You might also like
- Hemant Mahanand (201941103034) Case StudyDocument50 pagesHemant Mahanand (201941103034) Case StudyHemiNo ratings yet
- ArrythmiaDocument31 pagesArrythmialubnaNo ratings yet
- Module 4 - Cardiac EmergencyDocument30 pagesModule 4 - Cardiac EmergencyElaine AntonetteNo ratings yet
- Endocrine Focus PointsDocument10 pagesEndocrine Focus PointsHayden ShulerNo ratings yet
- Careplan 4Document16 pagesCareplan 4api-653800047No ratings yet
- Persistent - Recurrent PneumoniaDocument35 pagesPersistent - Recurrent PneumoniaVishal SidanaNo ratings yet
- Persistent Vegetative StateDocument14 pagesPersistent Vegetative StateMuhammad Abdul RahmanNo ratings yet
- Draft Case Study Traumatic Brain InjuryDocument47 pagesDraft Case Study Traumatic Brain InjuryTrixia Joy R NachorNo ratings yet
- Revalida Review NotesDocument14 pagesRevalida Review NotesBryan Lloyd RayatNo ratings yet
- NCS GlaucomaDocument47 pagesNCS GlaucomaDan Floyd FernandezNo ratings yet
- نسخة اختبارDocument318 pagesنسخة اختبارSami AlanziNo ratings yet
- A Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseDocument6 pagesA Case Report - Ayurvedic Management of Pariplutayonivyapada W.S.R To Pelvic Inflammatory DiseaseIJAR JOURNALNo ratings yet
- Chapter 17. Improving The Quality of Care Through Pain Assessment and ManagementDocument30 pagesChapter 17. Improving The Quality of Care Through Pain Assessment and ManagementNur MiladiyahNo ratings yet
- Perioperative Management of Hyperglycemia and Diabetes in Cardiac Surgery PatientsDocument24 pagesPerioperative Management of Hyperglycemia and Diabetes in Cardiac Surgery PatientsRudi HaryantoNo ratings yet
- Quality of Prenatal Care Questionnaire: Instrument Development and TestingDocument17 pagesQuality of Prenatal Care Questionnaire: Instrument Development and TestingGreat CoassNo ratings yet
- Maternal and Fetal Outcomes in Patients With Previous Caesarean Section Undergoing Trial of Vaginal BirthDocument14 pagesMaternal and Fetal Outcomes in Patients With Previous Caesarean Section Undergoing Trial of Vaginal BirthIJAR JOURNALNo ratings yet
- Cellular AberrationDocument8 pagesCellular AberrationRaymund IdicaNo ratings yet
- Emailing 18-1-2019 Primary GNDocument57 pagesEmailing 18-1-2019 Primary GNSagvan HajaniNo ratings yet
- Mithsa Chanthavong at 01 - 13 - 2023 11 - 32 PMDocument4 pagesMithsa Chanthavong at 01 - 13 - 2023 11 - 32 PMschoolgirl7796100% (1)
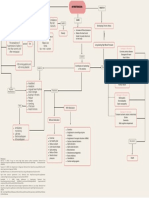
- Concept Map On HypertensionDocument1 pageConcept Map On Hypertensionleh XDNo ratings yet
- A Complete Neurological Nursing Assessment GuideDocument57 pagesA Complete Neurological Nursing Assessment GuideSarithaRajeshNo ratings yet
- Kimmulato EbrDocument2 pagesKimmulato EbrKimLawrence MulatoNo ratings yet
- Clinical Practice: Ted R. Mikuls, M.D., M.S.P.HDocument11 pagesClinical Practice: Ted R. Mikuls, M.D., M.S.P.HRichy Escobar PNo ratings yet
- Pulmonary Hypertension in The CICUDocument50 pagesPulmonary Hypertension in The CICUCardiacCareCenterMCHNo ratings yet
- ReportDocument31 pagesReportgunratna kambleNo ratings yet
- A Research Proposal HshahshDocument4 pagesA Research Proposal HshahshJaqueline Magno EmraNo ratings yet
- Diabetes OPD ดีมากกกDocument5 pagesDiabetes OPD ดีมากกกPonpimol Odee BongkeawNo ratings yet
- Final Comprehensive Case Study - Noday!Document11 pagesFinal Comprehensive Case Study - Noday!natalie nodayNo ratings yet
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniNo ratings yet
- Management Lethal ArrhythmiaDocument42 pagesManagement Lethal ArrhythmiaNovi CahyaNo ratings yet
- AbbreviationDocument90 pagesAbbreviationIrwanshah MohammadNo ratings yet
- The Effect of Obesity On Lung FunctionDocument25 pagesThe Effect of Obesity On Lung FunctionharvardboyNo ratings yet
- Arpa - 2018 0219 RaDocument6 pagesArpa - 2018 0219 Rahuseikha velayazulfahdNo ratings yet
- DiabetesDocument12 pagesDiabetessara bazanNo ratings yet
- 3 23 16 Type 1 DM Dka Group 1Document57 pages3 23 16 Type 1 DM Dka Group 1ALEXANDRA VICTORIA ANTIPORDANo ratings yet
- Strategies Tto Prevent Catheter-Associated Urinary Tract Infections in Acute Care HospitalsDocument17 pagesStrategies Tto Prevent Catheter-Associated Urinary Tract Infections in Acute Care HospitalsKiran SurageNo ratings yet
- Ebp Head Up 30Document9 pagesEbp Head Up 30La fazaNo ratings yet
- Pedia Case File PDFDocument25 pagesPedia Case File PDFSanskriti SinghNo ratings yet
- Clinical Manifestations and Treatment of Hypokalemia in AdultsDocument25 pagesClinical Manifestations and Treatment of Hypokalemia in Adultsr33realNo ratings yet
- Vital SignsDocument38 pagesVital SignsSanjna Kumari (SNSR Senior Tutor/Lecturer)100% (1)
- Electrolytes (3607)Document11 pagesElectrolytes (3607)JennNo ratings yet
- Synopsis LatestDocument23 pagesSynopsis LatestPreeti ChouhanNo ratings yet
- QweqDocument7 pagesQweqJackieNo ratings yet
- Hepatic Encephalopathy: DR Sadath HussainDocument32 pagesHepatic Encephalopathy: DR Sadath Hussain966342No ratings yet
- Mitral StenosisDocument67 pagesMitral StenosisNamithaNo ratings yet
- Cerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonDocument12 pagesCerebralamyloid Angiopathy: Laszlo Szidonya,, Joshua P. NickersonJuan Carlos LazoNo ratings yet
- PulseDocument13 pagesPulseArdi EroNo ratings yet
- 312 MidDocument60 pages312 MidVALERIANO TRISHANo ratings yet
- Prevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskDocument20 pagesPrevention of Cardiovascular Disease: Pocket Guidelines For Assessment and Management of Cardiovascular RiskCaryl Kit Balani TimtimNo ratings yet
- MS LecDocument15 pagesMS LecAngel YN Patricio FlorentinoNo ratings yet
- Surpass 1Document13 pagesSurpass 1Fernando DominguezNo ratings yet
- 1 - Neuro Assessment 2021 - 336Document30 pages1 - Neuro Assessment 2021 - 336HADI BADWAN100% (2)
- Chronic Diarrhea PDFDocument5 pagesChronic Diarrhea PDFnaryNo ratings yet
- A Systematic Review On Dementia CareDocument5 pagesA Systematic Review On Dementia CareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Va. Scd. Esc Pocket Gls. 2022. White BackgroundDocument72 pagesVa. Scd. Esc Pocket Gls. 2022. White BackgroundGeoNo ratings yet
- Cardiac RehabilitationDocument48 pagesCardiac RehabilitationsdsdNo ratings yet
- Forcadilla MedsudrugstudyDocument11 pagesForcadilla MedsudrugstudyKeir Mrls ForcadillaNo ratings yet
- Pathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCDocument42 pagesPathophysiology, Diagnosis, and Management of Dyslipidemia: Gerald T. Gau, MD, and R. Scott Wright, MD, FACC, FAHA, FESCSherleen HeiNo ratings yet
- Sudden Cardiac DeathDocument6 pagesSudden Cardiac DeathdesindahNo ratings yet
- Case Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDocument7 pagesCase Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDaniel Angelo ArangoNo ratings yet
- Daniel Angelo E. Arango BSN 2-A Group - 1 Enhanced Usapan SeriesDocument2 pagesDaniel Angelo E. Arango BSN 2-A Group - 1 Enhanced Usapan SeriesDaniel Angelo ArangoNo ratings yet
- Mortality (Global)Document3 pagesMortality (Global)Daniel Angelo ArangoNo ratings yet
- UntitledDocument1 pageUntitledDaniel Angelo ArangoNo ratings yet
- Orientations and Gender Identities in School and Promoting Reproductive Health Which IsDocument1 pageOrientations and Gender Identities in School and Promoting Reproductive Health Which IsDaniel Angelo ArangoNo ratings yet
- Bsn2-A Arango Group1 FNCP PDFDocument3 pagesBsn2-A Arango Group1 FNCP PDFDaniel Angelo ArangoNo ratings yet
- SymbolismDocument2 pagesSymbolismDaniel Angelo ArangoNo ratings yet
- Arango Lesson 1aDocument1 pageArango Lesson 1aDaniel Angelo ArangoNo ratings yet
- Jean Annette S. Ibo: Family Health Nursing ProcessDocument42 pagesJean Annette S. Ibo: Family Health Nursing ProcessDaniel Angelo ArangoNo ratings yet
- UntitledDocument1 pageUntitledDaniel Angelo ArangoNo ratings yet
- UntitledDocument1 pageUntitledDaniel Angelo ArangoNo ratings yet
- Case Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDocument7 pagesCase Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDaniel Angelo ArangoNo ratings yet
- Community Health Nursing: By: Daniel Angelo E. ArangoDocument3 pagesCommunity Health Nursing: By: Daniel Angelo E. ArangoDaniel Angelo ArangoNo ratings yet
- RUSTRIA - Gallery List of DelegationDocument1 pageRUSTRIA - Gallery List of DelegationDaniel Angelo ArangoNo ratings yet
- UntitledDocument7 pagesUntitledDaniel Angelo ArangoNo ratings yet
- BSN2A Arango LITE APPLIED-PRODUCTIVITY-TOOLSDocument2 pagesBSN2A Arango LITE APPLIED-PRODUCTIVITY-TOOLSDaniel Angelo ArangoNo ratings yet
- Daniel Angelo E. Arango BSN 2-ADocument2 pagesDaniel Angelo E. Arango BSN 2-ADaniel Angelo ArangoNo ratings yet
- Perineal Care ChecklistDocument2 pagesPerineal Care ChecklistDaniel Angelo ArangoNo ratings yet
- Leveling of Expectations StudentsDocument3 pagesLeveling of Expectations StudentsDaniel Angelo ArangoNo ratings yet
- Bsn2-A Arango Group1 FNCPDocument3 pagesBsn2-A Arango Group1 FNCPDaniel Angelo ArangoNo ratings yet
- 2A JCPArmario NCM107 Leveling of ExpectationsDocument4 pages2A JCPArmario NCM107 Leveling of ExpectationsDaniel Angelo ArangoNo ratings yet
- Arango, Daniel Angelo E. - Rcy Volunteer Application FormDocument3 pagesArango, Daniel Angelo E. - Rcy Volunteer Application FormDaniel Angelo ArangoNo ratings yet
- Case Study: Hyponatremia: Bicol University College of NursingDocument34 pagesCase Study: Hyponatremia: Bicol University College of NursingDaniel Angelo ArangoNo ratings yet
- Parents Waiver Form - DaneDocument1 pageParents Waiver Form - DaneDaniel Angelo ArangoNo ratings yet
- Why Its Important To Have Safe SexDocument3 pagesWhy Its Important To Have Safe SexDaniel Angelo ArangoNo ratings yet
- 2A EMBausa NCM107 Leveling of ExpectationsDocument3 pages2A EMBausa NCM107 Leveling of ExpectationsDaniel Angelo ArangoNo ratings yet
- Daniel Angelo E. Arango BSN2-ADocument1 pageDaniel Angelo E. Arango BSN2-ADaniel Angelo ArangoNo ratings yet
- College in Face-To-Face: Free VerseDocument1 pageCollege in Face-To-Face: Free VerseDaniel Angelo ArangoNo ratings yet
- UntitledDocument1 pageUntitledDaniel Angelo ArangoNo ratings yet
- Everyone Can Be An EntrepreneurDocument1 pageEveryone Can Be An EntrepreneurDaniel Angelo ArangoNo ratings yet
- Nursing Informatics-Reflection PaperDocument2 pagesNursing Informatics-Reflection PaperDaniel Angelo ArangoNo ratings yet
- Gynaecology 2WW Patient Information LeafletDocument3 pagesGynaecology 2WW Patient Information LeafletMusaab MouadNo ratings yet
- First Aid Kit HomeoDocument12 pagesFirst Aid Kit HomeoBelegan CrengutaNo ratings yet
- UntitledDocument16 pagesUntitledAstriUtamaNo ratings yet
- Management of Snake Bite Ulcer by Ayurvedic Formulation A Case ReportDocument5 pagesManagement of Snake Bite Ulcer by Ayurvedic Formulation A Case ReportEditor IJTSRDNo ratings yet
- Rohit Budhiraja, MD Divisions of Sleep and Circadian DisordersDocument55 pagesRohit Budhiraja, MD Divisions of Sleep and Circadian DisordersAlonso Rodriguez EscobedoNo ratings yet
- Stephen WalshDocument41 pagesStephen WalshSilviu PuiuNo ratings yet
- No. W - 00102 / IX / Date:25.04.2024. Special Bulletin-11: TH THDocument5 pagesNo. W - 00102 / IX / Date:25.04.2024. Special Bulletin-11: TH THsahidaslafkhan102No ratings yet
- 116 Shivani NairDocument20 pages116 Shivani NairShivani NairNo ratings yet
- Amlodipine - Drug StudyDocument2 pagesAmlodipine - Drug StudyAcads useNo ratings yet
- GalactosemiaDocument11 pagesGalactosemiahajiaewenlaNo ratings yet
- NCP 3rd YearDocument6 pagesNCP 3rd YearTotoro AblogNo ratings yet
- Increase in Chronic DiseasesDocument5 pagesIncrease in Chronic Diseasesxingqi yiNo ratings yet
- 200+ TOP OPHTHALMOLOGY Online Quiz Questions - Exam Test 2023Document29 pages200+ TOP OPHTHALMOLOGY Online Quiz Questions - Exam Test 2023Sharif Guddu100% (1)
- Chapter 16 Victimology: Exploring The Experience of VictimizationDocument23 pagesChapter 16 Victimology: Exploring The Experience of VictimizationBatasan Police Station100% (1)
- Quiz 1Document5 pagesQuiz 1Elle LibalibNo ratings yet
- Drug Study - Muscle Relaxant, Antiseizure & Antiparkinson'sDocument12 pagesDrug Study - Muscle Relaxant, Antiseizure & Antiparkinson'sKristineNo ratings yet
- NCM 417 - Midterm Exam 2016Document6 pagesNCM 417 - Midterm Exam 2016Mae DacerNo ratings yet
- A Case of Longitudinal Melanonychia in A Child - Benign or MalignaDocument7 pagesA Case of Longitudinal Melanonychia in A Child - Benign or MalignaMariana JuravleNo ratings yet
- Top 100 ECG CasesDocument212 pagesTop 100 ECG Casessoha.s.tumsa7No ratings yet
- ExamView - Chapter - 33 PDFDocument8 pagesExamView - Chapter - 33 PDFChizua OkoyeNo ratings yet
- Needle Stick InjuryDocument27 pagesNeedle Stick InjuryVishal ThakareNo ratings yet
- Wkqiq4fhk - Salvi Icf ModelDocument1 pageWkqiq4fhk - Salvi Icf ModelVilma Mahusay JalaliNo ratings yet
- Advanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6Document32 pagesAdvanced Cardiac Life Support (Acls) Part I: ACP 202 Module 6MoeNo ratings yet
- 2022.02.10 MCCQE Study Plan Canada 2Document52 pages2022.02.10 MCCQE Study Plan Canada 2joann15marrieNo ratings yet
- TUMORDocument13 pagesTUMORGabrielle Joyce TagalaNo ratings yet
- ACG Clinical Guideline Ulcerative Colitis In.10Document30 pagesACG Clinical Guideline Ulcerative Colitis In.10Edwin VileloNo ratings yet
- Auckland HEMS Checklist Reference 2014Document29 pagesAuckland HEMS Checklist Reference 2014Jorge JoNo ratings yet
- JBDS 11 Management of Adults With Diabetes On Dialysis Summary of Recommendations September 2022Document26 pagesJBDS 11 Management of Adults With Diabetes On Dialysis Summary of Recommendations September 2022AchrafNo ratings yet
- UntitledDocument455 pagesUntitledEmier Zulhilmi100% (2)
- ASCOT Hypertension StudyDocument12 pagesASCOT Hypertension StudyAnonymous NeRC5JYiSNo ratings yet