You might also like
- Article in Press: Orthopaedics & Traumatology: Surgery & ResearchDocument6 pagesArticle in Press: Orthopaedics & Traumatology: Surgery & ResearchAren BizdikianNo ratings yet
- Does Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyDocument6 pagesDoes Use of A Variable Distal Femur Resection Angle Improve Radiographic Alignment in Primary Total Knee ArthroplastyAsmed El SalugNo ratings yet
- A New Approach To Determining The Hip Rotation Profile From Clinical Gait Analysis DataDocument20 pagesA New Approach To Determining The Hip Rotation Profile From Clinical Gait Analysis Datachacho1971No ratings yet
- A Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringDocument7 pagesA Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringEzgi PelitNo ratings yet
- Three-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsDocument8 pagesThree-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsFayza RihastaraNo ratings yet
- Journal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. AminianDocument6 pagesJournal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. Aminianconstantinescuana200No ratings yet
- PIIS08Document8 pagesPIIS08Ahmad Ibrahim SalemNo ratings yet
- Manual TherapyDocument10 pagesManual Therapyubiktrash1492No ratings yet
- Kinematic Analysis of A Six-Degree-Of-Freedom Model Based On ISB Recommendation A Repeatability Analysis and Comparison With Convetional Gait ModelDocument9 pagesKinematic Analysis of A Six-Degree-Of-Freedom Model Based On ISB Recommendation A Repeatability Analysis and Comparison With Convetional Gait ModelLaura VNo ratings yet
- Sagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsDocument5 pagesSagittal Spine Posture Assessment: Feasibility of A Protocol Based On Intersegmental MomentsVizaNo ratings yet
- J - A Clinico-Radiographic AnalysisDocument34 pagesJ - A Clinico-Radiographic AnalysisSusovan GiriNo ratings yet
- Between Session Reliability of Opto Electronic Motion Capture - 2018 - Journal oDocument5 pagesBetween Session Reliability of Opto Electronic Motion Capture - 2018 - Journal oRyuNo ratings yet
- Measurement of Pelvic Orientation Angles During Sprinting Using A Single Inertial SensorDocument6 pagesMeasurement of Pelvic Orientation Angles During Sprinting Using A Single Inertial SensorMonikaNo ratings yet
- Jurnal 5Document7 pagesJurnal 5JAQUELINENo ratings yet
- Gait AnalysisDocument3 pagesGait AnalysisVinay KumarNo ratings yet
- Automatic Tracking Measurement System On Human Lumbar Vertebral MotionDocument4 pagesAutomatic Tracking Measurement System On Human Lumbar Vertebral MotionebrahimpanNo ratings yet
- 10 1016@j Joca 2006 02 024Document7 pages10 1016@j Joca 2006 02 024Roman PopescuNo ratings yet
- Gait & Posture: Full Length ArticleDocument7 pagesGait & Posture: Full Length ArticleMKNo ratings yet
- Dynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsDocument7 pagesDynamic Measurement of Lumbar Curvature Using Fibre-Optic SensorsebrahimpanNo ratings yet
- Gait & Posture: William Samson, Stéphane Sanchez, Patrick Salvia, Serge Van Sint Jan, Véronique FeipelDocument9 pagesGait & Posture: William Samson, Stéphane Sanchez, Patrick Salvia, Serge Van Sint Jan, Véronique FeipelAarsyid Aldi PratamaNo ratings yet
- 1 s2.0 S0021929015001931 MainDocument7 pages1 s2.0 S0021929015001931 MainceliaNo ratings yet
- Asaeda 2018Document5 pagesAsaeda 2018alonsoNo ratings yet
- Transverso Do Abdomen e Movimentos Dos Membros1Document5 pagesTransverso Do Abdomen e Movimentos Dos Membros1jordandorrNo ratings yet
- Classifying Alpha AngleDocument10 pagesClassifying Alpha AngleAlberto MedinNo ratings yet
- Orthopaedics & Traumatology: Surgery & ResearchDocument7 pagesOrthopaedics & Traumatology: Surgery & ResearchMohan DesaiNo ratings yet
- 3D Motion Reliability of Occipital Condylar Glide Testing From ConceptDocument6 pages3D Motion Reliability of Occipital Condylar Glide Testing From ConceptGustavo Adolfo GarciaNo ratings yet
- 02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsDocument6 pages02 - Biomechanical Analysis of Sit-To-stand Movement in Normal and Obese SubjectsCristian HuequelefNo ratings yet
- Salem 201Document6 pagesSalem 201mikelNo ratings yet
- Andriacchi 1998 PCTDocument7 pagesAndriacchi 1998 PCTdanasolav1798No ratings yet
- 1 s2.0 S0021929020304681 MainDocument7 pages1 s2.0 S0021929020304681 MainSamanta EgañaNo ratings yet
- Accuracy of Planar Anteversion THADocument8 pagesAccuracy of Planar Anteversion THAManny TantorNo ratings yet
- Sicotj 8 34Document5 pagesSicotj 8 34robertoNo ratings yet
- Ravi Et Al 2021 Comparison of Roll and Pitch Among Patients With Vertical and Horizontal Skeletal Patterns Using Cant oDocument4 pagesRavi Et Al 2021 Comparison of Roll and Pitch Among Patients With Vertical and Horizontal Skeletal Patterns Using Cant oPulkit BimalNo ratings yet
- Wade Et Al 2020Document4 pagesWade Et Al 2020Christos TheodorakisNo ratings yet
- ISB Recommendation On Definitions of Joint Coordinate Systems of Various Joints For The Reporting of Human Joint Motion - Part II Shoulder, Elbow, Wrist and HandDocument12 pagesISB Recommendation On Definitions of Joint Coordinate Systems of Various Joints For The Reporting of Human Joint Motion - Part II Shoulder, Elbow, Wrist and HandAnonymous YePlm1vHz7No ratings yet
- Reliability and Validity of A Clinical Assessment Tool For Measuring Scapular Motion in All 3 Anatomical PlanesDocument8 pagesReliability and Validity of A Clinical Assessment Tool For Measuring Scapular Motion in All 3 Anatomical PlanesAronNo ratings yet
- Koop Man 2014Document12 pagesKoop Man 2014Elizabeth CominaNo ratings yet
- Radiographic Measurements On Hindfoot Alignment View in - 2021 - Foot and AnkleDocument5 pagesRadiographic Measurements On Hindfoot Alignment View in - 2021 - Foot and Anklexbyhz759g7No ratings yet
- ICORR 2011 Revised v7Document6 pagesICORR 2011 Revised v7Luu Trieu PhatNo ratings yet
- Effect of Meniscal Loss On Knee Stability After Single-Bundle Anterior Cruciate Ligament ReconstructionDocument9 pagesEffect of Meniscal Loss On Knee Stability After Single-Bundle Anterior Cruciate Ligament Reconstructioni_anitaNo ratings yet
- Nüesch 2017Document24 pagesNüesch 2017AFoqsdifNo ratings yet
- Tannast 2005Document7 pagesTannast 2005Santiago CeliNo ratings yet
- Accuracy of EOS Imagining Technology in Comparison.94031Document18 pagesAccuracy of EOS Imagining Technology in Comparison.94031Mohammad KaramNo ratings yet
- Unit 1.4Document5 pagesUnit 1.4jayanthikNo ratings yet
- Recording Condylar Guidance: Are We Getting It?: January 2017Document9 pagesRecording Condylar Guidance: Are We Getting It?: January 2017Shraddha AgarwalNo ratings yet
- Effects of Locomotion Mode Recognition Errors On Volitional Control of Powered Above-Knee ProsthesesDocument9 pagesEffects of Locomotion Mode Recognition Errors On Volitional Control of Powered Above-Knee ProsthesesjuanNo ratings yet
- Foot Type Classification Using Sensor-Enabled FootwearDocument12 pagesFoot Type Classification Using Sensor-Enabled FootwearDio Alif HutamaNo ratings yet
- Cardan AnglesDocument8 pagesCardan Anglesangelicamaria_647609No ratings yet
- X-Ray: Correlation Study Between Cervical X-Ray Sagittal Parameters and Chuna Posture Analysis ResultsDocument13 pagesX-Ray: Correlation Study Between Cervical X-Ray Sagittal Parameters and Chuna Posture Analysis Resultskang soon cheolNo ratings yet
- Journal of BiomechanicsDocument10 pagesJournal of Biomechanicsع الNo ratings yet
- MRI-derived Moment-Arms of The Female and Male Spine Loading MusclesDocument12 pagesMRI-derived Moment-Arms of The Female and Male Spine Loading Muscleshamid_nnbeNo ratings yet
- Approach To The Perpendicular Fixation of A Scaphoid Waist Fracture-A Computer Analyzed Cadaver ModelDocument10 pagesApproach To The Perpendicular Fixation of A Scaphoid Waist Fracture-A Computer Analyzed Cadaver ModelantoanetaNo ratings yet
- Paper Taping en HombroDocument6 pagesPaper Taping en HombroCarolina Leiva NeiraNo ratings yet
- A Simple Method For Accurate Rotational Positioning of The Femoral Component in Total Knee ArthroplastDocument8 pagesA Simple Method For Accurate Rotational Positioning of The Femoral Component in Total Knee ArthroplastShivamNo ratings yet
- An Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningDocument7 pagesAn Automated Pelvic Bone Geometrical Feature Measurement Utilities On CT ScanningInternational Organization of Scientific Research (IOSR)No ratings yet
- Ahn 2015Document6 pagesAhn 2015fabian hernandez medinaNo ratings yet
- Initial Biomechanical Analysis and Modeling of Transfemoral Amputee GaitDocument7 pagesInitial Biomechanical Analysis and Modeling of Transfemoral Amputee GaitAshwini Kumar BaluguriNo ratings yet
- Assessment of Radial Torsion Using Computed Tomography in Dogs With and Without Antebrachial Limb DeformityDocument8 pagesAssessment of Radial Torsion Using Computed Tomography in Dogs With and Without Antebrachial Limb DeformityNathaly DejoyNo ratings yet
- Patterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Document7 pagesPatterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Patrik NazarioNo ratings yet
- Euclidean and Non Euclidean Geometries Development and History PDFDocument2 pagesEuclidean and Non Euclidean Geometries Development and History PDFMelissaNo ratings yet
- An Efficient Color Quantization Using Color HistogramDocument5 pagesAn Efficient Color Quantization Using Color HistogramAndre SetiawanNo ratings yet
- Automatically allocate planned and actual indirect activities using keysDocument4 pagesAutomatically allocate planned and actual indirect activities using keysSudharsan PonnambalamNo ratings yet
- Diction Exercises For 'B' WordsDocument4 pagesDiction Exercises For 'B' WordsBianca ConstantinNo ratings yet
- Mse 221 Final ReviewDocument8 pagesMse 221 Final ReviewnmfreedomNo ratings yet
- Factor Analysis To Evaluate Hospital ResilienceDocument7 pagesFactor Analysis To Evaluate Hospital ResiliencecemadaroNo ratings yet
- Computational MHDDocument66 pagesComputational MHDverthex20992828No ratings yet
- Multiple RegressionDocument30 pagesMultiple Regressionjagdip_barikNo ratings yet
- Aurelio BaldorDocument1 pageAurelio BaldorAnonymous vcdqCTtS9No ratings yet
- Find the equation of a parabola given its focus and directrixDocument1 pageFind the equation of a parabola given its focus and directrixpeteNo ratings yet
- Handbook On Dress and Cloak Cutting 1884Document68 pagesHandbook On Dress and Cloak Cutting 1884linNo ratings yet
- Selecting Tube Inserts For Shell-and-Tube Heat ExchangersDocument7 pagesSelecting Tube Inserts For Shell-and-Tube Heat Exchangerskamranonline999No ratings yet
- Hungarian Method ExplainedDocument2 pagesHungarian Method ExplainedJosé Luis VelázquezNo ratings yet
- Pulse Code Modulation (Sampling, Quantizing, Encoding)Document21 pagesPulse Code Modulation (Sampling, Quantizing, Encoding)Jayan Kulathoor100% (1)
- DynamicsDocument8 pagesDynamicsLaud FumhandaNo ratings yet
- Standard VHDL PackagesDocument2 pagesStandard VHDL PackagesSundar RajanNo ratings yet
- Composite Optimisation of A Formula One Front WingDocument10 pagesComposite Optimisation of A Formula One Front WingaerostressNo ratings yet
- Allen: Pre-Nurture CourseDocument3 pagesAllen: Pre-Nurture CourseAshrithNo ratings yet
- Icsis 2022 Face MorphingDocument10 pagesIcsis 2022 Face MorphingprashantrinkuNo ratings yet
- Outline of DegreeDocument277 pagesOutline of Degreewarda irfanNo ratings yet
- Analysis of Multi-Layered Filament-Wound Composite Pipes Under Combined Internal Pressure and Thermomechanical Loading With Thermal VariationsDocument10 pagesAnalysis of Multi-Layered Filament-Wound Composite Pipes Under Combined Internal Pressure and Thermomechanical Loading With Thermal VariationsAhmed HassanNo ratings yet
- HG Properties Table 2016 PDFDocument19 pagesHG Properties Table 2016 PDFMario LeonoNo ratings yet
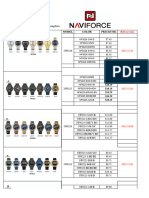
- NAVIFORCE Watch Catalogue in USD - Updated in 20240104Document47 pagesNAVIFORCE Watch Catalogue in USD - Updated in 20240104Perez PerezNo ratings yet
- Evaluation of SAR Reduction For Mobile Phone Using RF ShieldDocument5 pagesEvaluation of SAR Reduction For Mobile Phone Using RF ShieldsubuhpramonoNo ratings yet
- BCA 4th Sem. Asst. 2018-19Document15 pagesBCA 4th Sem. Asst. 2018-19Kumar InfoNo ratings yet
- FS@Document9 pagesFS@Nidhie ✫ SinghNo ratings yet
- 91985v00 Mazda User Story FinalDocument2 pages91985v00 Mazda User Story Finalopek161No ratings yet
- Performance Evaluation of Air Conditioner Using Earth Air Tunnel Heat ExchangerDocument5 pagesPerformance Evaluation of Air Conditioner Using Earth Air Tunnel Heat ExchangerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Science of Tone-Color: Exploring the Relationship Between Sound and LightDocument105 pagesThe Science of Tone-Color: Exploring the Relationship Between Sound and LightXeropointNo ratings yet
- Torque Equation of Three Phase Induction Motor - Electrical4UDocument14 pagesTorque Equation of Three Phase Induction Motor - Electrical4Ukaustav choudhuryNo ratings yet