You might also like
- Business Paradigms Discovering The Future PDFDocument20 pagesBusiness Paradigms Discovering The Future PDFAndray Jamil Almakhadmeh100% (1)
- Astm A66 07 PDFDocument3 pagesAstm A66 07 PDFJavier Ricardo Romero BohorquezNo ratings yet
- 1.0 Introduction To Construction Materials and TestingDocument8 pages1.0 Introduction To Construction Materials and TestingPearl Mae AngusNo ratings yet
- ScP031 States LADocument2 pagesScP031 States LAORBeducation100% (4)
- Medical Imaging: Translating 2 Dimensional Mri Scans of the Human Forearm into 3 Dimensional Dielectric PhantomsFrom EverandMedical Imaging: Translating 2 Dimensional Mri Scans of the Human Forearm into 3 Dimensional Dielectric PhantomsNo ratings yet
- Adsorption by BhanuDocument20 pagesAdsorption by BhanuHiren vaghaniNo ratings yet
- Bet MethodDocument16 pagesBet MethodG Nivetha100% (1)
- HW - Apb - C02Document6 pagesHW - Apb - C02Ngoclinh Vo100% (1)
- Guide To Better GuardingDocument20 pagesGuide To Better GuardingLew MingNo ratings yet
- Faraday CupsDocument10 pagesFaraday CupsAshish SharmaNo ratings yet
- Jasmine2012 PDFDocument10 pagesJasmine2012 PDFmanju deviNo ratings yet
- Reconstruction, Segmentation and Smoothing of Tibia and Fibula Parts From Knee Joint Assembly and RPT Estimation and Material ConsumptionDocument5 pagesReconstruction, Segmentation and Smoothing of Tibia and Fibula Parts From Knee Joint Assembly and RPT Estimation and Material ConsumptionVishnu KalyanNo ratings yet
- J Cas 00Document10 pagesJ Cas 00Mohamed AhmedNo ratings yet
- Journal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj HowladerDocument7 pagesJournal of Oral Biology and Craniofacial Research: U. Vignesh, Divya Mehrotra, Dichen, Vaibhav Anand, Debraj Howladerlowjy119411No ratings yet
- Didier Hans, Nicole Barthe, Stephanie Boutroy, Laurent Pothuaud, Renaud Winzenrieth and Marc-Antoine KriegDocument11 pagesDidier Hans, Nicole Barthe, Stephanie Boutroy, Laurent Pothuaud, Renaud Winzenrieth and Marc-Antoine KriegkwafqjwqnyNo ratings yet
- 1 s2.0 S0889540614008634 MainDocument7 pages1 s2.0 S0889540614008634 MainPanaite TinelaNo ratings yet
- Paper M Time 2012Document5 pagesPaper M Time 2012Elizandro SordiNo ratings yet
- 2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningDocument4 pages2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningAlbert OliveraNo ratings yet
- Clinical BiomechanicsDocument7 pagesClinical BiomechanicsAngélica Luna AyalaNo ratings yet
- 2017 Article 566Document10 pages2017 Article 566abdo houamerNo ratings yet
- A Three-Dimensional Cephalometric Analysis of Japanese Adults and Its Usefulness in Orthognathic Surgery A Retrospective StudyDocument11 pagesA Three-Dimensional Cephalometric Analysis of Japanese Adults and Its Usefulness in Orthognathic Surgery A Retrospective StudyPhachara SiripraphonrojNo ratings yet
- 23 PDFDocument7 pages23 PDFPae Anusorn AmtanonNo ratings yet
- Zhang 2020Document6 pagesZhang 2020oscarNo ratings yet
- 3-Dimensional Characterization of Cortical Bone Microdamageusing OCTDocument13 pages3-Dimensional Characterization of Cortical Bone Microdamageusing OCTNareshNo ratings yet
- Assessment of Vertebral Wedge Strength Using Cancellous Textural - 2018 - JournaDocument7 pagesAssessment of Vertebral Wedge Strength Using Cancellous Textural - 2018 - JournaRyuNo ratings yet
- Tibia Model SimulationDocument9 pagesTibia Model SimulationEmon BaruaNo ratings yet
- Computerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersDocument11 pagesComputerized Medical Imaging and Graphics: Jianhua Yao, Joseph E. Burns, Hector Mu Noz, Ronald M. SummersMasithaNo ratings yet
- Manufacturing of Customized Implants For Orbital Fractures Using 3D PrintingDocument6 pagesManufacturing of Customized Implants For Orbital Fractures Using 3D PrintingManmadha CharyNo ratings yet
- Mandibular Posterior Anatomic Limit For MolarDocument8 pagesMandibular Posterior Anatomic Limit For MolarRommy MelgarejoNo ratings yet
- Paper Semana1 Opción2Document3 pagesPaper Semana1 Opción2Jharley Asencios perezNo ratings yet
- Postoperative KneeDocument15 pagesPostoperative Kneeradiology residentsNo ratings yet
- An Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointDocument7 pagesAn Approach For Three-Dimensional Visualization Using High-Resolution MRI of The Temporomandibular JointПавло БурлаковNo ratings yet
- A Finite Element Approach For Locating The Center of Resistance of Maxillary TeethDocument12 pagesA Finite Element Approach For Locating The Center of Resistance of Maxillary Teeth김재훈No ratings yet
- Interpretation of Mandibular Condyle Fractures Using 2d-And 3D-Computed TomographyDocument6 pagesInterpretation of Mandibular Condyle Fractures Using 2d-And 3D-Computed TomographyhaneefmdfNo ratings yet
- Bijcrid 20211101Document7 pagesBijcrid 20211101BOHR International Journal of Current research in Dentistry (BIJCRID)No ratings yet
- 2018 Preoperative CT-Based Three-Dimensional Templating in Robot-Assisted Total Knee Arthroplasty More Accurately Predicts Implant Sizes Than Two-Dimensional TemplatingDocument7 pages2018 Preoperative CT-Based Three-Dimensional Templating in Robot-Assisted Total Knee Arthroplasty More Accurately Predicts Implant Sizes Than Two-Dimensional Templatingsumon.huqNo ratings yet
- 14 IJAEMS-SEP-2016-11-3 Dimensional Virtual Modelling of Human Femur Bone With Prosthetic Plate and ScrewsDocument6 pages14 IJAEMS-SEP-2016-11-3 Dimensional Virtual Modelling of Human Femur Bone With Prosthetic Plate and ScrewsSyed Anas SohailNo ratings yet
- Finite Element Analysis For Prediction of BoneDocument9 pagesFinite Element Analysis For Prediction of Bonediego ricardo paez ardilaNo ratings yet
- 1 s2.0 S0010482514001413 MainDocument10 pages1 s2.0 S0010482514001413 MainFarzadNo ratings yet
- Ising 2012Document9 pagesIsing 2012leoncio cabrera rojasNo ratings yet
- Automated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BDocument6 pagesAutomated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BRyuNo ratings yet
- Computational Method To Verify Static Alignment of Transtibial ProsthesisDocument5 pagesComputational Method To Verify Static Alignment of Transtibial ProsthesisNARENDRA SAININo ratings yet
- ASME IMECE2019 CuttingGuides RevisedDocument7 pagesASME IMECE2019 CuttingGuides Revisedalexis jonathanNo ratings yet
- Accuracy of Surgical Positioning of Orthodontic Miniscrews With A Computer-Aided Design and Manufacturing TemplateDocument10 pagesAccuracy of Surgical Positioning of Orthodontic Miniscrews With A Computer-Aided Design and Manufacturing TemplateDONGXU LIUNo ratings yet
- Full-Arch Implant Surgical and Restorative Considerations: ImplantsDocument4 pagesFull-Arch Implant Surgical and Restorative Considerations: ImplantsTín ĐăngNo ratings yet
- Journal of Biomechanics: Petr Marcián, Libor Borák, Ji Ří Valášek, Jozef Kaiser, Zden Ěk Florian, Jan WolffDocument7 pagesJournal of Biomechanics: Petr Marcián, Libor Borák, Ji Ří Valášek, Jozef Kaiser, Zden Ěk Florian, Jan WolffAmrita FrancisNo ratings yet
- Esthetic Optimization of Surgical-Orthodontic TreatmentDocument22 pagesEsthetic Optimization of Surgical-Orthodontic TreatmentumadeviNo ratings yet
- Magnetic Resonance Imaging: ArticleinfoDocument10 pagesMagnetic Resonance Imaging: ArticleinfodimgloNo ratings yet
- Virtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDDocument8 pagesVirtual Surgical Planning in Craniofacial Surgery: Harvey Chim, MBBS Nicholas Wetjen, MD Samir Mardini, MDR KNo ratings yet
- Condylar Volume and Surface in Caucasian Young Adult SubjectsDocument10 pagesCondylar Volume and Surface in Caucasian Young Adult SubjectsДенис КравченкоNo ratings yet
- Implications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryDocument10 pagesImplications of 3-Dimensional Printed Spinal Implants On The Outcomes in Spine SurgeryOstazNo ratings yet
- Case Report: Mandibular Third Molar Impaction Features in CBCT 3D RadiographyDocument4 pagesCase Report: Mandibular Third Molar Impaction Features in CBCT 3D Radiographyrahmawati isnaningrumNo ratings yet
- [American Journal of Veterinary Research] Efficacy of two reduction methods in conjunction with 3-D–printed patient-specific pin guides for aligning simulated comminuted tibial fractures in cadaveric dogsDocument10 pages[American Journal of Veterinary Research] Efficacy of two reduction methods in conjunction with 3-D–printed patient-specific pin guides for aligning simulated comminuted tibial fractures in cadaveric dogsEduardo GuevaraNo ratings yet
- Changes in The Loading of Tibial Articular Cartilage Following Medial Meniscectomy: A Finite Element Analysis StudyDocument7 pagesChanges in The Loading of Tibial Articular Cartilage Following Medial Meniscectomy: A Finite Element Analysis StudylenbertiNo ratings yet
- Ijest11 03 04 182Document5 pagesIjest11 03 04 182Dattatraya ParleNo ratings yet
- Assessing The Diagnostic Precision of Cone Beam Computed Tomography (CBCT) in Temporomandibular Joint Arthritis: A Comprehensive ReviewDocument4 pagesAssessing The Diagnostic Precision of Cone Beam Computed Tomography (CBCT) in Temporomandibular Joint Arthritis: A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Setup 3DDocument8 pagesSetup 3DAlvaro ChacónNo ratings yet
- Modal Analysis of Femur Bone Using Finite Element Method For Healthcare SystemDocument5 pagesModal Analysis of Femur Bone Using Finite Element Method For Healthcare Systemimen mehriNo ratings yet
- Analysis of Correlation Between Height of Residual Ridge and Bone Density of Residual Ridge Crest at Edentulous Mandible Using Computed TomographyDocument8 pagesAnalysis of Correlation Between Height of Residual Ridge and Bone Density of Residual Ridge Crest at Edentulous Mandible Using Computed TomographydentureNo ratings yet
- Assessing The Effect of Unicondylar Knee Arthroplasty On Proximal Tibia Bone Strains Using Digital Image CorrelationDocument6 pagesAssessing The Effect of Unicondylar Knee Arthroplasty On Proximal Tibia Bone Strains Using Digital Image CorrelationAnonymous UXBSV13cNo ratings yet
- Oral and Maxillofacial Radiology: Editor: Stephen R. MattesonDocument9 pagesOral and Maxillofacial Radiology: Editor: Stephen R. MattesonLiz StephanyNo ratings yet
- Tomographic Evaluation of Infrazygomatic Crest ForDocument7 pagesTomographic Evaluation of Infrazygomatic Crest ForVishal SharmaNo ratings yet
- CJT 023Document7 pagesCJT 023Panaite TinelaNo ratings yet
- Barou 2002Document7 pagesBarou 2002Sebastián Hernán Cortés CampillayNo ratings yet
- Advanced Applications of Cone Beam Computed Tomography in OrthodonticsDocument15 pagesAdvanced Applications of Cone Beam Computed Tomography in Orthodonticsaung NaingmyoNo ratings yet
- Chang2004 2Document8 pagesChang2004 2AlfonsoNo ratings yet
- An Update in Qualitative Imaging of Bone Using Ultrashort Echo Time Magnetic ResonanceDocument12 pagesAn Update in Qualitative Imaging of Bone Using Ultrashort Echo Time Magnetic ResonanceGustavo Del PinoNo ratings yet
- 3D Imaging of Residual Limbs Using UltrasoundDocument10 pages3D Imaging of Residual Limbs Using UltrasoundVivek IyerNo ratings yet
- Stress Distribution in The Temporomandibular Joint After Mandibular Protraction: A 3-Dimensional Finite Element Method Study. Part 1Document12 pagesStress Distribution in The Temporomandibular Joint After Mandibular Protraction: A 3-Dimensional Finite Element Method Study. Part 1Sam PrasanthNo ratings yet
- Pscitech 2016 01 002Document9 pagesPscitech 2016 01 002Morteza AtaeiNo ratings yet
- 1 Saharudin2017Document18 pages1 Saharudin2017Morteza AtaeiNo ratings yet
- Astm A65 07 PDFDocument4 pagesAstm A65 07 PDFJavier Ricardo Romero BohorquezNo ratings yet
- Flexural Strength of Heat Polymerized PoDocument4 pagesFlexural Strength of Heat Polymerized PoMorteza AtaeiNo ratings yet
- Program Metric Module Involute SplinesDocument57 pagesProgram Metric Module Involute SplinesMorteza AtaeiNo ratings yet
- Rao Et Al. - 2014 - Preparation and Characterization of A Poly (Methyl Methacrylate) Based Composite Bone Cement Containing Poly (AcrylateDocument8 pagesRao Et Al. - 2014 - Preparation and Characterization of A Poly (Methyl Methacrylate) Based Composite Bone Cement Containing Poly (AcrylateMorteza AtaeiNo ratings yet
- Fracture and Fatigue Behavior of Polymer Nanocomposites-A ReviewDocument18 pagesFracture and Fatigue Behavior of Polymer Nanocomposites-A ReviewDevan1984No ratings yet
- Piezoresistive Characterization of Epoxy Based Nanocomposites Loaded With Swcnts-Dwcnts in Tensile and Fracture TestsDocument12 pagesPiezoresistive Characterization of Epoxy Based Nanocomposites Loaded With Swcnts-Dwcnts in Tensile and Fracture TestsMorteza AtaeiNo ratings yet
- 1 Saharudin2017Document18 pages1 Saharudin2017Morteza AtaeiNo ratings yet
- Materials and Design: M.R. Ayatollahi, S. Shadlou, M.M. ShokriehDocument10 pagesMaterials and Design: M.R. Ayatollahi, S. Shadlou, M.M. ShokriehMorteza AtaeiNo ratings yet
- # Experimental Procedure and Test StandardDocument6 pages# Experimental Procedure and Test StandardMorteza AtaeiNo ratings yet
- #1-Astm D5528Document13 pages#1-Astm D5528Morteza AtaeiNo ratings yet
- Flow Resistance in A Compound ChannelDocument21 pagesFlow Resistance in A Compound ChannelAhmad Mansoor MansooriNo ratings yet
- Chapter 1 - Introduction of ScienceDocument27 pagesChapter 1 - Introduction of SciencenixleonNo ratings yet
- Magnetic Contactor Over HeatingDocument7 pagesMagnetic Contactor Over HeatingReynald Shymrock UdascoNo ratings yet
- Chemical Plant Design DDocument12 pagesChemical Plant Design DFebio DalantaNo ratings yet
- Stability of Slopes: Dr. Sayed Mohamed ElarabyDocument38 pagesStability of Slopes: Dr. Sayed Mohamed ElarabyTân BùiNo ratings yet
- Department of Mathematics, Unirersity California. Berkcle-V, California 94720Document36 pagesDepartment of Mathematics, Unirersity California. Berkcle-V, California 94720Anirudh SinghNo ratings yet
- BC Series 7 - 04-05-10Document39 pagesBC Series 7 - 04-05-10Krista TranNo ratings yet
- Addressing Some Issues in Drop Weight Testing - A Material Science ApproachDocument16 pagesAddressing Some Issues in Drop Weight Testing - A Material Science ApproachManish BhadauriaNo ratings yet
- Angewandte Chemie International Edition Volume 14 Issue 11 1975 (Doi 10.1002/anie.197507451) Prof. Dr. Rudolf Criegee - Mechanism of OzonolysisDocument8 pagesAngewandte Chemie International Edition Volume 14 Issue 11 1975 (Doi 10.1002/anie.197507451) Prof. Dr. Rudolf Criegee - Mechanism of OzonolysisSubramanya ByndoorNo ratings yet
- Wenya, Li .Numerical Simulation of Friction Welding Processes Based On ABAQUS EnvironmentDocument10 pagesWenya, Li .Numerical Simulation of Friction Welding Processes Based On ABAQUS EnvironmentRadinal Fernandez SimanjuntakNo ratings yet
- E 1893 - 15Document27 pagesE 1893 - 15Eric GozzerNo ratings yet
- 2192Y / H03VVH2-F BS EN 50525-2-11 Flexible CableDocument2 pages2192Y / H03VVH2-F BS EN 50525-2-11 Flexible CableVictor Manayay ChamayaNo ratings yet
- BRAUN A5S0-Manual ENDocument20 pagesBRAUN A5S0-Manual ENSureshNo ratings yet
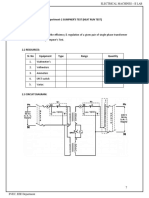
- 2.sumpner's Test On A Pair of Single Phase TransformersDocument5 pages2.sumpner's Test On A Pair of Single Phase Transformerschandrakanth100% (2)
- Soil Engineering & Geotechnics: Analysis of Potential ProblemsDocument1 pageSoil Engineering & Geotechnics: Analysis of Potential ProblemsdzingoNo ratings yet
- Literature Review: Rail Structure Interaction Analysis and Its Effect On FoundationDocument11 pagesLiterature Review: Rail Structure Interaction Analysis and Its Effect On FoundationSHRADDHA KADAMNo ratings yet
- GR 12 - Mathematics ATP - 2024Document9 pagesGR 12 - Mathematics ATP - 2024alwandeolwethu36No ratings yet
- 2.measurement CharacteristicsDocument27 pages2.measurement CharacteristicsIbtisam AbidNo ratings yet
- Sabic Diethylene Glycol: DescriptionDocument2 pagesSabic Diethylene Glycol: DescriptionAnant TyagiNo ratings yet
- BVAA Valve User Issue 13 PDFDocument88 pagesBVAA Valve User Issue 13 PDFrakacyuNo ratings yet
- RIYA Physics ProjectDocument18 pagesRIYA Physics ProjectRiya RoheraNo ratings yet
- 03 Transfer of HeatDocument34 pages03 Transfer of Heatmahsan abbasNo ratings yet


















































![[American Journal of Veterinary Research] Efficacy of two reduction methods in conjunction with 3-D–printed patient-specific pin guides for aligning simulated comminuted tibial fractures in cadaveric dogs](https://imgv2-2-f.scribdassets.com/img/document/591256390/149x198/435924092f/1710540811?v=1)