You might also like
- Chronic Pain Management ChartsDocument2 pagesChronic Pain Management Chartslrpokhrel100% (3)
- Se LF Di SC Ip Li NeDocument9 pagesSe LF Di SC Ip Li NeHannah Andrea Laparan100% (2)
- Zhi Gang Sha - Power Healing. The Four Keys To Energizing Your Body, Mind, and Spirit-HarperSanFrancisco (2003)Document276 pagesZhi Gang Sha - Power Healing. The Four Keys To Energizing Your Body, Mind, and Spirit-HarperSanFrancisco (2003)Defne Güller100% (3)
- Pericardial Diseases - Dr. BartolomeDocument8 pagesPericardial Diseases - Dr. BartolomeMedisina101No ratings yet
- Pedh ExamDocument12 pagesPedh ExamJames100% (2)
- 4 +basic+nutritionDocument71 pages4 +basic+nutritionJasmine CorreosNo ratings yet
- Elimination DisordersDocument30 pagesElimination DisordersFaridatul IsniyahNo ratings yet
- Concept Map of CellulitisDocument8 pagesConcept Map of CellulitisReese Anne100% (1)
- Dr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - OHS Modern ConceptDocument3 pagesDr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - OHS Modern ConceptDr. Prakash KulkarniNo ratings yet
- Having Nasal Surgery? Don't You Become An Empty Nose Victim!From EverandHaving Nasal Surgery? Don't You Become An Empty Nose Victim!No ratings yet
- Lesson Plan On AneurysmDocument13 pagesLesson Plan On AneurysmAmlan jyoti thanapati100% (1)
- Lha Ceremony 0210Document2 pagesLha Ceremony 0210Denis HengNo ratings yet
- Reflexology New Patient FormDocument7 pagesReflexology New Patient FormOana Iftimie100% (2)
- The Effect of Chamomile Tea To Induce A Persons Sleepiness FINALDocument47 pagesThe Effect of Chamomile Tea To Induce A Persons Sleepiness FINALMaxinne Alquilos MadroñalNo ratings yet
- Percutaneous Nephrolithotomy (PCNL) : A. Interpreter / Cultural NeedsDocument3 pagesPercutaneous Nephrolithotomy (PCNL) : A. Interpreter / Cultural Needsvicentiu2003No ratings yet
- Paraphimosis Repair: Adult (18 Years and Over)Document3 pagesParaphimosis Repair: Adult (18 Years and Over)MADAGASCAR IDNo ratings yet
- Cardiac 13Document5 pagesCardiac 13Prince RaiNo ratings yet
- Leadless PPMDocument3 pagesLeadless PPMPenelope NorrisNo ratings yet
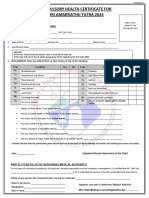
- Certificate of Physical Fitness: Personal DetailsDocument2 pagesCertificate of Physical Fitness: Personal DetailsVijay KumarNo ratings yet
- Template HXDocument1 pageTemplate HXdawnNo ratings yet
- Physical Fitness - Certificate 2022Document2 pagesPhysical Fitness - Certificate 2022Warrior SoulNo ratings yet
- Health FitnessDocument3 pagesHealth FitnessNo oneNo ratings yet
- Assessment Planning InterventionsDocument11 pagesAssessment Planning InterventionsKenrick BajaoNo ratings yet
- Purposes Only Download and Print: Antenatal AssessmentDocument2 pagesPurposes Only Download and Print: Antenatal AssessmentHadiyasa JatmikaNo ratings yet
- UST NSTP Medical Examination Report FormDocument1 pageUST NSTP Medical Examination Report FormFrancisQueNo ratings yet
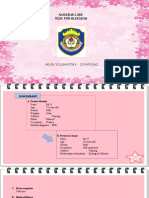
- Helen Yossrantika (2014901060) NCP Risk For BleedingDocument6 pagesHelen Yossrantika (2014901060) NCP Risk For BleedingGusmila SariNo ratings yet
- PhysicalFitness CertificateDocument2 pagesPhysicalFitness Certificatesoyamsidh dasNo ratings yet
- Risk NCP Eclampsia - PESCADERO 4CDocument1 pageRisk NCP Eclampsia - PESCADERO 4COrlando VillanuevaNo ratings yet
- Who Surgical Safety Checklist: Before Induction of Anesthesia Before Skin Incision Before Patient Leaves Operating RoomDocument1 pageWho Surgical Safety Checklist: Before Induction of Anesthesia Before Skin Incision Before Patient Leaves Operating RoomRpgmc Dr-nicuNo ratings yet
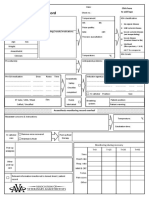
- University of South Florida College of Nursing: Fundamental Patient Assessment ToolDocument19 pagesUniversity of South Florida College of Nursing: Fundamental Patient Assessment Toolapi-418237167No ratings yet
- ISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüDocument23 pagesISU Ogrenci Klinik Uygulama Bakim Plani Degerlendirme DönüştürüldüMerve kdkkNo ratings yet
- History FormDocument5 pagesHistory FormYazeed AsrawiNo ratings yet
- JobsRegistrationDownloads File 1Document8 pagesJobsRegistrationDownloads File 1Amanda LaPointNo ratings yet
- Organ System Subjective Cues and Objective Cues Analysis InterpretationDocument3 pagesOrgan System Subjective Cues and Objective Cues Analysis InterpretationSeika SouiNo ratings yet
- Vsim - Edited Clinical WorksheetsDocument8 pagesVsim - Edited Clinical WorksheetsTedra FloydNo ratings yet
- Colorectal 06Document5 pagesColorectal 06Robertobosco BoscoNo ratings yet
- Attending Physician's Statement For Proposed Insured/OwnerDocument2 pagesAttending Physician's Statement For Proposed Insured/OwnerSincerely ReynNo ratings yet
- ACR Sample OntarioDocument5 pagesACR Sample OntarioAlisha PowerNo ratings yet
- Latihan MTK Un SMP BahasDocument2 pagesLatihan MTK Un SMP Bahasdinas pertanianNo ratings yet
- Individual Health ProfileDocument2 pagesIndividual Health ProfilendpNo ratings yet
- Pathophysiology A. Anatomy & Physiology: ReferenceDocument3 pagesPathophysiology A. Anatomy & Physiology: ReferenceAllana RayosNo ratings yet
- English CHCDocument1 pageEnglish CHCBhupi AgrawalNo ratings yet
- 200f MaDocument5 pages200f MaJerrica Charlene GalopeNo ratings yet
- A Nursing Care Plan Presented To The Faculty of The Nursing Department Karen Eve Mirafuentes, RNDocument12 pagesA Nursing Care Plan Presented To The Faculty of The Nursing Department Karen Eve Mirafuentes, RNRoel John Atamosa CasilacNo ratings yet
- Drug Study..Document2 pagesDrug Study..Ethan NamoNo ratings yet
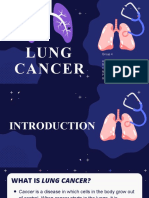
- Lung CancerDocument23 pagesLung CancerCristel Gervacio SumayanNo ratings yet
- Modern DermatologyDocument3 pagesModern DermatologySphoortiN XII B 927No ratings yet
- Understand and Prevent Stroke: What Is A Stroke? How To Prevent A Stroke The F.A.S.T. TestDocument7 pagesUnderstand and Prevent Stroke: What Is A Stroke? How To Prevent A Stroke The F.A.S.T. TestAidanNo ratings yet
- Rheumatic Heart DiseaseDocument21 pagesRheumatic Heart Diseasemedzmedina2No ratings yet
- Medical Certificate ProformaDocument2 pagesMedical Certificate ProformaAnulal .sNo ratings yet
- After I Lifted The Heavy Object, I Suddenly Felt A Pain in My Chest and I Am Also Experiencing of Difficulty in BreathingDocument8 pagesAfter I Lifted The Heavy Object, I Suddenly Felt A Pain in My Chest and I Am Also Experiencing of Difficulty in BreathingJulliza Joy PandiNo ratings yet
- AVA ASA Hi ElectronicDocument2 pagesAVA ASA Hi ElectronicJonathan ZapataNo ratings yet
- Onshore Pre Asses FormDocument6 pagesOnshore Pre Asses Formwendyphan09No ratings yet
- AdvancedSuggestionNeuroinduction 10284212Document419 pagesAdvancedSuggestionNeuroinduction 10284212jurebieNo ratings yet
- Catheter Laboratory Referral FormDocument1 pageCatheter Laboratory Referral FormMr ShoaiBiNo ratings yet
- Tgs Ibu Ellen 1Document11 pagesTgs Ibu Ellen 1rosna wallyNo ratings yet
- Assessmen T Diagnosi S Planning Intervention S Rational E Evaluatio NDocument3 pagesAssessmen T Diagnosi S Planning Intervention S Rational E Evaluatio Nmarie judimor gomezNo ratings yet
- Offshore Pre Asses FormDocument8 pagesOffshore Pre Asses Formwendyphan09No ratings yet
- CT Consent FormDocument3 pagesCT Consent FormAnonymous WXqKjTXMNo ratings yet
- Im Toledo Chestpain 110321Document14 pagesIm Toledo Chestpain 110321Vie TNo ratings yet
- CDC Wonder: The Vaccine Adverse Event Reporting System (VAERS) ResultsDocument339 pagesCDC Wonder: The Vaccine Adverse Event Reporting System (VAERS) ResultsMark LaceyNo ratings yet
- Drug Study Bryan P.Document5 pagesDrug Study Bryan P.Stephanie Dulay SierraNo ratings yet
- Nicholas Chung Ching Pui: Nursing Care PlanDocument3 pagesNicholas Chung Ching Pui: Nursing Care PlanMelDred Cajes BolandoNo ratings yet
- Assessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyDocument2 pagesAssessment Nursing Diagnosis Background Knowledge Goals of Care Intervention Rationale Evaluation Subjective: EpisiorraphyMaria Jessica DumdumNo ratings yet
- DDChest PainDocument3 pagesDDChest PainabbasifaiqNo ratings yet
- Aefi CifDocument6 pagesAefi CifVic KwanNo ratings yet
- Nursing Care Plan: Assessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationDocument6 pagesNursing Care Plan: Assessment Cues Nursing Diagnosis Desired Outcome Nursing Intervention Justification EvaluationPaul Gio OebandaNo ratings yet
- Burns: by Victoria S. Brioso-AngDocument33 pagesBurns: by Victoria S. Brioso-AngAmanda OsbornNo ratings yet
- Essentials of Radiofrequency Ablation of the Spine and JointsFrom EverandEssentials of Radiofrequency Ablation of the Spine and JointsNo ratings yet
- 09 Urinary Tract Infections in The ElderlyDocument19 pages09 Urinary Tract Infections in The Elderlypatel bhaumikNo ratings yet
- 4Q Mapeh 9 PTDocument2 pages4Q Mapeh 9 PTLouis MisolesNo ratings yet
- Year 4 PPT Paper 1 2018Document9 pagesYear 4 PPT Paper 1 2018Anonymous PYH3CmFNo ratings yet
- SuppressionDocument9 pagesSuppressiondharmishthavala41No ratings yet
- Muhammad Nauman (CV) ...Document3 pagesMuhammad Nauman (CV) ...SajidNo ratings yet
- Glomerular DiseaseDocument24 pagesGlomerular DiseasemadhuNo ratings yet
- Uv LightDocument5 pagesUv LightKingHungTingNo ratings yet
- The Policy Cycle PDFDocument11 pagesThe Policy Cycle PDFLauditta AchyaNo ratings yet
- Science Dept Ci TeamfinalDocument29 pagesScience Dept Ci TeamfinalEmely EstacioNo ratings yet
- Early Benefit Assessment EBA in Germany AnalysingDocument14 pagesEarly Benefit Assessment EBA in Germany AnalysingNeziha BEN ABDESSLEMNo ratings yet
- Group D Draft BookDocument53 pagesGroup D Draft BookmandyNo ratings yet
- Assignment 3 - David - Aaker's Ad Exposure Model - Vicks VaporubDocument10 pagesAssignment 3 - David - Aaker's Ad Exposure Model - Vicks VaporubHarish DunakheNo ratings yet
- Stemi ChecklistDocument1 pageStemi ChecklistDanu SusantoNo ratings yet
- National Guidelines For Lab Testing and Reporting On Resp Infectious Diseases Ghana - 2 PDFDocument18 pagesNational Guidelines For Lab Testing and Reporting On Resp Infectious Diseases Ghana - 2 PDFHenry OseiNo ratings yet
- Mauritius All-in-One Travel Digital FormDocument1 pageMauritius All-in-One Travel Digital FormANIL100% (1)
- Autism Spectrum Disorders: A Booklet For Parents and CarersDocument40 pagesAutism Spectrum Disorders: A Booklet For Parents and CarersAndreea SanduNo ratings yet
- Clinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewDocument2 pagesClinical Veterinary Advisor Dogs and Cats by Etienne Cote DVMDACVIMCardiology and Small Animal Internal Medicine - 5 Star ReviewMirsad Gilic0% (1)
- Internal Audit Risk AssessmentDocument2 pagesInternal Audit Risk AssessmentkhNo ratings yet
- Lesson 3 Primary Health Care and The Philippine Health Care Delivery System 1Document40 pagesLesson 3 Primary Health Care and The Philippine Health Care Delivery System 1Ritter GamingNo ratings yet
- Unit 5 Midterm MN566Document6 pagesUnit 5 Midterm MN566Jhouleen Angelika TamNo ratings yet
- Cashless Healthcare Benefit: Hamara Jawan AyushmanDocument2 pagesCashless Healthcare Benefit: Hamara Jawan AyushmanDipankar PatraNo ratings yet