You might also like
- CASE PRESENTATION ON UTI Case 3Document14 pagesCASE PRESENTATION ON UTI Case 3Safoora RafeeqNo ratings yet
- Beyond Talk Therapy Using Movement and Expressive Techniques in Clinical Practice PDFDocument308 pagesBeyond Talk Therapy Using Movement and Expressive Techniques in Clinical Practice PDFSiyao LiNo ratings yet
- UTI TreatmentDocument3 pagesUTI TreatmentMaria RezitadinaNo ratings yet
- UTI Treatment Algorithm - Sharp Mesa Vista 2Document3 pagesUTI Treatment Algorithm - Sharp Mesa Vista 2Fitri 1997No ratings yet
- Làm Gì Khi SDMA TăngDocument1 pageLàm Gì Khi SDMA TăngNguyễn Tấn TàiNo ratings yet
- How Can You Help Your Patients With An Uncomplicated UTI?: Know?Document1 pageHow Can You Help Your Patients With An Uncomplicated UTI?: Know?gegeNo ratings yet
- Algoritmo Peritoneal EffusionDocument2 pagesAlgoritmo Peritoneal EffusionJuliana Torres GarciaNo ratings yet
- finalsURINARY ELIMINATION DIAGNOSTICSDocument11 pagesfinalsURINARY ELIMINATION DIAGNOSTICSFrances LiqueNo ratings yet
- Guidelines Ut I 2012Document1 pageGuidelines Ut I 2012Siti ZulaikhahNo ratings yet
- Algorith UTI 20121218 PDFDocument1 pageAlgorith UTI 20121218 PDFIin fermitaNo ratings yet
- Pharmacotherapy of UTI and STDDocument36 pagesPharmacotherapy of UTI and STDDr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Syndromic Management of StiDocument46 pagesSyndromic Management of StiJeeban Jyoti MishraNo ratings yet
- Managing LUTS BPH For Patients at Risk of Progression - DR RickyDocument37 pagesManaging LUTS BPH For Patients at Risk of Progression - DR RickyafifberlianNo ratings yet
- Urological RefferalDocument12 pagesUrological Refferalmichelle octavianiNo ratings yet
- MS 2Document8 pagesMS 2Vincent AmitNo ratings yet
- UrolithiasisDocument9 pagesUrolithiasisJessa MaeNo ratings yet
- CDN 2Document8 pagesCDN 2Steph NuñezNo ratings yet
- PPT Case NephrolithiasisDocument45 pagesPPT Case NephrolithiasisRifka Anisa0% (1)
- Final OSCEs CollectionDocument2 pagesFinal OSCEs Collections129682No ratings yet
- Uti, Rheumatic Fever & ArthritisDocument2 pagesUti, Rheumatic Fever & ArthritisKM PanganibanNo ratings yet
- Naproxen Drug StudyDocument4 pagesNaproxen Drug StudyTimz GatdulaNo ratings yet
- Uti PDFDocument1 pageUti PDFKurouSakiNo ratings yet
- Hematology B Bleeding and Cancer PDFDocument143 pagesHematology B Bleeding and Cancer PDFMark Samuel TanchocoNo ratings yet
- Isk BSKDocument5 pagesIsk BSKAndy F MonroeNo ratings yet
- Pharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009Document12 pagesPharmaco Logy Imm Une Syste M Drugs: Julia Leonor Huaringa Lagomarsino, RN February 13, 2009julialeoNo ratings yet
- ITU RO Dr. Vlad Cristiana 2020Document55 pagesITU RO Dr. Vlad Cristiana 2020Mădălina Mihaela LuchianNo ratings yet
- Acute AUBDocument9 pagesAcute AUBJessa MaeNo ratings yet
- Emergency Case Report December 14 - 15 2021Document17 pagesEmergency Case Report December 14 - 15 2021harisNo ratings yet
- Rheumatology SBIM Part 1Document5 pagesRheumatology SBIM Part 1Gousay AlkhazmariNo ratings yet
- 3 Antitubercular Therapy Hepatitis 18032022Document1 page3 Antitubercular Therapy Hepatitis 18032022Nido MalghaniNo ratings yet
- Continence Problem at HomeDocument71 pagesContinence Problem at HomeZayar HmunNo ratings yet
- First Line of DrugsDocument5 pagesFirst Line of DrugsBiancaGabatinoAbarcaNo ratings yet
- Fin DRUG STUDYDocument4 pagesFin DRUG STUDYKc AcainNo ratings yet
- Drug Study CISPLATINDocument2 pagesDrug Study CISPLATINCorrine IvyNo ratings yet
- CPG Bite StingsDocument10 pagesCPG Bite StingsMarvin M PulaoNo ratings yet
- Kidney FailureDocument4 pagesKidney FailureAslimah RakimNo ratings yet
- McEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFDocument2 pagesMcEntee, Asst Prof Laurence Lower Back Pain A4 301120 PDFRamesh SinghNo ratings yet
- Metronidazole HydrochlorideDocument2 pagesMetronidazole HydrochlorideSTORAGE FILENo ratings yet
- Overactivebladder 160426102342Document53 pagesOveractivebladder 160426102342Tô Hoàng DũngNo ratings yet
- Fluid and ElectrolytesDocument21 pagesFluid and ElectrolytesKc Cabanilla LizardoNo ratings yet
- Hand Pathway 4Document7 pagesHand Pathway 4api-163168129No ratings yet
- Home Care RN Skills ChecklistDocument2 pagesHome Care RN Skills ChecklistGloryJaneNo ratings yet
- ch2 fs1Document2 pagesch2 fs1ry beNo ratings yet
- Drug Study (Romel) Feb 1&2 - Ventura PDFDocument4 pagesDrug Study (Romel) Feb 1&2 - Ventura PDFJian VenturaNo ratings yet
- Abdominal PainDocument3 pagesAbdominal PainNoor AlblushiNo ratings yet
- Department of Internal Medicine Iii: - Vanaveerapandian Swetha GROUP 415 B' Subgroup "15"Document51 pagesDepartment of Internal Medicine Iii: - Vanaveerapandian Swetha GROUP 415 B' Subgroup "15"Suba Saravanan 12No ratings yet
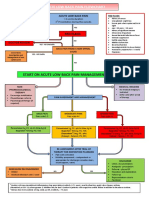
- Acute Low Back Pain Flowchart March 2016Document1 pageAcute Low Back Pain Flowchart March 2016Alfiya HasnaNo ratings yet
- Gyna Short 4Document2 pagesGyna Short 4ahmed naeemNo ratings yet
- Urinary Tract Infections in Children 2021Document19 pagesUrinary Tract Infections in Children 2021azri.hafiziNo ratings yet
- Ptyalism & Pseudoptyalism - Allen, JulieDocument2 pagesPtyalism & Pseudoptyalism - Allen, JulieJuanMartínezNo ratings yet
- Notes On UtiDocument15 pagesNotes On UtiSaleh Mohammad ShoaibNo ratings yet
- Surgical - Floor RequirementDocument8 pagesSurgical - Floor RequirementPureza Maye SalapangNo ratings yet
- Insignis Pedia Red Flags of Renal DiseasesDocument4 pagesInsignis Pedia Red Flags of Renal DiseasesBinod Kumar SahNo ratings yet
- PharmacologyDocument4 pagesPharmacologyEmmanuel CuevasNo ratings yet
- Assignment On Week 3Document6 pagesAssignment On Week 3Samantha PargadNo ratings yet
- Pediatric Genitourinary DisordersDocument40 pagesPediatric Genitourinary DisordersGelsey Gelsinator JianNo ratings yet
- Philippine Urological Association, Inc.: Executive Committee and Board Members 1997Document12 pagesPhilippine Urological Association, Inc.: Executive Committee and Board Members 1997mits98No ratings yet
- MS 2Document9 pagesMS 2Vincent AmitNo ratings yet
- OSCEs For Medical Finals RectalDocument3 pagesOSCEs For Medical Finals Rectalss123sNo ratings yet
- The Ultimate Chronic Kidney Disease Diet Cookbook; The Complete Nutrition Guide To Restoring The Health Of Your Kidney With Meal Plan And Nourishing RecipesFrom EverandThe Ultimate Chronic Kidney Disease Diet Cookbook; The Complete Nutrition Guide To Restoring The Health Of Your Kidney With Meal Plan And Nourishing RecipesNo ratings yet
- The Ideal Dialysis Diet Cookbook; The Superb Diet Guide To Managing Kidney Problems And Soothing Dialysis With Nutritious Low Sodium Low Potassium RecipesFrom EverandThe Ideal Dialysis Diet Cookbook; The Superb Diet Guide To Managing Kidney Problems And Soothing Dialysis With Nutritious Low Sodium Low Potassium RecipesNo ratings yet
- Biography DRDocument3 pagesBiography DRFitriani AzizNo ratings yet
- Mapeh IDocument10 pagesMapeh IjenilynNo ratings yet
- Lesson 1 - Proper Handwashing TechniqueDocument1 pageLesson 1 - Proper Handwashing TechniqueIdk UlitNo ratings yet
- Innate HealingDocument14 pagesInnate HealingDrThangaraj KNo ratings yet
- Results of HSRC Study On South African Healthcare Workers Mental Health and Covid 19Document64 pagesResults of HSRC Study On South African Healthcare Workers Mental Health and Covid 19Laura Lopez GonzalezNo ratings yet
- KH!Winter!Challenge!-!Weeks!1&5: Workout 1-Legs, Calves, CardioDocument4 pagesKH!Winter!Challenge!-!Weeks!1&5: Workout 1-Legs, Calves, CardioJessika CastilloNo ratings yet
- Study PlanDocument1 pageStudy PlanNobby MonicaNo ratings yet
- Introduction of Dance: Learning OutcomesDocument93 pagesIntroduction of Dance: Learning OutcomesLala BubNo ratings yet
- Thematic AnalysisDocument12 pagesThematic AnalysisFlorence Roselle Rejuso UdasNo ratings yet
- Role Purpose of Role: Role Profile INVIGILATOR InvigilatorDocument3 pagesRole Purpose of Role: Role Profile INVIGILATOR Invigilatorernest libertyNo ratings yet
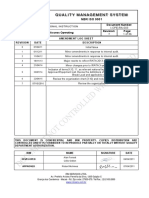
- I-OPE-RA-003 - Rope Access Operating - Rev.7 (Em Revisao)Document36 pagesI-OPE-RA-003 - Rope Access Operating - Rev.7 (Em Revisao)Rael Zorzo MichelsNo ratings yet
- Universidad El Bosque: Taller de Biología Celular Y MolecularDocument4 pagesUniversidad El Bosque: Taller de Biología Celular Y MolecularNikol ParraNo ratings yet
- Unit 6 Concet of EliminationDocument32 pagesUnit 6 Concet of EliminationAbdur Rehman100% (1)
- 2022 - Digital Medicine - Evaluation of An Artificial Intelligence-Based Medical Device For Diagnosis of Autism Spectrum DisorderDocument11 pages2022 - Digital Medicine - Evaluation of An Artificial Intelligence-Based Medical Device For Diagnosis of Autism Spectrum DisorderNeraLogoNo ratings yet
- IT Audit ExerciseDocument1 pageIT Audit ExercisewirdinaNo ratings yet
- MSDS MEGAFLOC 515 Revisi OkDocument5 pagesMSDS MEGAFLOC 515 Revisi OkYafie Al IslamiNo ratings yet
- PA - Coursepack DAY 1Document352 pagesPA - Coursepack DAY 1Elly NuñezNo ratings yet
- Voice Over ScriptDocument4 pagesVoice Over ScriptJESSIE DAUG100% (1)
- Competency No. of ItemsDocument9 pagesCompetency No. of ItemsNorielee MartinNo ratings yet
- HRM656 Work Life BalanceDocument24 pagesHRM656 Work Life Balance2021485676No ratings yet
- ME14 1329 Maintenance Management: Workbook 2: Failure CharacteristicsDocument16 pagesME14 1329 Maintenance Management: Workbook 2: Failure CharacteristicsjamalNo ratings yet
- Abtracts Effects of Divorce On ChildrenDocument7 pagesAbtracts Effects of Divorce On ChildrenJoshua AjimNo ratings yet
- Professional Disclosure StatementDocument3 pagesProfessional Disclosure Statementapi-642170591No ratings yet
- Kolehiyo NG Lungsod NG Lipa: College of Teacher EducationDocument4 pagesKolehiyo NG Lungsod NG Lipa: College of Teacher EducationHeeseung LeeNo ratings yet
- 2022 Tool For Best Be ImplementersDocument10 pages2022 Tool For Best Be ImplementersALJERR LAXAMANANo ratings yet
- Mike Brown Complete Autopsy ReportDocument16 pagesMike Brown Complete Autopsy ReportDiana StakeyNo ratings yet
- Abebe Yilma - 2Document127 pagesAbebe Yilma - 2Robiya OrumbekovaNo ratings yet
- PL4243 Intellectual Developmental Disability OutlineDocument9 pagesPL4243 Intellectual Developmental Disability OutlineKura ChingNo ratings yet
- 2020-10-07-Student Learning ContractDocument3 pages2020-10-07-Student Learning ContractJJAMPPONG PSNo ratings yet