You might also like
- Trigeminal nerve anatomy and functionsDocument5 pagesTrigeminal nerve anatomy and functionsManuel GeronimoNo ratings yet
- DEAFNESS, DIZZINESS, AND VertigoDocument46 pagesDEAFNESS, DIZZINESS, AND VertigoDian DestriyanahNo ratings yet
- Mechanisms of Perception: Audition and MoreDocument24 pagesMechanisms of Perception: Audition and Morejeyn100% (1)
- Clinical Anatomy of the Vestibular SystemDocument21 pagesClinical Anatomy of the Vestibular Systemaditya febriansyahNo ratings yet
- Lab Act Special SensesDocument7 pagesLab Act Special SensesJhia TorreonNo ratings yet
- Cranial Nerve 8 (Vestibulo-Cochlear)Document14 pagesCranial Nerve 8 (Vestibulo-Cochlear)osakaNo ratings yet
- NEURO - Topic 1 - Additional SlidesDocument25 pagesNEURO - Topic 1 - Additional SlidesreaobokasegoeNo ratings yet
- Cullen - 2016 - Physiology of Central Pathways-AnnotatedDocument24 pagesCullen - 2016 - Physiology of Central Pathways-AnnotatedRosarioNo ratings yet
- The Anatomy of The Cranial Nerves Vii-XiiDocument38 pagesThe Anatomy of The Cranial Nerves Vii-Xiiabdul azizNo ratings yet
- Medulla Oblongata Nucleus (Final)Document7 pagesMedulla Oblongata Nucleus (Final)Hassan.shehri100% (3)
- Faal 4 - Telinga (DR - Sony)Document46 pagesFaal 4 - Telinga (DR - Sony)sarahwahyuni36No ratings yet
- Tutor 16.2 GRACE NASYA (18-091) 4BDocument92 pagesTutor 16.2 GRACE NASYA (18-091) 4BGrace HerlisNo ratings yet
- WEEK 16 LABORATORY EXERCISE Special SensesDocument10 pagesWEEK 16 LABORATORY EXERCISE Special SensesEricka ElloNo ratings yet
- 6th Lecture - Physiology of The Brain Stem - CNS PhysiologyDocument13 pages6th Lecture - Physiology of The Brain Stem - CNS PhysiologyAnastasia SoareNo ratings yet
- Cerebellum Anatomy and FunctionsDocument43 pagesCerebellum Anatomy and FunctionsHarmas Novryan FarezaNo ratings yet
- Enfermedad Vestibular FelinaDocument8 pagesEnfermedad Vestibular FelinaPamela Susana Rivera GómezNo ratings yet
- The Nervous System: Na ShaoDocument79 pagesThe Nervous System: Na ShaoArvindhanNo ratings yet
- 8th NerveDocument91 pages8th NerveKinjal SharmaNo ratings yet
- Piter - LR - Peripheral Balance Examination1Document29 pagesPiter - LR - Peripheral Balance Examination1Arief FakhrizalNo ratings yet
- Table Describing The Vestibulocochlear NerveDocument82 pagesTable Describing The Vestibulocochlear NerveIqtader hoque khan AkibNo ratings yet
- Neuro AvesDocument23 pagesNeuro AvesMiriam CaramicoNo ratings yet
- Download ebook Psychology Psyc2020 Psyc2021 Custom Edition By Schutte E Ed Et A Pdf full chapter pdfDocument67 pagesDownload ebook Psychology Psyc2020 Psyc2021 Custom Edition By Schutte E Ed Et A Pdf full chapter pdfedward.bittner820100% (25)
- The Science Behind Holosync and Other NeurotechnologiesDocument13 pagesThe Science Behind Holosync and Other NeurotechnologiesTheHiddenSoldiersNo ratings yet
- Spinal Cord and MedullaDocument34 pagesSpinal Cord and MedullaveegeerNo ratings yet
- AuriculotherapyDocument14 pagesAuriculotherapyapi-3769566100% (3)
- 8 KandleDocument7 pages8 KandleKezia KurniaNo ratings yet
- Vestibular Disease: Understanding Peripheral and Central CausesDocument7 pagesVestibular Disease: Understanding Peripheral and Central CausesBruno CantinNo ratings yet
- Pembimbing: Prof - Dr. Zainal Muttaqien, PHD, SP - Bs (K) Edwin Sugondo Taufik - 22041920320001Document25 pagesPembimbing: Prof - Dr. Zainal Muttaqien, PHD, SP - Bs (K) Edwin Sugondo Taufik - 22041920320001Vicky NovitasariNo ratings yet
- Functional Classification and Emergence of Cranial NervesDocument10 pagesFunctional Classification and Emergence of Cranial NervesObansa JohnNo ratings yet
- The Vestibular System: Sensing Head MovementsDocument14 pagesThe Vestibular System: Sensing Head MovementsEslam ElsayedNo ratings yet
- I Olfactory Nerve Anterior Olfactory Nucleus Transmits The Sense of SmellDocument4 pagesI Olfactory Nerve Anterior Olfactory Nucleus Transmits The Sense of SmellalvinNo ratings yet
- Cranial NervesDocument65 pagesCranial NervesatefmaboodNo ratings yet
- Acute Rotatory Vertigo Caused by A SmallDocument8 pagesAcute Rotatory Vertigo Caused by A SmallasasakopNo ratings yet
- Cerebellum: Usmle Target: Stanford School of Medicine NeurologyDocument8 pagesCerebellum: Usmle Target: Stanford School of Medicine NeurologyKarun BhattaraiNo ratings yet
- Why, . Sign and Symptom!!!: Anwar Wardy, MD - Neu Department of Neurology FKK UmjDocument29 pagesWhy, . Sign and Symptom!!!: Anwar Wardy, MD - Neu Department of Neurology FKK UmjNurul Wandasari SNo ratings yet
- The Central Nervous System: Lee Kui SoonDocument38 pagesThe Central Nervous System: Lee Kui SoonSayapPutihNo ratings yet
- White MatterDocument19 pagesWhite MatterZoya MoraniNo ratings yet
- d8c Cranial NervesDocument29 pagesd8c Cranial NervesYhemmy Lhawal JummyNo ratings yet
- Medulla OblongataDocument22 pagesMedulla Oblongataveegeer100% (1)
- Physiologyofequilibriumbalance 111029153537 Phpapp01Document43 pagesPhysiologyofequilibriumbalance 111029153537 Phpapp01Dorin PathakNo ratings yet
- 8 Brainstem 2Document20 pages8 Brainstem 2sjs6r8wwv9No ratings yet
- Introduction and Spinal CordDocument27 pagesIntroduction and Spinal Cordapi-196413370% (1)
- 1 s2.0 S2211568413002052 MainDocument7 pages1 s2.0 S2211568413002052 MaindoraNo ratings yet
- Nakajima 2015Document9 pagesNakajima 2015Carturo VduncanNo ratings yet
- Nervus Cranialis Dan Basis Cranii: Praktikum Anatomi IIDocument42 pagesNervus Cranialis Dan Basis Cranii: Praktikum Anatomi IIRahayu OktalianiNo ratings yet
- Cranial NervesDocument39 pagesCranial NervesVaishnavi SNo ratings yet
- CerebellumDocument16 pagesCerebellumjainilNo ratings yet
- Cranial Nerve I - Olfactory NerveDocument6 pagesCranial Nerve I - Olfactory NerveAysha AishaNo ratings yet
- Bell's Palsy Causes, Symptoms, and Multidisciplinary TreatmentDocument8 pagesBell's Palsy Causes, Symptoms, and Multidisciplinary TreatmentMarsya Yulinesia LoppiesNo ratings yet
- Week 4 Lab Exercise - Special SensesDocument12 pagesWeek 4 Lab Exercise - Special SensesJoselito JardielNo ratings yet
- Facial Nerve: From Anatomy To Pathology: F. ToulgoatDocument10 pagesFacial Nerve: From Anatomy To Pathology: F. ToulgoatIman PradanaNo ratings yet
- Cap 11 - 22 Handbook of Clinical AudiologyDocument216 pagesCap 11 - 22 Handbook of Clinical AudiologyCami IrribarraNo ratings yet
- Chapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDocument4 pagesChapter 3 Anatomical Organization of Cranial Nerves 2009 Manual Therapy For The Cranial NervesDaniela Bustos PéndolaNo ratings yet
- CerebellumDocument14 pagesCerebellumapi-508474347No ratings yet
- Cranial Nerves Lecture OverviewDocument30 pagesCranial Nerves Lecture Overviewcilla235No ratings yet
- Nervous System 127 150Document23 pagesNervous System 127 150Claw GamerNo ratings yet
- Cranial Nerves: Anatomy and Physiology: AppendixDocument13 pagesCranial Nerves: Anatomy and Physiology: Appendixgolagani praveenkumarNo ratings yet
- Coordination in the human bodyDocument9 pagesCoordination in the human bodyEdgar LeungNo ratings yet
- Vestibular DisordersDocument8 pagesVestibular DisordersHilwy Al-haninNo ratings yet
- Urinary SystemDocument5 pagesUrinary SystemDonnabell DayudayNo ratings yet
- Schwartz's Hour Notes On TraumaDocument19 pagesSchwartz's Hour Notes On TraumaEver Seneca EscaLera100% (2)
- Meningitis Seminar 1Document38 pagesMeningitis Seminar 1vani reddyNo ratings yet
- Acute MX of StrokeDocument23 pagesAcute MX of StrokeAshish GuragainNo ratings yet
- Neck Pain and Lower Back Pain. Med Clin N Am. 2019.Document14 pagesNeck Pain and Lower Back Pain. Med Clin N Am. 2019.Jose Fernando Diez100% (1)
- Anaphy Midterm ExaminationDocument6 pagesAnaphy Midterm ExaminationCarmela Jane SonzaNo ratings yet
- Epbl 2 (Deep Venous Thrombosis)Document7 pagesEpbl 2 (Deep Venous Thrombosis)Noor Ul AminNo ratings yet
- 36 Applied NeuroscienceDocument26 pages36 Applied Neurosciencecercuri pătrate de fumNo ratings yet
- Pre Mid Assignment 1 Sania Saddique (Book)Document7 pagesPre Mid Assignment 1 Sania Saddique (Book)Sania SaddiqueNo ratings yet
- Lesions of The Visual PathwayDocument2 pagesLesions of The Visual PathwayM StojanovskaNo ratings yet
- The Nigrostriatal PathwayDocument13 pagesThe Nigrostriatal Pathwayapi-534201968No ratings yet
- Introduction To Anatomy and Homeostasis Within The BodyDocument24 pagesIntroduction To Anatomy and Homeostasis Within The BodyTrinity SherNo ratings yet
- STING Agonist-Loaded, CD47/PD-L1-targeting Nanoparticles Potentiate Antitumor Immu-Nity and Radiotherapy For GlioblastomaDocument19 pagesSTING Agonist-Loaded, CD47/PD-L1-targeting Nanoparticles Potentiate Antitumor Immu-Nity and Radiotherapy For GlioblastomaAnonymous HUY0yRexYfNo ratings yet
- Prostate-Induced Orgasms:: A Concise Review Illustrated With A Highly Relevant Case StudyDocument5 pagesProstate-Induced Orgasms:: A Concise Review Illustrated With A Highly Relevant Case StudyDayanaNo ratings yet
- A Rare Presentation of Solitary Giant NeurofibromaDocument7 pagesA Rare Presentation of Solitary Giant NeurofibromaAthenaeum Scientific PublishersNo ratings yet
- Final Synthesis EssayDocument5 pagesFinal Synthesis Essayapi-617074664No ratings yet
- Cerebral Edema Associated With MeningiomaDocument3 pagesCerebral Edema Associated With MeningiomaEstefania Ramirez CardonaNo ratings yet
- Hypothalamic-Pituitary Axis NotesDocument9 pagesHypothalamic-Pituitary Axis NotesSreejith Jagal KishoreNo ratings yet
- Li LBM 1 THT KL (Nallury)Document9 pagesLi LBM 1 THT KL (Nallury)Nallury Rizqi100% (1)
- Endocrine System: LECTURER: Durrefishan KhillatDocument8 pagesEndocrine System: LECTURER: Durrefishan Khillatkalsoom iqbalNo ratings yet
- Odontogenesis NotesDocument14 pagesOdontogenesis NotesClarisse Mendoza100% (1)
- Blue Red LesionDocument14 pagesBlue Red LesionXara Barretto MagadiaNo ratings yet
- Clinical Classification of Cerebral PalsyDocument23 pagesClinical Classification of Cerebral PalsymiNo ratings yet
- Herniated Nucleus Pulposus (HNP)Document21 pagesHerniated Nucleus Pulposus (HNP)Kaye100% (1)
- METS Gait Deviations & AVN CausesDocument10 pagesMETS Gait Deviations & AVN CausesClaNo ratings yet
- Neurologic Examination: Cranial NervesDocument68 pagesNeurologic Examination: Cranial Nerves2013SecBNo ratings yet
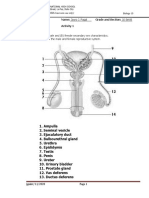
- INHS Biology Class Identifies Male and Female Reproductive PartsDocument6 pagesINHS Biology Class Identifies Male and Female Reproductive PartsJayro Jacuma PagalNo ratings yet
- The Neurologyof Sleep 2012 Published FormDocument18 pagesThe Neurologyof Sleep 2012 Published FormNeurologie PediatricaNo ratings yet
- Brain Tumor Localization Through Image ProcessingDocument7 pagesBrain Tumor Localization Through Image ProcessingJohn AmonNo ratings yet
- HypermetropiaDocument42 pagesHypermetropiaMalik AllahbachayaNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (17)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)