Velasco100% (1)
- Lesson Plan ON AppendicitisDocument14 pagesLesson Plan ON AppendicitisrevathyNo ratings yet
- Nursing Diagnosis Kel 3Document7 pagesNursing Diagnosis Kel 3Akun NyampahNo ratings yet
- Snoring, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSnoring, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- The PharynxDocument67 pagesThe PharynxArvindhanNo ratings yet
- LP DispneaDocument15 pagesLP DispneaWanda FerolitaNo ratings yet
- Respiratorydistressinthe Adultandfoal: Ashley G. BoyleDocument15 pagesRespiratorydistressinthe Adultandfoal: Ashley G. BoyleJuan Pardo CarrascoNo ratings yet
- A Modern Approach To Cough ManagementDocument4 pagesA Modern Approach To Cough ManagementSorin PalcuNo ratings yet
- Retdem Heart and Abdomen ScriptDocument2 pagesRetdem Heart and Abdomen ScriptFrancine Jane GungonNo ratings yet
- FELİNE-Upper Airway Obstruction in Cats Pathogenesis and Clinical SignsDocument7 pagesFELİNE-Upper Airway Obstruction in Cats Pathogenesis and Clinical Signstaner_soysuren100% (1)
- Medicine: CardiorespiratoryDocument56 pagesMedicine: CardiorespiratoryWalaa abo foolNo ratings yet
- Module 2 H&EDocument5 pagesModule 2 H&EHeron EgretNo ratings yet
- ملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةDocument59 pagesملزمة تمريض باطني جراحي الترم الثاني2 التميز +الريادةabdullah almatary100% (1)
- Bahaya Penyakit PolipDocument18 pagesBahaya Penyakit PolipSri Yuni HaninanaNo ratings yet
- 316 RevalidaDocument14 pages316 RevalidaPAOLA LUZ CRUZNo ratings yet
- History Notes - RespiratoryDocument17 pagesHistory Notes - Respiratoryياسر نعيم علي عبودNo ratings yet
- Jordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryDocument11 pagesJordan A. Mamalumpong Bsn-3 Clinical Instructor: Ma. Antonietta Edris Assignments For NCM 112 A. GlossaryJordan Abosama MamalumpongNo ratings yet
- Examination of The Chest and LungsDocument5 pagesExamination of The Chest and Lungsteena12aNo ratings yet
- Respiratory System: SecretionsDocument4 pagesRespiratory System: SecretionsMarian FloresNo ratings yet
- LESSON PLAN ON. Lung AbscessDocument12 pagesLESSON PLAN ON. Lung AbscessFriends ForeverNo ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Review For ENT (2008 Batch)Document9 pagesReview For ENT (2008 Batch)HaslinNo ratings yet
- Prioritized Nursing Problem For Pneumothorax Nursing Diagnosis Nursing Intervention RationaleDocument3 pagesPrioritized Nursing Problem For Pneumothorax Nursing Diagnosis Nursing Intervention RationaleJoshua VillarbaNo ratings yet
- Case Scenario 1 Pediatric-Community Acquired Pneumonia P-CapDocument19 pagesCase Scenario 1 Pediatric-Community Acquired Pneumonia P-CapJane LaquihonNo ratings yet
- Pulmonary Exam 2020Document6 pagesPulmonary Exam 2020InhoNo ratings yet
- Lungs and ThoracicDocument66 pagesLungs and ThoracicJoyce Jacobe0% (1)
- CP3 Respiratory SystemDocument23 pagesCP3 Respiratory SystemirynNo ratings yet
- Dr. N.K. Agrawal Prof, Dept. of Anaesthesiology, JNMC, SawangiDocument25 pagesDr. N.K. Agrawal Prof, Dept. of Anaesthesiology, JNMC, SawangiAmr mohammedNo ratings yet
- Dr. N.K. Agrawal Prof, Dept. of Anaesthesiology, JNMC, SawangiDocument25 pagesDr. N.K. Agrawal Prof, Dept. of Anaesthesiology, JNMC, SawangiHafid JuniorNo ratings yet
- Respiratory System - 2019Document20 pagesRespiratory System - 2019Glen Lazarus100% (1)
- Broncho PneumoniaDocument3 pagesBroncho PneumoniakathzcNo ratings yet
- Batuk Kronik BerulangDocument24 pagesBatuk Kronik BerulangHameldo Andika PattinasaranyNo ratings yet
- Case Analysis 4 GERDDocument12 pagesCase Analysis 4 GERDCJ100% (1)
- Respiratory System Assessment PDFDocument53 pagesRespiratory System Assessment PDFJay RomeNo ratings yet
- Abceso Periamigdalino AFP 2017Document6 pagesAbceso Periamigdalino AFP 2017Cin VisbeekNo ratings yet
- Respiratory Asessment Inroduction: ProcedureDocument8 pagesRespiratory Asessment Inroduction: ProcedureSREEDEVI T SURESHNo ratings yet
- Chapter 40 ReviewerDocument12 pagesChapter 40 ReviewerGracian Vel AsocsomNo ratings yet
- Cough: Group - 10Document41 pagesCough: Group - 10AradhanaRamchandaniNo ratings yet
- Respiratory Emergencies in ChildrenDocument66 pagesRespiratory Emergencies in Childrenlordoftheweb100% (7)
- Worksheet #5 Tracheostomy CareDocument3 pagesWorksheet #5 Tracheostomy CareAnonymous zVYmOxIX9SNo ratings yet
- Objectives of Physical AssessmentDocument10 pagesObjectives of Physical Assessmentemman_abz100% (1)
- Clinical SkilllllllllllllllDocument12 pagesClinical SkilllllllllllllllAlmira Putri100% (1)
- Pneumonia MikrobialDocument3 pagesPneumonia MikrobialAkun NyampahNo ratings yet
- ASSESSMENT WITH RESPIRATORY DISORDERS and DiagnosticsDocument11 pagesASSESSMENT WITH RESPIRATORY DISORDERS and DiagnosticsErika Mae Sta. MariaNo ratings yet
- Assessment Pulmonary ExamDocument3 pagesAssessment Pulmonary Examdd marshallNo ratings yet
- RTM 3Document8 pagesRTM 3Christine Danica BiteraNo ratings yet
- Pleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Jarvis Chapter 18 Study GuideDocument5 pagesJarvis Chapter 18 Study GuideEmily Cheng100% (2)
- 123group Oral Case Presentation - Medical Surgical Nursing III FINAL NA FINALDocument42 pages123group Oral Case Presentation - Medical Surgical Nursing III FINAL NA FINAL20-06115No ratings yet
- Approch To StridorDocument27 pagesApproch To Stridoraltabeb hasoon67% (3)
- Oropharyngeal DysphagiaDocument6 pagesOropharyngeal Dysphagianevelle4667No ratings yet
- Pulmo AxDocument16 pagesPulmo AxPaula Grace MorfeNo ratings yet
- SEM OutputDocument8 pagesSEM OutputJireh Vien AtienzaNo ratings yet
- AFP Clinical Nasal ObstructionDocument5 pagesAFP Clinical Nasal ObstructionTri OktarinaNo ratings yet
- Croup GuidelineDocument17 pagesCroup Guidelineromeoenny4154No ratings yet
- Lung AssessmentDocument4 pagesLung AssessmentChristel Mariz SantellaNo ratings yet
- Theories in Health EducationDocument1 pageTheories in Health EducationMary Joy EscoraNo ratings yet
- The Education ProcessDocument1 pageThe Education ProcessMary Joy EscoraNo ratings yet
- Fundamentals of Nursing PracticeDocument3 pagesFundamentals of Nursing PracticeMary Joy EscoraNo ratings yet
- Moral Decision Making (Comic Strips)Document2 pagesMoral Decision Making (Comic Strips)Mary Joy EscoraNo ratings yet
- Acute BronchitisDocument2 pagesAcute BronchitisChristabella Natalia WijayaNo ratings yet
- Oxford Mastering Science 2a Unit 7Document17 pagesOxford Mastering Science 2a Unit 7cocNo ratings yet
- Humidification in The Intensive Care UnitDocument272 pagesHumidification in The Intensive Care UnitAbu HibbaanNo ratings yet
- NursingBulletin Notes On PneumothoraxDocument27 pagesNursingBulletin Notes On Pneumothoraxseigelystic100% (11)
- Kami Export - General Review - Student Version Part I - FinalDocument8 pagesKami Export - General Review - Student Version Part I - FinalDareen FahadNo ratings yet
- Asphyxia Case StudyDocument8 pagesAsphyxia Case StudySanny Ramos100% (2)
- Acute Care Concept Map 5Document2 pagesAcute Care Concept Map 5api-380337414No ratings yet
- Test Bank For Egans Fundamentals of Respiratory Care 11th Edition by KacmarekDocument6 pagesTest Bank For Egans Fundamentals of Respiratory Care 11th Edition by Kacmarekcanebrutalfniy66No ratings yet
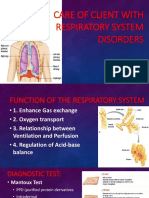
- Care of Client With Respiratory System DisordersDocument17 pagesCare of Client With Respiratory System DisordersAYTONA, JAMAICA F.No ratings yet
- Subject 1-LG-F-v2.1Document166 pagesSubject 1-LG-F-v2.1ஆர்த்தி ஆதிNo ratings yet
- Greys-Anatomy-Student (1) - CompressedDocument2 pagesGreys-Anatomy-Student (1) - CompressedKaranNo ratings yet
- Absen Pembacaan Telaah Jurnal Suci RamadhaniDocument2 pagesAbsen Pembacaan Telaah Jurnal Suci Ramadhanisuci ramadhaniNo ratings yet
- AVIAN Respiratory SystemDocument7 pagesAVIAN Respiratory Systemtaner_soysurenNo ratings yet
- Chapter 11 Biology 11Document36 pagesChapter 11 Biology 11ax1leNo ratings yet
- Tracheostomy Care: Module DescriptionDocument9 pagesTracheostomy Care: Module DescriptionRenea Joy ArruejoNo ratings yet
- Acidosis and AlkolosisDocument4 pagesAcidosis and AlkolosisDani PhilipNo ratings yet
- A2 Energy Systems and RecoveryDocument31 pagesA2 Energy Systems and RecoveryClayesmorePE0% (1)
- Week 11 Laboratory Exercise The Respiratory SystemDocument6 pagesWeek 11 Laboratory Exercise The Respiratory SystemEricka ElloNo ratings yet
- Expt7 - Something-to-Fume-About-Cigarette - (Cigarette-Smoking-and-Air-Pollution)Document7 pagesExpt7 - Something-to-Fume-About-Cigarette - (Cigarette-Smoking-and-Air-Pollution)Rex BayonaNo ratings yet
- Water CycleDocument5 pagesWater CycleJovie Ann RamiloNo ratings yet
- Arjun Chauhan (Bio)Document52 pagesArjun Chauhan (Bio)Sharad ChoudharyNo ratings yet
- Forensic MedicineDocument38 pagesForensic MedicineDominicSavioNo ratings yet
- Chronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISDocument4 pagesChronic Cough in Dogs: Published With The Permission of LAVC Close Window To Return To IVISJuanEstebanOspinaNo ratings yet
- Airway Management Recognition of Airway ObstructionDocument31 pagesAirway Management Recognition of Airway ObstructionMuhammad Hadyan RusinNo ratings yet
- Mechanical VentilationDocument16 pagesMechanical Ventilationclaire yowsNo ratings yet
- BRONCHOSDocument6 pagesBRONCHOSrajnishpathak648No ratings yet
- Respiration in Organisms - NotesDocument13 pagesRespiration in Organisms - NotesxxNo ratings yet
- Kerosene ToxicityDocument12 pagesKerosene ToxicityMohamed Abo SeifNo ratings yet
- Vaka TustimeDocument887 pagesVaka TustimeMohamed AbbasNo ratings yet
- Congenital Pulmonary Airway (Cystic Adenomatoid) Malformation - UpToDateDocument28 pagesCongenital Pulmonary Airway (Cystic Adenomatoid) Malformation - UpToDateTung PhamNo ratings yet