You might also like
- CARDIOVASCULAR PHYSIOLOGY LECTURE ANALYSISDocument47 pagesCARDIOVASCULAR PHYSIOLOGY LECTURE ANALYSISAndreea ŞtefănescuNo ratings yet
- Ventricular Pressure-Volume Relationship Preload, Afterload, Stroke Volume, Wall Stress & Frank-Starling's Law - ECG & ECHODocument1 pageVentricular Pressure-Volume Relationship Preload, Afterload, Stroke Volume, Wall Stress & Frank-Starling's Law - ECG & ECHOAlagusundaram LakshminarayananNo ratings yet
- K-12 Heart As A Pump - CVS-K12Document37 pagesK-12 Heart As A Pump - CVS-K12Jane Andrea Christiano DjianzonieNo ratings yet
- Cardiovascular SystemDocument50 pagesCardiovascular Systemkintan kamila100% (1)
- Cardiac Cycle: Presenter: DR Hairul Anuar Bin MahatDocument23 pagesCardiac Cycle: Presenter: DR Hairul Anuar Bin MahatHairul AnuarNo ratings yet
- DR Rahimah Zakaria Dept of PhysiologyDocument31 pagesDR Rahimah Zakaria Dept of PhysiologyChokJunHoongNo ratings yet
- Physiology (Code) - Year 2Document20 pagesPhysiology (Code) - Year 2bgj9cddvxhNo ratings yet
- Ciclul CardiacDocument1 pageCiclul CardiacAurelia AlexandraNo ratings yet
- Cardiovascular PhysiologyDocument49 pagesCardiovascular PhysiologyAndreea ŞtefănescuNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- CARDIAC CYCLE New For StudentDocument54 pagesCARDIAC CYCLE New For StudentDavi DzikirianNo ratings yet
- Study FastDocument49 pagesStudy FastmbbsporalekhaNo ratings yet
- Electrocardiogram: by H.Khorrami PH.DDocument32 pagesElectrocardiogram: by H.Khorrami PH.Dkhorrami4No ratings yet
- Cardiac Cycle: Himawan WDocument46 pagesCardiac Cycle: Himawan WaprinaNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvestoicea_katalinNo ratings yet
- Mitral ValveDocument48 pagesMitral Valvesinghal296% (23)
- Heart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument33 pagesHeart As A Pump: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraXeniel AlastairNo ratings yet
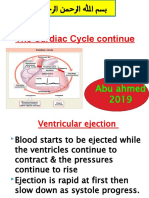
- The Cardiac Cycle Continue: Abu Ahmed 2019Document19 pagesThe Cardiac Cycle Continue: Abu Ahmed 2019Khalid AbdullahNo ratings yet
- Cardiac Cycle StagesDocument19 pagesCardiac Cycle StagesKhalid AbdullahNo ratings yet
- Rapid Ventricular Ejection Slow Ventricular EjectionDocument4 pagesRapid Ventricular Ejection Slow Ventricular EjectionKC White Dela RosaNo ratings yet
- CIE OL Bio Cardiac CycleDocument16 pagesCIE OL Bio Cardiac Cyclevqnygxb8fvNo ratings yet
- The Cardiac Cycle: - Again, This Is A Sequence of Events That Is Repeated With Each and EveryDocument4 pagesThe Cardiac Cycle: - Again, This Is A Sequence of Events That Is Repeated With Each and EveryHossam BaniisNo ratings yet
- 4,5-Cardiac Cycle Team441Document29 pages4,5-Cardiac Cycle Team441aliusman laseNo ratings yet
- CV 3 PHDocument15 pagesCV 3 PHaya najemNo ratings yet
- 8.1b. Systole-Diastole & Cardiac CycleDocument34 pages8.1b. Systole-Diastole & Cardiac Cycleverysedatedx100% (1)
- First Session-Dr - Maryam MalekiDocument49 pagesFirst Session-Dr - Maryam MalekiAamir EjazNo ratings yet
- 04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Document6 pages04-The Cardiac Cycle - Wigger's Diagram (J Swanevelder)Patrick WilliamsNo ratings yet
- 2-ch 21 - Circulatory BDocument91 pages2-ch 21 - Circulatory Blouise navorNo ratings yet
- CARDIAC CYCLE-laDocument12 pagesCARDIAC CYCLE-latehillahkabwe100No ratings yet
- The Cardiac Cycle ExplainedDocument18 pagesThe Cardiac Cycle ExplainedKundan GuptaNo ratings yet
- Cardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHDocument56 pagesCardiac Cycle: DR - Lalitha Shanmugam, Professor of Physiology, VMCHRamakrishnanNo ratings yet
- Cardiac Cycle - WikipediaDocument13 pagesCardiac Cycle - WikipediaHarshal GaikwadNo ratings yet
- Murmur and Cardiac Cycle PDFDocument17 pagesMurmur and Cardiac Cycle PDFAlesisNo ratings yet
- Cardiac Cycle: DR Rakesh JainDocument97 pagesCardiac Cycle: DR Rakesh JainKemoy FrancisNo ratings yet
- CV 2 Heart As A Pump Notes CopyrightDocument7 pagesCV 2 Heart As A Pump Notes Copyrightmaxwell amponsahNo ratings yet
- Physiology (Code) - Year 2Document20 pagesPhysiology (Code) - Year 2bgj9cddvxhNo ratings yet
- Cardiovascular System Chapter 2 SummaryDocument2 pagesCardiovascular System Chapter 2 SummaryFahmy AmyNo ratings yet
- CARDIAC CYCLE - Part I PDFDocument55 pagesCARDIAC CYCLE - Part I PDFChirag Dagar100% (1)
- Moderator: DR - Anil Verma Speaker: Rajeev: Published byDocument40 pagesModerator: DR - Anil Verma Speaker: Rajeev: Published bydaw022100% (1)
- Cardiology 2: OutlineDocument5 pagesCardiology 2: Outlinevinnie0905No ratings yet
- Cardiac EventsDocument3 pagesCardiac Eventshannahangella5949No ratings yet
- Cardiac CycleDocument30 pagesCardiac CycleAdel100% (1)
- Cardiac cycle: Mechanical events and hemodynamic changesDocument20 pagesCardiac cycle: Mechanical events and hemodynamic changesKelly Yeow100% (3)
- 8.1 Mammalian Heart and Its Regulation 2021 - 2022Document66 pages8.1 Mammalian Heart and Its Regulation 2021 - 2022Syaqir ZufazriNo ratings yet
- Cardiac Cycle Stages and Valve MovementsDocument2 pagesCardiac Cycle Stages and Valve MovementsmeandnewNo ratings yet
- Cardiac Cycle by Bala GoyalDocument14 pagesCardiac Cycle by Bala Goyaltee su lingNo ratings yet
- DR Najeeb Cardiac CycleDocument5 pagesDR Najeeb Cardiac Cycleعلي. احمد100% (1)
- Cardiovascular PhysiologyDocument287 pagesCardiovascular Physiologyarshamboss4No ratings yet
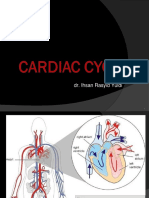
- Dr. Ihsan Rasyid Yuldi's Guide to the Cardiac CycleDocument37 pagesDr. Ihsan Rasyid Yuldi's Guide to the Cardiac CycleEltika utariNo ratings yet
- Cardiovascular Physiology: October 25, 2010Document51 pagesCardiovascular Physiology: October 25, 2010VinuPrakashJ.No ratings yet
- CARDIOVASCULAR LECTURE: TERMINOLOGY AND CIRCULATIONDocument7 pagesCARDIOVASCULAR LECTURE: TERMINOLOGY AND CIRCULATIONAnabelle RicoNo ratings yet
- Cardiac PhysioDocument9 pagesCardiac Physiosakuragi jakeNo ratings yet
- 01 - Cardiac CycleDocument4 pages01 - Cardiac CycleEhtiram HuseynovNo ratings yet
- Cardiac CycleDocument31 pagesCardiac CycleAdwaitha KrNo ratings yet
- Cardiovascular Physiology: Lawrence A. Olatunji ReaderDocument46 pagesCardiovascular Physiology: Lawrence A. Olatunji ReaderMaryam Ogunade0% (1)
- The Cardiac Cycle ExplainedDocument15 pagesThe Cardiac Cycle ExplainedNimisha BalakrishnanNo ratings yet
- The Cardiac Cycle ExplainedDocument15 pagesThe Cardiac Cycle ExplainedNimisha BalakrishnanNo ratings yet
- Anatomy 10_01_18 posteDocument19 pagesAnatomy 10_01_18 posteOlga KucinskaNo ratings yet
- Cardiac Cycle JVPDocument70 pagesCardiac Cycle JVPAstrid PramudyaaNo ratings yet
- Central Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsFrom EverandCentral Venous Pressure: Its Clinical Use and Role in Cardiovascular DynamicsNo ratings yet
- Pneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentDocument1 pagePneumatic Pruning Equipment American Arborist Supplies, Tree Care, Climbing EquipmentSalman JoNo ratings yet
- GROHE Specification Sheet 19443000-1Document2 pagesGROHE Specification Sheet 19443000-1Fred PrzNo ratings yet
- Diagrama 4 AMBIENT AIR TEMPER..Document1 pageDiagrama 4 AMBIENT AIR TEMPER..Gustavo PérezNo ratings yet
- Legend of Nueva VizcayaDocument10 pagesLegend of Nueva VizcayaAndreanna Maria100% (1)
- Hydromechanical Piercing Perforation: Oil Service Innovation TechnologiesDocument8 pagesHydromechanical Piercing Perforation: Oil Service Innovation TechnologiesЕлена ПаниотNo ratings yet
- Oxford Reading Tree: The Pet ShopDocument12 pagesOxford Reading Tree: The Pet ShopKanjaNo ratings yet
- Hearing Aid InformationDocument22 pagesHearing Aid InformationDeepakRodeyNo ratings yet
- Comparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010Document6 pagesComparative Study of Organic Solvents For Extraction of Copper From Ammoniacal Carbonate Solution Hu2010mtanaydinNo ratings yet
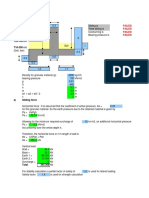
- Sliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallDocument4 pagesSliding, Overturning, Bearing Pressure and Bending Reinforcement Calculations for Retaining WallAbdul Aziz Julkarnain ZulkifliNo ratings yet
- The Future - G&VDocument6 pagesThe Future - G&VManuelHerreraMontoyaNo ratings yet
- Fair Directory 02-2016Document44 pagesFair Directory 02-2016Ravichandran SNo ratings yet
- Animal cell organelle and plant cell structure quizDocument20 pagesAnimal cell organelle and plant cell structure quizSITI ZAHILA ARYANIE BINTI ABD RAHIM KPM-GuruNo ratings yet
- Am 363 PDFDocument4 pagesAm 363 PDFsunsirNo ratings yet
- Category D Fluid ServiceDocument2 pagesCategory D Fluid Serviceaslam.ambNo ratings yet
- Manual Hoist ProductsDocument40 pagesManual Hoist Productskavin bhagavathyNo ratings yet
- Simulation of bitumen upgrading processes modelling and optimisationDocument6 pagesSimulation of bitumen upgrading processes modelling and optimisationDonato MontroneNo ratings yet
- Kyle 106 - 119 - 131 - 141Document1 pageKyle 106 - 119 - 131 - 141Gerson SouzaNo ratings yet
- HydrotherapyDocument7 pagesHydrotherapyGialys MoretaNo ratings yet
- Brochure - 2018 - Hitfact Mkii 2Document2 pagesBrochure - 2018 - Hitfact Mkii 2diaa ahmedNo ratings yet
- Liebert AC4 Controller ManualDocument88 pagesLiebert AC4 Controller ManualGreg WilliamsNo ratings yet
- Mother Teresa JerseyDocument2 pagesMother Teresa JerseyTanya van Zyl100% (1)
- Ship Construction: Second Mates - HANDOUTDocument117 pagesShip Construction: Second Mates - HANDOUTmaneeshNo ratings yet
- Model Question Paper and Solution 2022Document14 pagesModel Question Paper and Solution 2022R Y AnushNo ratings yet
- Proximity Sensing and Warning Technology For Heavy Construction Equipment OperationDocument10 pagesProximity Sensing and Warning Technology For Heavy Construction Equipment OperationAnand ReddyNo ratings yet
- Walet - Further Mathematical Methods PDFDocument79 pagesWalet - Further Mathematical Methods PDFPeter BraamsNo ratings yet
- Rate AnalysisDocument46 pagesRate AnalysisbulganinganguliNo ratings yet
- Hook and Eye-Stories Form The MarginsDocument220 pagesHook and Eye-Stories Form The MarginsJefferson LiinNo ratings yet
- Tables and Bar ChartsDocument7 pagesTables and Bar ChartsVictoria FedoseevaNo ratings yet
- The Respiratory System - Freebie GuideDocument4 pagesThe Respiratory System - Freebie GuideIndustria Quimica0% (1)
- 5020-Article Text-10917-1-10-20220808Document9 pages5020-Article Text-10917-1-10-20220808indah rumah4No ratings yet