You might also like
- This Study Resource Was: Worksheet CDocument7 pagesThis Study Resource Was: Worksheet CBetty CooperNo ratings yet
- CNS Special Sense, ReproDocument52 pagesCNS Special Sense, ReproihavetallbrainsNo ratings yet
- Coordination of Movement-Lecture Notes 20201Document47 pagesCoordination of Movement-Lecture Notes 20201Zobayer AhmedNo ratings yet
- Motor Control IIDocument39 pagesMotor Control IILuis Eduardo RibeiroNo ratings yet
- Motor System22 018Document66 pagesMotor System22 018Prasad HewawasamNo ratings yet
- Basal Ganglia: Dr. Mohamed AlzainDocument53 pagesBasal Ganglia: Dr. Mohamed AlzainAva EbsNo ratings yet
- Nesc 2471-Dec 1Document7 pagesNesc 2471-Dec 1kamalleryNo ratings yet
- Basal GangliaDocument38 pagesBasal GangliaKhalid AlhemyariNo ratings yet
- Disorders of The Motor System 2Document22 pagesDisorders of The Motor System 2Adel AliNo ratings yet
- Nervous System - All NotesDocument6 pagesNervous System - All NotesJNo ratings yet
- Motor System FinalDocument79 pagesMotor System FinalNdor BariboloNo ratings yet
- Control of Posture & Movement-Blok15Document36 pagesControl of Posture & Movement-Blok15BonitavanyNo ratings yet
- Motor Functions of Spinal CordDocument43 pagesMotor Functions of Spinal CordEugeniu CoretchiNo ratings yet
- 2.update Sensorik-Motorik NeuropsikiatriDocument56 pages2.update Sensorik-Motorik NeuropsikiatriumamitNo ratings yet
- CNS 5 Motor SystemDocument9 pagesCNS 5 Motor SystemJeff ParkNo ratings yet
- p4 Extra Pyramidal SystemDocument19 pagesp4 Extra Pyramidal SystemHomeground entertainmentNo ratings yet
- Autonomic Nervous System: Rodina Rivera-Gorospe, M.DDocument44 pagesAutonomic Nervous System: Rodina Rivera-Gorospe, M.DPogo LocoNo ratings yet
- Basal GangliaDocument6 pagesBasal Ganglia381a53c99bNo ratings yet
- Neuroana Mod4 Basal Ganglia 1Document12 pagesNeuroana Mod4 Basal Ganglia 1Danielle HayagNo ratings yet
- MED (Neuro) - NeuroanatomyDocument6 pagesMED (Neuro) - NeuroanatomyFlora XuNo ratings yet
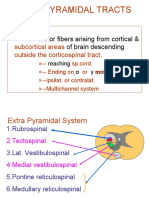
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1No ratings yet
- Ascending and Decending Tract-3Document24 pagesAscending and Decending Tract-3Lailatuz ZakiyahNo ratings yet
- Responding To The Environment HumansDocument82 pagesResponding To The Environment Humansapi-202349222No ratings yet
- Assessment of Neurologic Function - 2012Document33 pagesAssessment of Neurologic Function - 2012V_RNNo ratings yet
- Basal Ganglia Functions and Movement DisordersDocument35 pagesBasal Ganglia Functions and Movement DisordersAddison FreemanNo ratings yet
- Parkinson DiseaseDocument8 pagesParkinson DiseasedescalzotahNo ratings yet
- The Nervous SystemDocument63 pagesThe Nervous SystemLance PerezNo ratings yet
- Functional Neuroanatomy of BrainDocument50 pagesFunctional Neuroanatomy of BrainAsim ShresthaNo ratings yet
- Autonomic Pharmacology: OutlineDocument9 pagesAutonomic Pharmacology: OutlineEryll Paolo AleaNo ratings yet
- CNS DevelopmentDocument31 pagesCNS DevelopmentTaryn GoodmanNo ratings yet
- Systems Neuroscience Nov. 12, 2019Document37 pagesSystems Neuroscience Nov. 12, 2019TrajceNo ratings yet
- Motor Pathways Anatomy LecturesDocument24 pagesMotor Pathways Anatomy LecturesSindile MchunuNo ratings yet
- Motor SystemDocument49 pagesMotor SystemAhaisibwe GordonNo ratings yet
- Basal Ganglia Connections and Motor ControlDocument2 pagesBasal Ganglia Connections and Motor ControlzNo ratings yet
- Basal Ganglia: Modulation Initiation of Movements Smooth PerformanceDocument11 pagesBasal Ganglia: Modulation Initiation of Movements Smooth Performancemichaela frey purayNo ratings yet
- Motor Cortex Pyramidal ExtrapyramidalDocument22 pagesMotor Cortex Pyramidal ExtrapyramidalJOSE ARTURO LOZANO CRUZNo ratings yet
- CNS Physiology Lecture on Nervous System OrganizationDocument65 pagesCNS Physiology Lecture on Nervous System OrganizationИринаNo ratings yet
- Psyco104 Hayward Ch3 OnlineDocument51 pagesPsyco104 Hayward Ch3 OnlineyaoyingNo ratings yet
- Lesson 3 The Neuromotor Basis For Motor Control v2Document11 pagesLesson 3 The Neuromotor Basis For Motor Control v2Drift AlvinNo ratings yet
- Physiology of Motor TractsDocument34 pagesPhysiology of Motor TractsNiko MartinNo ratings yet
- Basal Ganglia Anatomy Functions Disorders (39Document10 pagesBasal Ganglia Anatomy Functions Disorders (39raph faithNo ratings yet
- Reticular Excitatory Area Controls Brain ExcitationDocument16 pagesReticular Excitatory Area Controls Brain ExcitationPutrika Juni EkasantiNo ratings yet
- Nervous, Endocrine and Reproductive Systems Test GuideDocument2 pagesNervous, Endocrine and Reproductive Systems Test GuideSean CampbellNo ratings yet
- Functions of CerebellumDocument5 pagesFunctions of CerebellumfdbhgfhgfNo ratings yet
- Neurotransmitters in The Basal GangliaDocument2 pagesNeurotransmitters in The Basal GangliazNo ratings yet
- Connections With The Brain Stem:: Neurotransmitters in The Basal GangliaDocument2 pagesConnections With The Brain Stem:: Neurotransmitters in The Basal GangliazNo ratings yet
- Physiology of Motor TractsDocument29 pagesPhysiology of Motor Tractsrj100% (1)
- Cerebellum: Location: The Term Cerebellum ObjectivesDocument34 pagesCerebellum: Location: The Term Cerebellum ObjectivesShruti ThakurNo ratings yet
- Chapter 4Document7 pagesChapter 4Neus Sangrós VidalNo ratings yet
- Sensory PathwayDocument31 pagesSensory PathwayAlma BaterinaNo ratings yet
- Neuro Exam NotesDocument31 pagesNeuro Exam NotesLizzy TaitNo ratings yet
- Autonomic Nervous System (Introduction)Document33 pagesAutonomic Nervous System (Introduction)Abdelrahman GalalNo ratings yet
- Nervous System Phisiology of Nervous Tissues. SynapsesDocument65 pagesNervous System Phisiology of Nervous Tissues. Synapsessatyagraha84No ratings yet
- Anat 6.5 Basal Ganglia - QuijanoDocument6 pagesAnat 6.5 Basal Ganglia - Quijanolovelots1234No ratings yet
- Nervous System DivisionsDocument52 pagesNervous System DivisionsJohn Toni OrtizNo ratings yet
- NeurologyDocument118 pagesNeurologykep1313No ratings yet
- Basic Concepts in Neuro-PhysiologyDocument19 pagesBasic Concepts in Neuro-Physiologymuhammad sadiqNo ratings yet
- Lesson 3 He Neuromotor Basis For Motor ControlDocument46 pagesLesson 3 He Neuromotor Basis For Motor ControlDrift AlvinNo ratings yet
- Jingying T.A. Department of PhysiologyDocument19 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Limbic SystemDocument6 pagesLimbic SystemGaby SanchezNo ratings yet
- Mind at Rest: How Neuron Structure Evolves in the Sleep Cycle.From EverandMind at Rest: How Neuron Structure Evolves in the Sleep Cycle.No ratings yet
- Physiology of Pain: DR M Madhavi LathaDocument23 pagesPhysiology of Pain: DR M Madhavi Lathanico diangeloNo ratings yet
- Physiology of Pain: DR M Madhavi LathaDocument27 pagesPhysiology of Pain: DR M Madhavi Lathanico diangeloNo ratings yet
- Carbohydrate metabolism and enzymes question bankDocument39 pagesCarbohydrate metabolism and enzymes question banknico diangeloNo ratings yet
- Endocrines 29.03.10Document3 pagesEndocrines 29.03.10nico diangeloNo ratings yet
- RespiratoryDocument2 pagesRespiratorynico diangeloNo ratings yet
- Henri Laborit and The Inhibition of ActionDocument5 pagesHenri Laborit and The Inhibition of ActionjavenacostaNo ratings yet
- Gluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDocument13 pagesGluteal Tendinopathy A Review of Mechanisms, Assessmentand ManagementDaniela Villablanca100% (1)
- Physiological Principles of SotaiDocument13 pagesPhysiological Principles of SotaiBuyu IkkanNo ratings yet
- Immunology: Overview (Moses Franklyn Dumbuya)Document69 pagesImmunology: Overview (Moses Franklyn Dumbuya)Moses DumbuyaNo ratings yet
- Care of Newborns: Understanding Vital Signs and ReflexesDocument36 pagesCare of Newborns: Understanding Vital Signs and ReflexesMA. JYRELL BONITONo ratings yet
- Basic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFDocument60 pagesBasic Clinical Laboratory Techniques 6Th Edition Estridge Solutions Manual Full Chapter PDFflorenceronaldoxo0100% (10)
- 1st MBBS From 2007 To 2018Document40 pages1st MBBS From 2007 To 2018Govindha Prem PutraNo ratings yet
- Syllabus ANP1105Document10 pagesSyllabus ANP1105Nusrat TazkiaNo ratings yet
- Intermittent FastingDocument14 pagesIntermittent FastingJéssica AssisNo ratings yet
- Lesson 2 - Muscular SystemDocument7 pagesLesson 2 - Muscular SystemCherubim GimaranganNo ratings yet
- Lecture Learning Objectives for BIO 210 SystemsDocument14 pagesLecture Learning Objectives for BIO 210 SystemsAmber DavisNo ratings yet
- Igcse Questions Placenta and Umbilical CordDocument3 pagesIgcse Questions Placenta and Umbilical CordFabriV9No ratings yet
- 01 The Living WorldDocument16 pages01 The Living Worldjocoge4337No ratings yet
- What Is General Adaptation SyndromeDocument3 pagesWhat Is General Adaptation SyndromeCARLOS, Ryan CholoNo ratings yet
- Face ExercisesDocument6 pagesFace Exercisesrima_khoury_3No ratings yet
- Poster Index Symposium 2021Document5 pagesPoster Index Symposium 2021Brien WongNo ratings yet
- Prokaryotic and Eukaryotic CellsDocument19 pagesProkaryotic and Eukaryotic CellsjhabNo ratings yet
- Lactate Dehydrogenas E: Clinical Chemistry Post-Laboratory DiscussionDocument21 pagesLactate Dehydrogenas E: Clinical Chemistry Post-Laboratory DiscussionValdez Francis ZaccheauNo ratings yet
- 1-First Aid Training Khmer & English (Basic)Document40 pages1-First Aid Training Khmer & English (Basic)Sor SethNo ratings yet
- Biochemistry of Aging TerminologiesDocument20 pagesBiochemistry of Aging TerminologiesKendrix FlorendoNo ratings yet
- (Series in Radiology 24) Raad H. Mohiaddin MD, MSC, Donald B. Longmore FRCS, FRCR (Auth.) - MRI Atlas of Normal Anatomy-Springer Netherlands (1992)Document200 pages(Series in Radiology 24) Raad H. Mohiaddin MD, MSC, Donald B. Longmore FRCS, FRCR (Auth.) - MRI Atlas of Normal Anatomy-Springer Netherlands (1992)Tina SNo ratings yet
- Accucell Diagnostic Center: Price ListDocument1 pageAccucell Diagnostic Center: Price ListAnonymous WXqKjTXMNo ratings yet
- NCM 112 (8F)Document27 pagesNCM 112 (8F)Justine April YbanezNo ratings yet
- Neuro-Oncology Explained Through Multiple Choice Questions: Joe M DasDocument243 pagesNeuro-Oncology Explained Through Multiple Choice Questions: Joe M Dasalistair90100% (1)
- 4 1Document2 pages4 1Raj BulaNo ratings yet
- BIOLOGICAL AND PSYCHOLOGICAL THEORIES OF AGINGDocument3 pagesBIOLOGICAL AND PSYCHOLOGICAL THEORIES OF AGINGLarman Keiza GaleNo ratings yet
- Invertebrates: Arthropods CharacteristicsDocument4 pagesInvertebrates: Arthropods Characteristicsfaith dicdicanNo ratings yet
- Principles of Anatomy and Physiology 15th Edition Tortora Test BankDocument52 pagesPrinciples of Anatomy and Physiology 15th Edition Tortora Test Bankgabrielvanztqro100% (29)
- Really Great School Quiz TimeDocument18 pagesReally Great School Quiz TimeKaitheryNo ratings yet