You might also like
- Physical Therapy For Cardiopumonary DisordersDocument101 pagesPhysical Therapy For Cardiopumonary Disorderssunita_h100% (5)
- Respiratory Air Flow and VolumeDocument7 pagesRespiratory Air Flow and Volumeshwuyng91100% (3)
- Chronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDocument12 pagesChronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDiana Jalaynie S. SambolawanNo ratings yet
- Respiratory Physiology Adaptations To High-Level Exercise 2012Document5 pagesRespiratory Physiology Adaptations To High-Level Exercise 2012Maria GrigoreNo ratings yet
- Effectiveness of Diaphragmatic Stretching Versus Rib Stretching On Improving Pulmonary Function and Thoracic Excursion in Subjects With COPDDocument9 pagesEffectiveness of Diaphragmatic Stretching Versus Rib Stretching On Improving Pulmonary Function and Thoracic Excursion in Subjects With COPDInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cardiovascular Response To ExerciseDocument16 pagesCardiovascular Response To ExerciseEPMJrNo ratings yet
- Asthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDocument26 pagesAsthmatic Attack: Miriti M.D Masters of Clinical Medicine Accidents and Emergency Facilitator: DR Simba DR MburuguDennis MiritiNo ratings yet
- Wasserman Chest 1997Document13 pagesWasserman Chest 1997Filip BreskvarNo ratings yet
- Copd Case StudyDocument5 pagesCopd Case StudyJake Yvan DizonNo ratings yet
- Are Your Lungs HealthyDocument2 pagesAre Your Lungs HealthyGen Li TogyNo ratings yet
- BronchitisDocument15 pagesBronchitisAakanksha vaishnav100% (1)
- CPEx InterpretationDocument12 pagesCPEx InterpretationHolly JonesNo ratings yet
- POCKET GUIDE GOLD 2023 Ver 1.2 17feb2023 - WMVDocument55 pagesPOCKET GUIDE GOLD 2023 Ver 1.2 17feb2023 - WMVMARISOL FERNANDA GÓMEZNo ratings yet
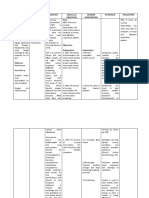
- Cues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalDocument4 pagesCues Nursing Diagnosis Analysis GOALS and Objectives Nursing Intervention Rationale Evaluation Subjective: GoalMonica Angelique SalayoNo ratings yet
- Intubation Set Equipment & FunctionsDocument4 pagesIntubation Set Equipment & FunctionsJrBong Semanero100% (1)
- UntitledDocument4 pagesUntitledRafsan HossainNo ratings yet
- Lab Report 4Document15 pagesLab Report 4api-273323485No ratings yet
- Lab 6 ReportDocument19 pagesLab 6 Reportapi-311215267100% (2)
- Respiratory Air Flow and Volume PDFDocument5 pagesRespiratory Air Flow and Volume PDFKim Robertson0% (1)
- Lab 5 397 2Document8 pagesLab 5 397 2api-568310444No ratings yet
- Copd Response of The Respiratory Muscles To Rehabilitation inDocument7 pagesCopd Response of The Respiratory Muscles To Rehabilitation inoanceaNo ratings yet
- Bio5 LabManual F19 1.0Document138 pagesBio5 LabManual F19 1.0Catherine BrennanNo ratings yet
- Exercise 15 - External RespirationDocument32 pagesExercise 15 - External RespirationAldrin LozanoNo ratings yet
- Ventilation increases during exercise to meet oxygen demandsDocument3 pagesVentilation increases during exercise to meet oxygen demandsErwan Sha HabinullahNo ratings yet
- Effects of A Balloon-Blowing Exercise On Lung Function of SmokersDocument4 pagesEffects of A Balloon-Blowing Exercise On Lung Function of SmokersMónica ReisNo ratings yet
- Pulmonary Function TestingDocument10 pagesPulmonary Function TestingSamman AftabNo ratings yet
- Clinical Study: Early Recovery of Exercise-Related Muscular Injury by HBOTDocument10 pagesClinical Study: Early Recovery of Exercise-Related Muscular Injury by HBOTVinnie Juliana YonatanNo ratings yet
- Impact of Fan Therapy During Exercise On Breathlessness and Recovery Time in Patients With COPD, A Pilot Randomised Controlled Crossover TrialDocument13 pagesImpact of Fan Therapy During Exercise On Breathlessness and Recovery Time in Patients With COPD, A Pilot Randomised Controlled Crossover TrialAmirudin ChonNo ratings yet
- Respiratory Physiology LecturesDocument37 pagesRespiratory Physiology LectureswiasonNo ratings yet
- 6211 PDFDocument7 pages6211 PDFDinilah AyuNo ratings yet
- Buceo ApneaDocument8 pagesBuceo ApneasurftraderNo ratings yet
- Exercise 7: Respiratory System Mechanics: Activity 1: Measuring Respiratory Volumes and Calculating Capacities Lab Pre-Lab Quiz ResultsDocument10 pagesExercise 7: Respiratory System Mechanics: Activity 1: Measuring Respiratory Volumes and Calculating Capacities Lab Pre-Lab Quiz ResultsNadila FaatinNo ratings yet
- Biology QuizDocument8 pagesBiology Quizkathy abreuNo ratings yet
- Physiological-Principles-of-Cardiopulmonary-Exercise-TestingDocument5 pagesPhysiological-Principles-of-Cardiopulmonary-Exercise-TestingNuno Vieira de Sousa Gomes LapaNo ratings yet
- Measuring Lung Capacity in Men and WomenDocument11 pagesMeasuring Lung Capacity in Men and WomenFatmawatiNo ratings yet
- Aerobic Training, Muscle Stretching Jurnal 2Document10 pagesAerobic Training, Muscle Stretching Jurnal 2Bunga Mitra MampuNo ratings yet
- Simple Exercises That Significantly IncrDocument29 pagesSimple Exercises That Significantly Incrsailesh singhNo ratings yet
- Measure Breathing & Heart Rates Before & After ExerciseDocument4 pagesMeasure Breathing & Heart Rates Before & After ExerciseRichard VemeNo ratings yet
- LungVolumeDocument24 pagesLungVolumeShalini Soorya100% (1)
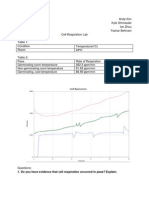
- Cell Respiration Lab Shows Effect of Temperature on Pea Germination RateDocument6 pagesCell Respiration Lab Shows Effect of Temperature on Pea Germination Rateianzhou1No ratings yet
- LAB ActivityDocument2 pagesLAB ActivityNicole AquinoNo ratings yet
- (Osborn) Chapter 19: Learning Outcomes (Number and Title)Document28 pages(Osborn) Chapter 19: Learning Outcomes (Number and Title)Kitties100% (1)
- Disability Evaluation Under Social Security 3.00 Respiratory Disorders - AdultDocument24 pagesDisability Evaluation Under Social Security 3.00 Respiratory Disorders - Adultsfinx100007696No ratings yet
- As PE Lesson 27 Resp Syst 2013-14Document13 pagesAs PE Lesson 27 Resp Syst 2013-14mancollNo ratings yet
- Module 1 Mechanical VentilationDocument13 pagesModule 1 Mechanical VentilationMinutes in MEDITATIONNo ratings yet
- Emsp 1355 !!! Co2Document17 pagesEmsp 1355 !!! Co2acctsacctsNo ratings yet
- Ejercicio DiafragmaticoDocument3 pagesEjercicio DiafragmaticoN onlyNo ratings yet
- Unit 7 Blood PressureDocument11 pagesUnit 7 Blood PressureQ O R Y A N INo ratings yet
- Heart-2007-Albouaini-1285-92 - Cardiopulmonary Exercise Testing and Its ApplicationDocument9 pagesHeart-2007-Albouaini-1285-92 - Cardiopulmonary Exercise Testing and Its Application徐振瑋No ratings yet
- Expt. 26 Lung Volumes and Capacities (A)Document5 pagesExpt. 26 Lung Volumes and Capacities (A)api-3769252100% (2)
- ReportDocument7 pagesReportThomas Yeung100% (1)
- BUTEYKO'S METHOD OF VOLITIONAL CONTROL OF BREATHINGDocument27 pagesBUTEYKO'S METHOD OF VOLITIONAL CONTROL OF BREATHINGOmmachineNo ratings yet
- 51456-Respiration-23086215D-Cheung-Chi-MingDocument5 pages51456-Respiration-23086215D-Cheung-Chi-Ming9rw9yrh6qyNo ratings yet
- Mechanical VentilationDocument13 pagesMechanical VentilationNithiya NadesanNo ratings yet
- Bio 142 Exercise Physiology Lab ReportDocument11 pagesBio 142 Exercise Physiology Lab Reportapi-34160259975% (4)
- Efficiency LabDocument3 pagesEfficiency LabsicklidboiNo ratings yet
- Exercise LabDocument3 pagesExercise LabJonatan LeflerNo ratings yet
- Activity 2.2.1b_ Oxygen _ Human RespirationDocument4 pagesActivity 2.2.1b_ Oxygen _ Human RespirationVictoria WarrenNo ratings yet
- Jurnal COPDDocument8 pagesJurnal COPDAyahnya RafliNo ratings yet
- Bronchitis: Edited by Ignacio Martín-LoechesDocument200 pagesBronchitis: Edited by Ignacio Martín-LoechesskilmagNo ratings yet
- E Static Lung Volumes and CapacitiesDocument5 pagesE Static Lung Volumes and CapacitiesAyeNo ratings yet
- Lectures 54 and 55 Phys Integration LOsDocument4 pagesLectures 54 and 55 Phys Integration LOsAndrew SagalovNo ratings yet
- FT Kardiorespirasi - CompressedDocument101 pagesFT Kardiorespirasi - CompressedWahdina PratamaNo ratings yet
- SCIENTIFIC BASIS OF HUMAN MOVEMENT EFFECTS OF EXERCISE ON RESPIRATORY SYSTEM - Wbshce PDFDocument9 pagesSCIENTIFIC BASIS OF HUMAN MOVEMENT EFFECTS OF EXERCISE ON RESPIRATORY SYSTEM - Wbshce PDFlancetNo ratings yet
- Zoology II (Em) BLM 21-22Document99 pagesZoology II (Em) BLM 21-22GANESH KANDAGATLANo ratings yet
- Activity 17 The Respiratory System and Pulmonary VentilationDocument5 pagesActivity 17 The Respiratory System and Pulmonary VentilationarmandNo ratings yet
- Journal 2Document8 pagesJournal 2Claudia JessicaNo ratings yet
- Respiratory Disease Anatomy and Phys Sheridan CollegeDocument7 pagesRespiratory Disease Anatomy and Phys Sheridan CollegeAudrey AndinoNo ratings yet
- Psychosomatic Theory of Bronchia AsthmaDocument11 pagesPsychosomatic Theory of Bronchia AsthmaMaria RiveraNo ratings yet
- Week 2 Assignment 2Document7 pagesWeek 2 Assignment 2Samantha PargadNo ratings yet
- Nursing Care Plan Profile: M.B (20 Yrs Old) Allergic RhinitisDocument1 pageNursing Care Plan Profile: M.B (20 Yrs Old) Allergic RhinitisMeccanazaren Susvilla Bojorque100% (1)
- Silverman Anderson IndexDocument2 pagesSilverman Anderson IndexMark Jaco AngNo ratings yet
- ECRI Test ResultsDocument3 pagesECRI Test ResultsAdam HarringtonNo ratings yet
- Review The Causes of Decreased Breath SoundsDocument1 pageReview The Causes of Decreased Breath SoundsArvinth Guna SegaranNo ratings yet
- Dust Can Kill: Raising Awareness To Protect LivesDocument3 pagesDust Can Kill: Raising Awareness To Protect LivesAmit RNo ratings yet
- Pulmonary Function Tests: Dr. Pooja ChopraDocument91 pagesPulmonary Function Tests: Dr. Pooja ChopraabbuahmedibbuNo ratings yet
- ICU Ventilator SpecificationsDocument2 pagesICU Ventilator Specificationsfirman laoweNo ratings yet
- HW1Document2 pagesHW1Bug AphidNo ratings yet
- Assessment Diagnosis Planning Intervention Evaluation for Impaired Gas ExchangeDocument2 pagesAssessment Diagnosis Planning Intervention Evaluation for Impaired Gas ExchangeCharissa Magistrado De LeonNo ratings yet
- Clustered Data Nursing Diagnosis (Diagnostic Label) PriorityDocument4 pagesClustered Data Nursing Diagnosis (Diagnostic Label) PriorityRoger ViloNo ratings yet
- Safety Data Sheet: 1. IdentificationDocument8 pagesSafety Data Sheet: 1. IdentificationIrvin CervantesNo ratings yet
- Chapter One: 1.4.1 General ObjectiveDocument3 pagesChapter One: 1.4.1 General ObjectivejohnNo ratings yet
- Concept Map RSV 4Document10 pagesConcept Map RSV 4api-546577761No ratings yet
- Self Reporting Form Details For International Arriving PassengersDocument2 pagesSelf Reporting Form Details For International Arriving Passengersbhupathyraju100% (1)
- Seroflo 250 Synchrobreathe - View Uses, Side Effects, Price and Substitutes - 1mgDocument10 pagesSeroflo 250 Synchrobreathe - View Uses, Side Effects, Price and Substitutes - 1mgParteek SinglaNo ratings yet
- Respiratory Assessment Guide for NursesDocument12 pagesRespiratory Assessment Guide for NursesDhen Marc0% (1)
- Hurry Cases, Signs of A Heart Attack, Rescue Breathing and CPRDocument2 pagesHurry Cases, Signs of A Heart Attack, Rescue Breathing and CPRgit pupNo ratings yet
- 1 - Spirometry Simplified With CRF's PEFR PDFDocument80 pages1 - Spirometry Simplified With CRF's PEFR PDFyayatiNo ratings yet
- Lazarte - Status AsthmaticusDocument5 pagesLazarte - Status AsthmaticusArvin LazarteNo ratings yet