Professional Documents
Culture Documents
NICE - UKHSA APG Summary Table Content Only - 29 June 2023
Uploaded by
Stacey WoodsOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
NICE - UKHSA APG Summary Table Content Only - 29 June 2023
Uploaded by
Stacey WoodsCopyright:
Available Formats
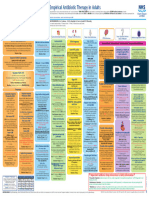
Summary of antimicrobial prescribing guidance – managing common infections
• See BNF for appropriate use and dosing in specific populations, for example, hepatic impairment, renal impairment, pregnancy and breastfeeding.
Key: Click to access doses for children Click to access NICE’s printable visual summary
Jump to section on:
Upper RTI Lower RTI UTI Meningitis GI Genital Skin Eye Dental
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Upper respiratory tract infections
Acute sore Advise paracetamol, or if preferred and suitable, First choice: 500mg QDS or 5 to 10 days*
throat ibuprofen for pain. phenoxymethylpenicillin 1000mg BD
Medicated lozenges may help pain in adults. Penicillin allergy: 250mg to 500mg 5 days
Use FeverPAIN or Centor to assess symptoms: clarithromycin OR BD
FeverPAIN 0-1 or Centor 0-2: no antibiotic; erythromycin (if macrolide 250mg to 500mg 5 days
FeverPAIN 2-3: no or back-up antibiotic; needed in pregnancy; QDS or
FeverPAIN 4-5 or Centor 3-4: immediate or consider benefit/harm)
UK Health back-up antibiotic. 500mg to 1000mg
Security BD
Agency Systemically very unwell or high risk of
complications: immediate antibiotic.
*5 days of phenoxymethylpenicillin may be
enough for symptomatic cure; but a 10-day
Last updated: course may increase the chance of
Feb 2023
microbiological cure.
For detailed information click the visual
summary icon.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 1
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Influenza
Last updated: For management guidance please refer to UKHSA guidance on Influenza: treatment and prophylaxis using anti-viral agents.
June 2023
Status: Under
review
Acute otitis Regular paracetamol or ibuprofen for pain (right First choice: amoxicillin - 5 to 7 days
media dose for age or weight at the right time and Penicillin allergy: - 5 to 7 days
maximum doses for severe pain). clarithromycin OR
Consider ear drops containing an anaesthetic erythromycin (if macrolide -
and an analgesic for pain if an immediate needed in pregnancy;
antibiotic is not given and there is no ear drum consider benefit/harm)
perforation or otorrhoea.
UK Health Second choice: co- - 5 to 7 days
Otorrhoea or under 2 years with infection in amoxiclav
Security both ears: no, back-up or immediate antibiotic.
Agency Otherwise: no or back-up antibiotic.
Systemically very unwell or high risk of
Last updated: Mar complications: immediate antibiotic.
2022
For detailed information click on the visual summary.
Acute otitis
externa For management guidance please refer to NICE/Clinical Knowledge Summaries: Otitis externa
Last updated:
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 2
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Scarlet fever
(GAS) For management guidance please refer to NICE/Clinical Knowledge Summaries: Scarlet Fever
Last updated:
June: 2023
Status: Under
review
Sinusitis Advise paracetamol or ibuprofen for pain. Little First choice: 500mg QDS
5 days
evidence that nasal saline or nasal phenoxymethylpenicillin
decongestants help, but people may want to try Penicillin allergy: 200mg on day 1,
them. doxycycline (not in under then 100mg OD
Symptoms for 10 days or less: no antibiotic. 12s) OR
Symptoms with no improvement for more clarithromycin OR 500mg BD 5 days
than 10 days: no antibiotic or back-up antibiotic erythromycin (if macrolide 250 to 500mg
UK Health depending on likelihood of bacterial cause. needed in pregnancy; QDS or
Security Consider high-dose nasal corticosteroid (if over consider benefit/harm) 500 to 1000mg BD
Agency 12 years). Second choice or first 500/125mg TDS
Systemically very unwell or high risk of choice if systemically
complications: immediate antibiotic. very unwell or high risk 5 days
Last updated:
For detailed information click on the visual summary. of complications:
Oct 2017
co-amoxiclav
Lower respiratory tract infections
COVID-19 Antibiotics should not be used for preventing or treating COVID-19 unless there is clinical suspicion of additional bacterial co-infection.
Do not use azithromycin to treat COVID-19.
Do not use doxycycline to treat COVID-19 in the community.
Do not offer an antibiotic for preventing secondary bacterial pneumonia in people with COVID-19.
Last updated: If a person in the community has suspected or confirmed secondary bacterial pneumonia, start antibiotic treatment as soon as possible, see
December 2021 community-acquired pneumonia for choices.
In hospital, start empirical antibiotics if there is clinical suspicion of a secondary bacterial infection in people with COVID-19, see hospital-acquired
pneumonia for choices. Start antibiotics as soon as possible after establishing a diagnosis of secondary bacterial pneumonia, and certainly within
4 hours. Start treatment within 1 hour if the person has suspected sepsis and meets any of the high-risk criteria for this outlined in the NICE
guideline on sepsis.
For detailed information, see the NICE guideline on managing COVID-19.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 3
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acute Many exacerbations are not caused by bacterial First choice: 500mg TDS (see
exacerbation infections so will not respond to antibiotics. amoxicillin OR BNF for severe -
of COPD Consider an antibiotic, but only after taking into infection)
account severity of symptoms (particularly doxycycline OR 200mg on day 1,
sputum colour changes and increases in volume 5 days
then 100mg OD
or thickness), need for hospitalisation, previous -
(see BNF for
exacerbations, hospitalisations and risk of severe infection)
complications, previous sputum culture and
clarithromycin 500mg BD -
susceptibility results, and risk of resistance with
repeated courses. Second choice: use alternative first choice
UK Health
Security Some people at risk of exacerbations may have Alternative choice (if 500/125mg TDS
Agency antibiotics to keep at home as part of their person at higher risk of
-
exacerbation action plan. treatment failure):
For detailed information click on the visual summary. co-amoxiclav OR
See also the NICE guideline on COPD in over 16s. co-trimoxazole OR 960mg BD -
Last updated:
levofloxacin (with 500mg OD 5 days
Dec 2018
specialist advice if co-
amoxiclav or co-
-
trimoxazole cannot be
used; consider safety
issues)
IV antibiotics (click on visual summary)
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 4
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acute Send a sputum sample for culture and First choice empirical 500mg TDS
exacerbation susceptibility testing. treatment:
of Offer an antibiotic. amoxicillin (preferred if
bronchiectasis pregnant) OR
When choosing an antibiotic, take account of 7 to 14 days
(non-cystic doxycycline (not in under 200mg on day 1,
severity of symptoms and risk of treatment
fibrosis) 12s) OR then 100mg OD
failure. People who may be at higher risk of
treatment failure include people who’ve had clarithromycin 500mg BD
repeated courses of antibiotics, a previous Alternative choice (if 500/125mg TDS
sputum culture with resistant or atypical person at higher risk of
bacteria, or a higher risk of developing treatment failure)
complications. empirical treatment:
Course length is based on severity of co-amoxiclav OR
UK Health bronchiectasis, exacerbation history, severity of
Security levofloxacin (adults only: 500mg OD or BD
exacerbation symptoms, previous culture and
Agency with specialist advice if
susceptibility results, and response to treatment. co-amoxiclav cannot be 7 to 14 days
Do not routinely offer antibiotic prophylaxis to used; consider safety
prevent exacerbations. issues) OR
Last updated: Seek specialist advice for preventing
Dec 2018 ciprofloxacin (children -
exacerbations in people with repeated acute only: with specialist advice
exacerbations. This may include a trial of if co-amoxiclav cannot be
antibiotic prophylaxis after a discussion of the used; consider safety
possible benefits and harms, and the need for issues)
regular review.
IV antibiotics (click on visual summary)
For detailed information click on the visual
When current susceptibility data available: choose antibiotics accordingly
summary.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 5
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acute cough Some people may wish to try honey (in over 1s), Adults first choice: 200mg on day 1,
the herbal medicine pelargonium (in over 12s), doxycycline then 100mg OD -
cough medicines containing the expectorant Adults alternative first 500mg TDS
guaifenesin (in over 12s) or cough medicines choices:
containing cough suppressants, except codeine, amoxicillin (preferred if -
(in over 12s). These self-care treatments have pregnant) OR
limited evidence for the relief of cough 5 days
symptoms. clarithromycin OR 250mg to 500mg
UK Health BD -
Security Acute cough with upper respiratory tract
Agency infection: no antibiotic. erythromycin (if macrolide 250mg to 500mg
needed in pregnancy; QDS or
Acute bronchitis: no routine antibiotic. consider benefit/harm) 500mg to 1000mg -
Acute cough and higher risk of BD
Last updated:
complications (at face-to-face examination):
Feb 2019 Children first choice: -
immediate or back-up antibiotic. amoxicillin
Acute cough and systemically very unwell (at
Children alternative first -
face to face examination): immediate
choices:
antibiotic.
clarithromycin OR
Higher risk of complications includes people with
erythromycin OR -
pre-existing comorbidity; young children born
prematurely; people over 65 with 2 or more of, doxycycline (not in under -
or over 80 with 1 or more of: hospitalisation in 12s)
5 days
previous year, type 1 or 2 diabetes, history of
congestive heart failure, current use of oral
corticosteroids.
Do not offer a mucolytic, an oral or inhaled
bronchodilator, or an oral or inhaled
corticosteroid unless otherwise indicated.
For detailed information click on the visual
summary.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 6
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Hospital- If symptoms or signs of pneumonia start within First choice (non-severe 500/125 mg TDS
acquired 48 hours of hospital admission, see community and not higher risk of 5 days then
pneumonia acquired pneumonia. resistance): review
Offer an antibiotic. Start treatment as soon as co-amoxiclav
possible after diagnosis, within 4 hours (within Adults alternative first 200mg on day 1,
1 hour if sepsis suspected and person meets choice (non-severe and then 100mg OD
any high risk criteria – see the NICE guideline not higher risk of
on sepsis). resistance)
UK Health
When choosing an antibiotic, take account of Choice based on specialist -
Security severity of symptoms or signs, number of days microbiological advice and
Agency in hospital before onset of symptoms, risk of local resistance data
developing complications, local hospital and Options include:
ward-based antimicrobial resistance data, recent doxycycline
Last updated: antibiotic use and microbiological results, recent 5 days then
Sept 2019
contact with a health or social care setting cefalexin (caution in 500 mg BD or TDS
review
before current admission, and risk of adverse penicillin allergy) (can increase to
1 to 1.5g TDS or -
effects with broad spectrum antibiotics.
QDS)
No validated severity assessment tools are
available. Assess severity of symptoms or signs co-trimoxazole 960mg BD -
based on clinical judgement. levofloxacin (only if 500mg OD or BD
Higher risk of resistance includes relevant switching from IV
comorbidity (such as severe lung disease or levofloxacin with specialist -
immunosuppression), recent use of broad advice; consider safety
spectrum antibiotics, colonisation with multi-drug issues)
resistant bacteria, and recent contact with health Children alternative first -
and social care settings before current choice (non-severe and
admission. not higher risk of
If symptoms or signs of pneumonia start within resistance):
days 3 to 5 of hospital admission in people not clarithromycin
Other options may be -
at higher risk of resistance, consider following
community acquired pneumonia for choice of suitable based on
antibiotic. specialist microbiological
advice and local
For detailed information click on the visual
resistance data
summary.
For first choice IV antibiotics (severe or higher risk of resistance) and
antibiotics to be added if suspected or confirmed MRSA infection see
visual summary
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 7
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Community- Assess severity in adults based on clinical First choice (low severity 500mg TDS
acquired judgement and guided by a mortality risk score in adults or non-severe (higher doses can
pneumonia (CRB65 or CURB65) when these scores can be in children): be used, see BNF)
calculated: amoxicillin
low severity – CRB65 0 or CURB65 0 or 1 Alternative first choice 200mg on day 1,
(low severity in adults or then 100mg OD
moderate severity – CRB65 1 or 2 or CURB65
non-severe in children): 5 days*
2
doxycycline (not in under
high severity – CRB65 3 or 4 or CURB65 3 to 12s) OR
5. clarithromycin OR 500mg BD
UK Health 1 point for each parameter: confusion, (urea erythromycin (if macrolide 500mg QDS
Security >7 mmol/l), respiratory rate ≥30/min, low needed in pregnancy;
Agency systolic (<90 mm Hg) or diastolic (≤60 mm Hg) consider benefit/harm)
blood pressure, age ≥65. First choice (moderate 500mg TDS
Assess severity in children based on clinical severity in adults): (higher doses can
Last updated: Sept judgement. amoxicillin be used, see BNF) -
2019
Offer an antibiotic. Start treatment as soon as AND (if atypical
possible after diagnosis, within 4 hours (within pathogens suspected)
1 hour if sepsis suspected and person meets clarithromycin OR 500mg BD -
any high risk criteria – see the NICE guideline erythromycin (if macrolide 500mg QDS
5 days*
on sepsis). needed in pregnancy; -
consider benefit/harm)
When choosing an antibiotic, take account of
Alternative first choice 200mg on day 1,
severity, risk of complications, local antimicrobial
(moderate severity in then 100mg OD
resistance and surveillance data, recent -
adults):
antibiotic use and microbiological results.
doxycycline OR
* Stop antibiotics after 5 days unless clarithromycin 500mg BD -
microbiological results suggest a longer course First choice (high 500/125mg TDS
is needed or the person is not clinically stable. severity in adults or
For detailed information click on the visual summary. severe in children):
co-amoxiclav
AND (if atypical
5 days*
pathogens suspected)
clarithromycin OR 500mg BD
erythromycin (if macrolide 500mg QDS
needed in pregnancy;
consider benefit/harm)
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 8
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Alternative first choice 500mg BD
(high severity in adults):
-
levofloxacin (consider
safety issues)
IV antibiotics (click on visual summary)
Urinary tract infections
Lower urinary Advise paracetamol or ibuprofen for pain. Non-pregnant women 100mg m/r BD (or
tract infection Non-pregnant women: back up antibiotic (to first choice: if unavailable
-
use if no improvement in 48 hours or symptoms nitrofurantoin (if eGFR 50mg QDS)
≥45 ml/minute) OR 3 days
worsen at any time) or immediate antibiotic.
Pregnant women, men, children or young trimethoprim (if low risk of 200mg BD
-
people: immediate antibiotic. resistance)
When considering antibiotics, take account of Non-pregnant women 100mg m/r BD (or
severity of symptoms, risk of complications, second choice: if unavailable
UK Health - 3 days
previous urine culture and susceptibility results, nitrofurantoin (if eGFR 50mg QDS)
Security previous antibiotic use which may have led to ≥45 ml/minute) OR
Agency resistant bacteria and local antimicrobial pivmecillinam (a penicillin) 400mg initial dose,
resistance data. - 3 days
OR then 200mg TDS
If people have symptoms of pyelonephritis (such fosfomycin 3g single dose
Last updated: as fever) or a complicated UTI, see acute - single dose
sachet
Oct 2018 pyelonephritis (upper urinary tract infection) for
Pregnant women first 100mg m/r BD (or
antibiotic choices.
choice: nitrofurantoin if unavailable
For detailed information click on the visual summary. - 7 days
(avoid at term) – if eGFR 50mg QDS)
See also the NICE guideline on urinary tract infection ≥45 ml/minute
in under 16s: diagnosis and management and the UK
Health Security Agency urinary tract infection: Pregnant women second 500mg TDS
diagnostic tools for primary care. choice: amoxicillin (only if
-
culture results available 7 days
and susceptible) OR
cefalexin 500mg BD -
Treatment of asymptomatic bacteriuria in pregnant women: choose from
nitrofurantoin (avoid at term), amoxicillin or cefalexin based on recent culture
and susceptibility results
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 9
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Men first choice: 200mg BD
-
trimethoprim OR
nitrofurantoin (if eGFR 100mg m/r BD (or 7 days
≥45 ml/minute) if unavailable -
50mg QDS)
Men second choice: consider alternative diagnoses basing antibiotic choice
on recent culture and susceptibility results
Children and young -
people (3 months and
over) first choice:
trimethoprim (if low risk of
resistance) OR
nitrofurantoin (if eGFR -
≥45 ml/minute)
Children and young -
people (3 months and -
over) second choice:
nitrofurantoin (if eGFR
≥45 ml/minute and not
used as first choice) OR
amoxicillin (only if culture -
results available and
susceptible) OR
cefalexin -
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 10
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acute Advise paracetamol (+/- low-dose weak opioid) Non-pregnant women 500mg BD or TDS
pyelonephritis for pain for people over 12. and men first choice: (up to 1g to 1.5g
- 7 to 10 days
(upper urinary Offer an antibiotic. cefalexin OR TDS or QDS for
tract) severe infections)
When prescribing antibiotics, take account of
severity of symptoms, risk of complications, co-amoxiclav (only if 500/125mg TDS
previous urine culture and susceptibility results, culture results available - 7 to 10 days
previous antibiotic use which may have led to and susceptible) OR
resistant bacteria and local antimicrobial
resistance data. trimethoprim (only if 200mg BD
Avoid antibiotics that don’t achieve adequate culture results available - 14 days
levels in renal tissue, such as nitrofurantoin. and susceptible) OR
UK Health For detailed information click on the visual summary. ciprofloxacin (consider 500mg BD
Security See also the NICE guideline on urinary tract infection - 7 days
safety issues)
Agency in under 16s: diagnosis and management and the UK
Health Security Agency urinary tract infection: Non-pregnant women and men IV antibiotics (click on visual summary)
diagnostic tools for primary care. Pregnant women first 500mg BD or TDS
choice: (up to 1g to 1.5g
Last updated: - 7 to 10 days
Oct 2018
cefalexin TDS or QDS for
severe infections)
Pregnant women second choice or IV antibiotics (click on visual summary)
Children and young -
people (3 months and
over) first choice:
cefalexin OR -
co-amoxiclav (only if -
culture results available
and susceptible)
Children and young people (3 months and over) IV antibiotics (click on
visual summary)
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 11
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acute Advise paracetamol (+/- low-dose weak opioid) First choice (guided by 500mg BD
prostatitis for pain, or ibuprofen if preferred and suitable. susceptibilities when
Offer antibiotic. available): -
ciprofloxacin (consider
Review antibiotic treatment after 14 days and
safety issues) OR
either stop antibiotics or continue for a further 14 days then
14 days if needed (based on assessment of ofloxacin (consider safety 200mg BD
- review
history, symptoms, clinical examination, urine issues) OR
and blood tests). trimethoprim (if 200mg BD
UK Health For detailed information click on the visual summary fluoroquinolone not
-
Security appropriate; seek
Agency specialist advice)
Second choice (after 500mg OD
discussion with specialist):
- 14 days then
levofloxacin (consider
Last updated:
safety issues) OR review
Oct 2018
co-trimoxazole 960mg BD -
IV antibiotics (click on visual summary)
Recurrent First advise about behavioural and personal First choice antibiotic 200mg single dose
urinary tract hygiene measures, and self-care (with D- prophylaxis: trimethoprim when exposed to a
-
infection mannose or cranberry products) to reduce the (avoid in pregnancy) OR trigger or
risk of UTI. 100mg at night
For postmenopausal women, if no improvement, nitrofurantoin (avoid at 100mg single dose
consider vaginal oestrogen (review within term) - if eGFR when exposed to a
12 months). ≥45 ml/minute trigger or -
For non-pregnant women, if no improvement, 50 to 100mg at
UK Health consider single-dose antibiotic prophylaxis for night
Security exposure to a trigger (review within 6 months). Second choice antibiotic 500mg single dose
Agency For non-pregnant women (if no improvement or prophylaxis: when exposed to a
-
no identifiable trigger) or with specialist advice amoxicillin OR trigger or
Last updated Oct for pregnant women, men, children or young 250mg at night
2018 people, consider a trial of daily antibiotic cefalexin 500mg single dose
prophylaxis (review within 6 months). when exposed to a
For detailed information click on the visual summary. trigger or
See also the NICE guideline on urinary tract infection 125mg at night -
in under 16s: diagnosis and management and the UK
Health Security Agency urinary tract infection:
diagnostic tools for primary care.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 12
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Catheter- Antibiotic treatment is not routinely needed for Non-pregnant women 100mg m/r BD (or
associated asymptomatic bacteriuria in people with a and men first choice if if unavailable
urinary tract urinary catheter. no upper UTI symptoms: 50mg QDS) -
infection Consider removing or, if not possible, changing nitrofurantoin (if eGFR ≥45
the catheter if it has been in place for more than ml/minute) OR
7 days
7 days. But do not delay antibiotic treatment. trimethoprim (if low risk of 200mg BD
-
Advise paracetamol for pain. resistance) OR
Advise drinking enough fluids to avoid amoxicillin (only if culture 500mg TDS
dehydration. results available and -
susceptible)
Offer an antibiotic for a symptomatic infection.
UK Health When prescribing antibiotics, take account of Non-pregnant women 400mg initial dose,
Security severity of symptoms, risk of complications, and men second choice then 200mg TDS
Agency previous urine culture and susceptibility results, if no upper UTI - 7 days
previous antibiotic use which may have led to symptoms:
resistant bacteria and local antimicrobial pivmecillinam (a penicillin)
Last updated: resistance data. Non-pregnant women 500mg BD or TDS
Nov 2018 Do not routinely offer antibiotic prophylaxis to and men first choice if (up to 1g to 1.5g
-
people with a short-term or long-term catheter. upper UTI symptoms: TDS or QDS for
cefalexin OR severe infections) 7 to 10 days
For detailed information click on the visual summary.
See also the UK Health Security Agency urinary tract co-amoxiclav (only if 500/125mg TDS
infection: diagnostic tools for primary care. culture results available -
and susceptible) OR
trimethoprim (only if 200mg BD
culture results available - 14 days
and susceptible) OR
ciprofloxacin (consider 500mg BD
- 7 days
safety issues)
Non-pregnant women and men IV antibiotics (click on visual summary)
Pregnant women first 500mg BD or TDS
choice: (up to 1g to 1.5g
- 7 to 10 days
cefalexin TDS or QDS for
severe infections)
Pregnant women second choice or IV antibiotics (click on visual summary)
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 13
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Children and young -
people (3 months and
over) first choice:
trimethoprim (if low risk of
resistance) OR
amoxicillin (only if culture -
results available and -
susceptible) OR
cefalexin OR -
co-amoxiclav (only if -
culture results available
and susceptible)
Children and young people (3 months and over) IV antibiotics (click on
visual summary)
Meningitis
Suspected
meningococcal
disease
For management guidance please refer to Meningococcal disease: guidance on public health management - GOV.UK (www.gov.uk)
Last updated:
June 2023
Status: Under
review
Prevention of
secondary For management guidance please refer to Meningococcal disease: guidance on public health management - GOV.UK (www.gov.uk)
case of
meningitis
Last updated:
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 14
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Gastrointestinal tract infections
Oral
candidiasis For management guidance please refer to NICE/Clinical Knowledge Summaries: Candida oral
Last updated:
June 2023
Status: Under
review
Infectious
diarrhoea For management guidance please refer to NICE/Clinical Knowledge Summaries: Gastroenteritis
Last updated:
June 2023
Status: Under
review
Traveller’s
diarrhoea For management guidance please refer to NICE/Clinical Knowledge Summaries: Diarrhoea - prevention and advice for travellers
Last updated:
June 2023
Status: Under
review
Threadworm
For management guidance please refer to NICE/Clinical Knowledge Summaries: Threadworm
Last updated:
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 15
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Clostridioides For suspected or confirmed C. difficile infection, First-line for first 125mg QDS
difficile see UK Health Security Agency’s guidance on episode of mild,
infection diagnosis and reporting. moderate or severe:
Assess: whether it is a first or further episode, vancomycin
severity of infection, individual risk factors for Second-line for first 200mg BD
complications or recurrence (such as age, frailty episode of mild,
or comorbidities). moderate or severe if
Existing antibiotics: review and stop unless vancomycin ineffective:
essential. If still essential, consider changing to fidaxomicin
UK Health one with a lower risk of C. difficile infection.
Security For further episode 200mg BD 10 days
Review the need to continue: proton pump within 12 weeks of
Agency inhibitors, other medicines with gastrointestinal symptom resolution
activity or adverse effects (such as laxatives), (relapse):
Last updated: medicines that may cause problems if people
Jul 2021 are dehydrated (such as NSAIDs). fidaxomicin
Do not offer antimotility medicines such as For further episode more 125mg QDS
loperamide. than 12 weeks after
symptom resolution
Offer an oral antibiotic to treat suspected or (recurrence):
confirmed C. difficile infection.
vancomycin OR
For adults, consider seeking prompt specialist
advice from a microbiologist or infectious fidaxomicin 200mg BD
diseases specialist before starting treatment.
For alternative antibiotics if first- and second-line antibiotics are
For children and young people, treatment should ineffective or for life-threatening infection seek specialist advice (see
be started by, or after advice from, a visual summary)
microbiologist, paediatric infectious diseases
specialist or paediatric gastroenterologist.
If antibiotics have been started for suspected
C. difficile infection, and subsequent stool
sample tests do not confirm infection, consider
stopping these antibiotics.
For detailed information click on the visual summary.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 16
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Helicobacter
pylori For management guidance please refer to NICE/BNF treatment summaries: Helicobacter pylori infection
Last updated:
June 2023
Status: Under
review
Acute Acute diverticulitis and systemically well: First-choice 500/125mg TDS
diverticulitis Consider no antibiotics, offer simple analgesia (uncomplicated acute
-
(for example paracetamol), advise to re-present diverticulitis):
if symptoms persist or worsen. co-amoxiclav
Acute diverticulitis and systemically unwell, Penicillin allergy or cefalexin: 500mg
immunosuppressed or significant co-amoxiclav unsuitable: BD or TDS (up to
comorbidity: offer an antibiotic. cefalexin (caution in 1g to 1.5g TDS or
Give oral antibiotics if person not referred to penicillin allergy) AND QDS for severe -
hospital for suspected complicated acute metronidazole OR infections)
Last updated: diverticulitis. metronidazole:
Nov 2019 Give IV antibiotics if admitted to hospital with 400mg TDS 5 days*
suspected or confirmed complicated acute trimethoprim AND trimethoprim:
diverticulitis (including diverticular abscess). metronidazole OR 200mg BD
If CT-confirmed uncomplicated acute -
metronidazole:
diverticulitis, review the need for antibiotics. 400mg TDS
* A longer course may be needed based on ciprofloxacin (only if ciprofloxacin:
clinical assessment. switching from IV 500mg BD
ciprofloxacin with metronidazole:
specialist advice; consider 400mg TDS
safety issues) AND
metronidazole
For IV antibiotics in complicated acute diverticulitis (including
diverticular abscess) see visual summary
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 17
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Genital tract infections
Epididymitis
For management guidance please refer to the BASHH United Kingdom guideline for the management of epididymo-orchitis
Last updated:
June 2023
Status: Under
review
Chlamydia
trachomatis/ For management guidance please refer to the BASHH United Kingdom guideline for the management of Chlamydia
urethritis
Last updated:
June 2023
Status: Under
review
Vaginal
candidiasis For management guidance please refer to the BASHH United Kingdom guideline for the management of vulvovaginal candidiasis
Last updated:
June 2023
Status: Under
review
Bacterial
vaginosis For management guidance please refer to the BASHH United Kingdom guideline for the management of bacterial vaginosis
Last updated:
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 18
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Genital herpes
For management guidance please refer to the BASHH United Kingdom guideline for the management of anogenital herpes
Last updated:
June 2023
Status: Under
review
Gonorrhoea
Last updated: For further management guidance please refer to the BASHH United Kingdom guideline for the management of Gonorrhoea
June 2023
Status: Under
review
Trichomoniasis
Last updated: For management guidance please refer to the BASHH United Kingdom guideline on the management of Trichomonas vaginalis
June 2023
Status: Under
review
Pelvic
inflammatory For further management guidance please refer to the BASHH United Kingdom national guideline on the management of pelvic inflammatory
disease disease
Last updated:
June 2023
Status: Under
review
Skin and soft tissue infections
Cold sores
Last updated: For management guidance please refer to NICE/Clinical Knowledge Summaries: Herpes simplex - oral
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 19
Doses Visual
Infection Key points Medicine Length
Adult Child summary
PVL-SA
Last updated: For management guidance please refer to UKHSA (PHE) PVL-Staphylococcus aureus infections: diagnosis and management
June 2023
Status: Under
review
Eczema Manage underlying eczema and flares with If not systemically unwell, do not routinely offer either a topical or oral
(bacterial treatments such as emollients and topical antibiotic
infection) corticosteroids, whether antibiotics are given or Topical antibiotic (if a topical is appropriate). For localised infections
not. only:
Symptoms and signs of secondary bacterial First choice: TDS
infection can include: weeping, pustules, crusts, fusidic acid 2% 5 to 7 days
no response to treatment, rapidly worsening
eczema, fever and malaise.
Oral antibiotic:
Not all flares are caused by a bacterial infection,
UK Health so will not respond to antibiotics. First choice: 500mg QDS
Security flucloxacillin
Eczema is often colonised with bacteria but may
Agency not be clinically infected. Penicillin allergy or 250mg BD (can be
flucloxacillin unsuitable: increased to
Do not routinely take a skin swab. clarithromycin OR 500mg BD for 5 to 7 days
Not systemically unwell: severe infections)
Last updated:
Mar 2021 Do not routinely offer either a topical or oral erythromycin (if macrolide 250mg to 500mg
antibiotic. needed in pregnancy; QDS
If an antibiotic is offered, when choosing consider benefit/harm)
between a topical or oral antibiotic, take account
of patient preferences, extent and severity of
symptoms or signs, possible adverse effects,
and previous use of topical antibiotics because
antimicrobial resistance can develop rapidly with
extended or repeated use.
Systemically unwell:
If MRSA suspected or confirmed – consult local microbiologist
Offer an oral antibiotic.
If there are symptoms or signs of cellulitis, see
cellulitis and erysipelas.
For detailed information click on the visual
summary.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 20
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Impetigo Localised non-bullous impetigo: Topical antiseptic:
Hydrogen peroxide 1% cream (other topical hydrogen peroxide 1% BD or TDS 5 days*
antiseptics are available but no evidence for
impetigo). Topical antibiotic:
If hydrogen peroxide unsuitable or ineffective, First choice: TDS
short-course topical antibiotic. fusidic acid 2%
Widespread non-bullous impetigo: Fusidic acid resistance TDS 5 days*
UK Health
Short-course topical or oral antibiotic. suspected or confirmed:
Security
Take account of person’s preferences, mupirocin 2%
Agency
practicalities of administration, previous use of Oral antibiotic:
topical antibiotics because antimicrobial First choice: 500mg QDS
resistance can develop rapidly with extended or flucloxacillin
Last updated: repeated use, and local antimicrobial resistance
Feb 2020 data. Penicillin allergy or 250mg BD
flucloxacillin unsuitable:
Bullous impetigo, systemically unwell, or 5 days*
clarithromycin OR
high risk of complications:
erythromycin (if macrolide 250 to 500mg
Short-course oral antibiotic. needed in pregnancy; QDS
Do not offer combination treatment with a topical consider benefit/harm)
and oral antibiotic to treat impetigo.
*5 days is appropriate for most, can be
increased to 7 days based on clinical judgement. If MRSA suspected or confirmed – consult local microbiologist
For detailed information click on the visual
summary.
Mastitis
Last updated: For management guidance please refer to NICE/Clinical Knowledge Summaries: Mastitis and breast abscess
June 2023
Status: Under
review
Tick bites
(Lyme
disease)
Last updated: For management guidance please refer to NICE NG95: Lyme disease
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 21
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Scabies
Last updated: For management guidance please refer to the BASHH United Kingdom national guideline on the management of Scabies
June 2023
Status: Under
review
Insect bites Most insect bites or stings will not need
and stings antibiotics.
Do not offer an antibiotic if there are no
symptoms or signs of infection.
If there are symptoms or signs of infection, see
UK Health cellulitis and erysipelas. - - - -
Security
Agency
Last updated:
Sep 2020
Leg ulcer Manage any underlying conditions to promote First-choice:
infection ulcer healing. flucloxacillin 500mg to 1g QDS - 7 days
Only offer an antibiotic when there are Penicillin allergy or if flucloxacillin unsuitable:
symptoms or signs of infection (such as redness doxycycline OR 200mg on day 1,
or swelling spreading beyond the ulcer, localised then 100mg OD
warmth, increased pain or fever). Few leg ulcers (can be increased
are clinically infected but most are colonised by to 200mg daily)
- 7 days
UK Health bacteria. clarithromycin OR 500mg BD
Security When prescribing antibiotics, take account of erythromycin (if macrolide 500mg QDS
Agency severity, risk of complications and previous needed in pregnancy;
antibiotic use. consider benefit/harm)
Second choice:
For detailed information click on the visual
Last updated: summary. co-amoxiclav OR 500/125mg TDS
Feb 2020 co-trimoxazole (in 960mg BD - 7 days
penicillin allergy)
For antibiotic choices if severely unwell or MRSA suspected or
confirmed, click on the visual summary
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 22
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Cellulitis and Exclude other causes of skin redness First choice:
erysipelas (inflammatory reactions or non-infectious flucloxacillin 500mg to 1g QDS 5 to 7 days*
causes).
Consider marking extent of infection with a Penicillin allergy or if flucloxacillin unsuitable:
single-use surgical marker pen. clarithromycin OR 500mg BD
erythromycin (if macrolide 500mg QDS
Offer an antibiotic. Take account of severity, site
needed in pregnancy;
of infection, risk of uncommon pathogens, any
consider benefit/harm) OR
microbiological results and MRSA status.
doxycycline (adults only) 200mg on day 1, 5 to 7 days*
UK Health Infection around eyes or nose is more -
OR then 100mg OD
Security concerning because of serious intracranial co-amoxiclav (children -
Agency complications. only: not in penicillin
*A longer course (up to 14 days in total) may be allergy)
needed but skin takes time to return to normal, If infection near eyes or nose:
Last updated: and full resolution at 5 to 7 days is not expected. co-amoxiclav 500/125mg TDS
Sept 2019 7 days*
Do not routinely offer antibiotics to prevent
recurrent cellulitis or erysipelas. If infection near eyes or nose (penicillin allergy):
clarithromycin AND 500mg BD
For detailed information click on the visual
metronidazole (only add in 400mg TDS
summary. 7 days*
children if anaerobes
suspected)
For alternative choice antibiotics for severe infection, suspected or
confirmed MRSA infection and IV antibiotics click on the visual summary
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 23
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Diabetic foot In diabetes, all foot wounds are likely to be Mild infection: first choice
infection colonised with bacteria. Diabetic foot infection flucloxacillin 500mg to 1g QDS - 7 days*
has at least 2 of: local swelling or induration;
erythema; local tenderness or pain; local Mild infection (penicillin allergy):
warmth; purulent discharge. clarithromycin OR 500mg BD
Severity is classified as: erythromycin (if macrolide 500mg QDS
Mild: local infection with 0.5 to less than 2cm needed in pregnancy;
erythema consider benefit/harm) OR
- 7 days*
UK Health Moderate: local infection with more than 2cm doxycycline 200mg on day 1,
Security erythema or involving deeper structures (such then 100mg OD
Agency as abscess, osteomyelitis, septic arthritis or (can be increased
fasciitis) to 200mg daily)
Last updated: Severe: local infection with signs of a systemic For antibiotic choices for moderate or severe infection, infections where
Oct 2019 Pseudomonas aeruginosa or MRSA is suspected or confirmed, and IV
inflammatory response.
antibiotics click on the visual summary
Start antibiotic treatment as soon as possible.
Take samples for microbiological testing before,
or as close as possible to, the start of treatment
When choosing an antibiotic, take account of
severity, risk of complications, previous
microbiological results and antibiotic use, and
patient preference.
*A longer course (up to a further 7 days) may be
needed based on clinical assessment. However,
skin does take time to return to normal, and full
resolution at 7 days is not expected.
Do not offer antibiotics to prevent diabetic foot
infection.
For detailed information click on the visual
summary.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 24
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Acne vulgaris First-line treatment options: offer a course of 1 First line: fixed 0.1% adapalene/
of the options, taking account of severity, combination of topical 2.5% benzoyl
preferences, and advantages/disadvantages of adapalene with topical peroxide OR 0.3%
each option. Completing the course is important benzoyl peroxide (for any adapalene/2.5%
because positive effects can take 6 to 8 weeks. acne severity, not in under benzoyl peroxide
Consider topical benzoyl peroxide monotherapy 9s) OR OD (thinly
as an alternative if first-line treatment options evening)
are contraindicated, or to avoid topical retinoids fixed combination of 0.025% tretinoin/
Last updated:
or an antibiotic (topical or oral). topical tretinoin with topical 1% clindamycin
Jun 2021 Do not use: monotherapy with a topical clindamycin (for any acne OD (thinly in the
antibiotic, monotherapy with an oral antibiotic, or severity, not in under 12s) evening)
a combination of a topical antibiotic and an oral OR
antibiotic. fixed combination of 3% benzoyl
Review first-line treatment at 12 weeks. topical benzoyl peroxide peroxide/1%
with topical clindamycin clindamycin OR
Only continue a topical or oral antibiotic for more
(for mild to moderate acne, 5% benzoyl
than 6 months in exceptional circumstances. Not available.
not in under 12s) OR peroxide/1%
Review at 3 monthly intervals, and stop the 12 weeks See the NICE
clindamycin OD (in
antibiotic as soon as possible. guideline on
the evening)
For detailed information see the NICE guideline on acne vulgaris.
acne vulgaris. fixed combination of 0.1% adapalene/
topical adapalene with 2.5% benzoyl
topical benzoyl peroxide peroxide OR 0.3%
AND either oral adapalene/2.5%
lymecycline or oral benzoyl peroxide
doxycycline (for moderate OD (in the
to severe acne, not in evening)
under 12s) OR AND
lymecycline 408mg
OD
OR
doxycycline 100mg
OD
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 25
Doses Visual
Infection Key points Medicine Length
Adult Child summary
topical azelaic acid AND 15% or 20%
either oral lymecycline or azelaic acid BD
oral doxycycline (for AND
moderate to severe acne,
lymecycline 408mg
not in under 12s)
OD
OR
doxycycline 100mg
OD
Alternative: topical 5% benzoyl
benzoyl peroxide peroxide OD to BD
Dermatophyte
infection: skin For management guidance please refer to NICE/Clinical Knowledge Summaries: Fungal skin infection - body and groin
Last updated:
June 2023
Status: Under
review
Dermatophyte
infection: nail For management guidance please refer to NICE/Clinical Knowledge Summaries: Fungal nail infection
Last updated:
June 2023
Status: Under
review
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 26
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Human and Offer an antibiotic for a human or animal bite if First choice:
animal bites there are symptoms or signs of infection, such co-amoxiclav 250/125mg or 3 days for
as increased pain, inflammation, fever, 500/125mg TDS prophylaxis
discharge or an unpleasant smell. Take a swab
5 days for
for microbiological testing if there is discharge
treatment*
(purulent or non-purulent) from the wound.
Do not offer antibiotic prophylaxis if a human or Penicillin allergy or co-amoxiclav unsuitable:
animal bite has not broken the skin. doxycycline AND 200mg on day 1,
then 100mg or 3 days for
UK Health Human bite:
200mg daily prophylaxis
Security Offer antibiotic prophylaxis if the human bite has
Agency metronidazole 400mg TDS 5 days for
broken the skin and drawn blood. treatment*
Consider antibiotic prophylaxis if the human bite seek specialist advice in pregnancy
has broken the skin but not drawn blood if it is in IV antibiotics (click on visual summary)
Last updated: a high-risk area or person at high risk.
Nov 2020
Cat bite:
Offer antibiotic prophylaxis if the cat bite has
broken the skin and drawn blood.
Consider antibiotic prophylaxis if the cat bite has
broken the skin but not drawn blood if the wound
could be deep.
Dog or other traditional pet bite (excluding
cat bite)
Do not offer antibiotic prophylaxis if the bite has
broken the skin but not drawn blood.
Offer antibiotic prophylaxis if the bite has broken
the skin and drawn blood if it has caused
considerable, deep tissue damage or is visibly
contaminated (for example, with dirt or a tooth).
Consider antibiotic prophylaxis if the bite has
broken the skin and drawn blood if it is in a high-
risk area or person at high risk.
*course length can be increased to 7 days (with
review) based on clinical assessment of the
wound.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 27
Doses Visual
Infection Key points Medicine Length
Adult Child summary
Varicella
zoster/ For management guidance please refer to NICE/Clinical Knowledge Summaries - Chickenpox
chickenpox
Or
NICE/Clinical Knowledge Summaries - Shingles
Herpes zoster/
shingles
Last updated:
June 2023
Status: Under
review
Eye infections
Conjunctivitis
Last updated: For management guidance please refer to NICE/Clinical Knowledge Summaries: Conjunctivitis - infective
June 2023
Status: Under
review
Blepharitis
Last updated: For management guidance please refer to NICE/Clinical Knowledge Summaries: Blepharitis
June 2023
Status: Under
review
Suspected dental infections in primary care (outside dental settings)
This guidance is not designed to be a definitive guide to oral conditions, as GPs should not be involved in dental treatment. Patients presenting to non-dental primary
care services with dental problems should be directed to their regular dentist, or if this is not possible, to the NHS 111 service (in England), who will be able to
provided details of how to access emergency dental care.
For further information on this topic please refer to the: College of General Dentistry and Faculty of Dental Surgery (FDS) of the Royal College of Surgeons of
England - Antimicrobial Prescribing in Dentistry: Good Practice Guidelines.
Abbreviations
BD, twice a day; eGFR, estimated glomerular filtration rate; IM, intramuscular; IV, intravenous; MALToma, mucosa-associated lymphoid tissue lymphoma; m/r,
modified release; MRSA, methicillin-resistant Staphylococcus aureus; MSM, men who have sex with men; stat, given immediately; OD, once daily; TDS, 3 times a
day; QDS, 4 times a day.
Summary of antimicrobial prescribing guidance – managing common infections (June 2023) 28
You might also like
- LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document8 pagesLPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085le sage0% (1)
- DRUG STUDY DoxycyclineDocument2 pagesDRUG STUDY DoxycyclineAMIN BARINo ratings yet
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Convulsions (Seizures) : Prof. Dr. Shahenaz M. HusseinDocument26 pagesConvulsions (Seizures) : Prof. Dr. Shahenaz M. HusseinAriefSuryoWidodo100% (1)
- Antimicrobial Prescribing GuidanceDocument24 pagesAntimicrobial Prescribing GuidanceJason Merari PeranginanginNo ratings yet
- Summary Antimicrobial Prescribing Guidance - July 21 For BNFDocument31 pagesSummary Antimicrobial Prescribing Guidance - July 21 For BNFbarcanbiancaNo ratings yet
- Management of Infection in Primary Care Adapted For Local UseDocument15 pagesManagement of Infection in Primary Care Adapted For Local UseWizri SuharianiNo ratings yet
- Meningitis ReviewDocument2 pagesMeningitis ReviewBolbol hayranNo ratings yet
- نموذج تعليمات المضادات الحيوية (أطفالDocument9 pagesنموذج تعليمات المضادات الحيوية (أطفال5n7qd7fjjjNo ratings yet
- Pharmacology: Antibiotic PrescribingDocument4 pagesPharmacology: Antibiotic PrescribingekanovicaNo ratings yet
- GHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalDocument19 pagesGHC Lower Respiratory Tract Antimicrobial Guideline V 3 FinalNicthe Ruiz RodríguezNo ratings yet
- Recommendation For The Use of Antibiotics For The Treatment of InfectionDocument5 pagesRecommendation For The Use of Antibiotics For The Treatment of InfectionGem BorjaNo ratings yet
- Infections in Primary CareDocument5 pagesInfections in Primary CareAtta Muhammad Memon100% (1)
- HTTPS:WWW - Nottsapc.nhs - Uk:Media:Mtqjk4pd:Dental AbscessDocument2 pagesHTTPS:WWW - Nottsapc.nhs - Uk:Media:Mtqjk4pd:Dental Abscesstinosan3No ratings yet
- NICE Otitis Media Guideline 2022Document7 pagesNICE Otitis Media Guideline 2022Oscar ChauNo ratings yet
- Universiti Teknologi Mara (Uitm) Puncak Alam Campus Faculty of Health SciencesDocument9 pagesUniversiti Teknologi Mara (Uitm) Puncak Alam Campus Faculty of Health SciencesMOHD MU'IZZ BIN MOHD SHUKRINo ratings yet
- 2021 Infection Management PosterDocument1 page2021 Infection Management PosterBosco WoodsNo ratings yet
- Emma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)Document28 pagesEmma Best, Simon Briggs, Rosemary Ikram, Mark Thomas - Antibiotics - Choices For Common Infections 2013 Edition (BPAC NZ) (2013, BPAC NZ)igd rsudcpNo ratings yet
- Antibiotics Guide 2013Document30 pagesAntibiotics Guide 2013Stefani NoviliaNo ratings yet
- 144TD (C) 25 (E3) - Issue No 4 - Ear Nose and Throat (ENT) Infections Antibiotic GuidelinesDocument9 pages144TD (C) 25 (E3) - Issue No 4 - Ear Nose and Throat (ENT) Infections Antibiotic GuidelinesOprea DoruNo ratings yet
- Nameofthedrugdosage, Route and Frequency Mechanism of Action Indication Contraindication Side Effects Client'S Response Nursing ResponsibilitiesDocument2 pagesNameofthedrugdosage, Route and Frequency Mechanism of Action Indication Contraindication Side Effects Client'S Response Nursing ResponsibilitiesAndrea Albester GarinoNo ratings yet
- Ear, Nose and Throat (ENT) Infections Antibiotic GuidelinesDocument9 pagesEar, Nose and Throat (ENT) Infections Antibiotic GuidelinesAtta Muhammad MemonNo ratings yet
- Adult Outpatient Treatment Recommendations - Antibiotic Use - CDCDocument4 pagesAdult Outpatient Treatment Recommendations - Antibiotic Use - CDCEdward LaurentNo ratings yet
- Acute Pyelonephritis AdultDocument1 pageAcute Pyelonephritis AdultMeagan SotoNo ratings yet
- المرشدات العلاجية للصادات في الامراض الاذنيةDocument8 pagesالمرشدات العلاجية للصادات في الامراض الاذنيةyasinoNo ratings yet
- Leaflet - Covid 19 Vaccination of ChildrenDocument2 pagesLeaflet - Covid 19 Vaccination of ChildrenshifanahmedNo ratings yet
- Proton Pump Inhibitors (Ppis) and Corticosteroids Advisory Guidance On When To Initiate A Ppi For Gastro-ProtectionDocument3 pagesProton Pump Inhibitors (Ppis) and Corticosteroids Advisory Guidance On When To Initiate A Ppi For Gastro-ProtectionjerryNo ratings yet
- Guidelines For Treatment of Infections in Primary Care in Hull and East RidingDocument22 pagesGuidelines For Treatment of Infections in Primary Care in Hull and East RidingSiLvia Riska PratiwiNo ratings yet
- Amoxicillin (Amoxycillin) : PresentationDocument4 pagesAmoxicillin (Amoxycillin) : PresentationRavikiran SuryanarayanamurthyNo ratings yet
- Austprescr 45 179Document1 pageAustprescr 45 179angelNo ratings yet
- BCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)Document10 pagesBCCDC Non-Certified Practice Decision Support Tool Pelvic Inflammatory Disease (PID)sandeepv08No ratings yet
- Drug Study FormatDocument5 pagesDrug Study FormatVannesa TarifaNo ratings yet
- Covid Vaccine Info SheetDocument10 pagesCovid Vaccine Info SheetHuatNo ratings yet
- Paracetamol JurnalDocument4 pagesParacetamol JurnalkanazNo ratings yet
- Acute PharyngitisDocument3 pagesAcute Pharyngitisdr_dediet1No ratings yet
- Management of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015Document66 pagesManagement of Infection Guidance For Primary Care For Consultation and Local Adaptation - July 2015neleatucicovshiiNo ratings yet
- FAQs For Doctors-PEDIADocument11 pagesFAQs For Doctors-PEDIAzzNo ratings yet
- AzithromycinDocument10 pagesAzithromycinShaina MentangNo ratings yet
- Pre Vaccination Screening FormDocument10 pagesPre Vaccination Screening Formbersabeh abayNo ratings yet
- Flu Consent FormDocument2 pagesFlu Consent FormTiger Palm TigerNo ratings yet
- Periorbital Cellulitis CA4024v3Document5 pagesPeriorbital Cellulitis CA4024v3John M. HemsworthNo ratings yet
- Immunizations To Be Taken On Gandako'S First VisitDocument5 pagesImmunizations To Be Taken On Gandako'S First VisitKryzza LeizellNo ratings yet
- Antibiotics Guide 2017Document32 pagesAntibiotics Guide 2017Josef SosNo ratings yet
- Pedoman Penggunaan Antibiotik Pada PasienDocument5 pagesPedoman Penggunaan Antibiotik Pada PasienErvina Lie100% (1)
- Corticosteroids For Sore Throat: A Clinical Practice GuidelineDocument7 pagesCorticosteroids For Sore Throat: A Clinical Practice GuidelineAmelia 'amek' RahayuNo ratings yet
- An Approach To Treating Long COVID: First Line TherapiesDocument3 pagesAn Approach To Treating Long COVID: First Line TherapiesflorentinaNo ratings yet
- Bpacnz Antibiotics GuideDocument40 pagesBpacnz Antibiotics GuideBulborea MihaelaNo ratings yet
- Meropenem Meropenem: (Lexi-Drugs Multinational)Document1 pageMeropenem Meropenem: (Lexi-Drugs Multinational)Jhoann JamanilaNo ratings yet
- Common Medications in PHCDocument19 pagesCommon Medications in PHCsalwakh266No ratings yet
- Sore Throat (Acute) : Antimicrobial Prescribing: National Institute For Health and Care Excellence GuidelineDocument18 pagesSore Throat (Acute) : Antimicrobial Prescribing: National Institute For Health and Care Excellence GuidelinesabaNo ratings yet
- Azithromycin Medication PDFDocument1 pageAzithromycin Medication PDFmp1757No ratings yet
- COVID Vaccination Side Effect Reducing OTC Medicines and NutraceuticalsDocument1 pageCOVID Vaccination Side Effect Reducing OTC Medicines and NutraceuticalsGlowstarNo ratings yet
- Antiemetic Drug Use in Children What The.3Document6 pagesAntiemetic Drug Use in Children What The.3Zafitri AsrulNo ratings yet
- Acute Otitis Media in ChildrenDocument7 pagesAcute Otitis Media in ChildrenssssceNo ratings yet
- Antibiotic GuidDocument11 pagesAntibiotic Guidlaur_rbNo ratings yet
- I CARE Protocol SummaryDocument4 pagesI CARE Protocol SummaryServaas OostrikNo ratings yet
- CH 023 STG Acute Otitis MediaDocument7 pagesCH 023 STG Acute Otitis MediaUdaykumarNo ratings yet
- EPI Vaccines HandoutsDocument14 pagesEPI Vaccines HandoutsStephen Pilar PortilloNo ratings yet
- EPI Vaccines HandoutsDocument14 pagesEPI Vaccines HandoutsBurhan uddin100% (11)
- Antiobtic PolicyDocument3 pagesAntiobtic PolicyRajinder Kumar BassanNo ratings yet
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryFrom EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryNo ratings yet
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingFrom EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNo ratings yet
- Id 397 TeicoplaninDocument2 pagesId 397 TeicoplaninStacey WoodsNo ratings yet
- Palliative2 Nausea MedtableDocument2 pagesPalliative2 Nausea MedtableStacey WoodsNo ratings yet
- IDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistDocument3 pagesIDSA Releases Guidance On Antibiotic Selection For Gram-Negative Antimicrobial-Resistant Bacterial Infections - ACP Internist Weekly - ACP InternistStacey WoodsNo ratings yet
- Appropriate Use of Laxatives in The Older PersonDocument7 pagesAppropriate Use of Laxatives in The Older PersonStacey WoodsNo ratings yet
- Therapeutic Drug Monitoring in Adults at NUH2011 FinalDocument2 pagesTherapeutic Drug Monitoring in Adults at NUH2011 FinalStacey WoodsNo ratings yet
- How To Select Antibiotics in Celiac DiseaseDocument6 pagesHow To Select Antibiotics in Celiac DiseaseStacey WoodsNo ratings yet
- Blood Transfusion - Indications, Administration and Adverse Reactions PDFDocument9 pagesBlood Transfusion - Indications, Administration and Adverse Reactions PDFStacey WoodsNo ratings yet
- Ventilator-Associated Pneumonia in The ICUDocument8 pagesVentilator-Associated Pneumonia in The ICUnyuwwchocolavaNo ratings yet
- Hypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityDocument7 pagesHypocaloric, High-Protein Nutrition Therapy For Critically Ill Patients With ObesityStacey WoodsNo ratings yet
- 22 MetabolicEncephalopathies FinalDocument19 pages22 MetabolicEncephalopathies FinalShravan BimanapalliNo ratings yet
- Complete Clinical Card Booklet 2014.2014 Booklet CroppedDocument30 pagesComplete Clinical Card Booklet 2014.2014 Booklet CroppedStacey Woods100% (1)
- Preventing Aspiration Pneumonia by Addressing Three Key Risk Factors - Dysphagia, Poor Oral Hygiene, and Medication UseDocument14 pagesPreventing Aspiration Pneumonia by Addressing Three Key Risk Factors - Dysphagia, Poor Oral Hygiene, and Medication UseStacey WoodsNo ratings yet
- Shock ConcensusDocument21 pagesShock ConcensusRezka OctavianoNo ratings yet
- NCP For FractureDocument4 pagesNCP For FracturePeejay Padigdig Feliciano100% (2)
- Prolapse Lumbar DiscDocument40 pagesProlapse Lumbar DiscAlfred BantigueNo ratings yet
- ALSANGEDY BULLETS For PACES Ankylosing Spondylitis 2nd EditionDocument2 pagesALSANGEDY BULLETS For PACES Ankylosing Spondylitis 2nd EditionGhulamMemonNo ratings yet
- Surgical ConscienceDocument35 pagesSurgical ConscienceTakale BuloNo ratings yet
- Types of WoundsDocument4 pagesTypes of WoundsHanarisha Putri AzkiaNo ratings yet
- Examination of The Gastrointestinal TractDocument44 pagesExamination of The Gastrointestinal TractDrNaveen Singh Rajpurohit Kadu100% (1)
- Living With A Tracheostomy: Patient EducationDocument2 pagesLiving With A Tracheostomy: Patient EducationJack Supramaniam100% (1)
- Relevant Equine Renal Anatomy, Physiology and Mechanisms of AKI ReviewDocument12 pagesRelevant Equine Renal Anatomy, Physiology and Mechanisms of AKI ReviewMarilú ValdepeñaNo ratings yet
- Lesson 4Document6 pagesLesson 4doldol ocampoNo ratings yet
- Case Study SampleDocument4 pagesCase Study SamplenivienneNo ratings yet
- Dealing With Shift Work and FatigueDocument14 pagesDealing With Shift Work and FatigueA. AkbariNo ratings yet
- Dexamethasone: (Martindale: The Complete Drug Reference) Drug NomenclatureDocument11 pagesDexamethasone: (Martindale: The Complete Drug Reference) Drug NomenclaturemaryNo ratings yet
- Literature Review: The Relationship Between Sleep Patterns and The Incidence of Hypertension in The ElderlyDocument22 pagesLiterature Review: The Relationship Between Sleep Patterns and The Incidence of Hypertension in The ElderlyCalvin permana pinemNo ratings yet
- Sertifikat Anik (IPCN)Document56 pagesSertifikat Anik (IPCN)Uus HarryNo ratings yet
- Clinical Microscopy Services PDFDocument5 pagesClinical Microscopy Services PDFNaima AmrosiNo ratings yet
- Obstructed Labor & Prolonged LaburDocument22 pagesObstructed Labor & Prolonged LaburOmari Kabelwa100% (1)
- UNEP Directory March 2021Document34 pagesUNEP Directory March 2021Perera KusalNo ratings yet
- Final PhysicalDocument409 pagesFinal PhysicalAbhishiktaAbhiNo ratings yet
- GR2 Plasmodium-Spp PDFDocument29 pagesGR2 Plasmodium-Spp PDFEran Mark RojasNo ratings yet
- Case StudyDocument30 pagesCase StudyNur SolehahNo ratings yet
- Bhoomi PatelDocument9 pagesBhoomi PatelPooja PanchalNo ratings yet
- PMDC Full Information PaperDocument9 pagesPMDC Full Information PaperjazzyNo ratings yet
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezNo ratings yet
- Blood Cells LabDocument7 pagesBlood Cells LabKameron WardNo ratings yet
- Dr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureDocument32 pagesDr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureShahadat Hossain BabuNo ratings yet
- Presentation DH (Repaired)Document22 pagesPresentation DH (Repaired)Anmol SinghNo ratings yet
- Colorado Department of Public Health and Environment Dial 2.0 Changes PresentationDocument15 pagesColorado Department of Public Health and Environment Dial 2.0 Changes PresentationMichael_Roberts2019No ratings yet
- Viruses 09 00029 PDFDocument10 pagesViruses 09 00029 PDFJimeno Franscisco de los pozosNo ratings yet