You might also like
- Otorhinolaryngology NotesDocument25 pagesOtorhinolaryngology NotesFako Filipinas100% (3)
- Classroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)Document6 pagesClassroom Instruction Delivery Alignment Map General Biology 1 Grade 11 (STEM)JunedelMirallesPerez50% (2)
- Pediatric Primitive ReflexesDocument2 pagesPediatric Primitive ReflexesJonathanNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-385828319No ratings yet
- Child-Pugh Score & MELDDocument3 pagesChild-Pugh Score & MELDChaterine GraceNo ratings yet
- NCP EmphysemaDocument9 pagesNCP Emphysemahermesdave188% (8)
- Child Development and Milestones - Knowledge at AMBOSSDocument22 pagesChild Development and Milestones - Knowledge at AMBOSSJoseNo ratings yet
- Primitive Reflexes Cheat Sheet FinalDocument3 pagesPrimitive Reflexes Cheat Sheet FinalAlano S. LimgasNo ratings yet
- Cranial Nerve V: The Trigeminal Nerve: SensoryDocument4 pagesCranial Nerve V: The Trigeminal Nerve: SensoryJhon LeeNo ratings yet
- MCN L ReviewerDocument8 pagesMCN L ReviewerkimaytacordaNo ratings yet
- MovSciLec MSC 2101 Week13Document14 pagesMovSciLec MSC 2101 Week13Mary SotoNo ratings yet
- S3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFDocument13 pagesS3-06 Ophthalmology Eyelid, Lacrimal - Orbital Disorders (v2) PDFAl SyNo ratings yet
- Assessing The Reflexes Bell-Magendie LawDocument9 pagesAssessing The Reflexes Bell-Magendie LawRoger ViloNo ratings yet
- Cephalocaudal KemerutDocument10 pagesCephalocaudal KemerutKIANA LOUISE ROMANONo ratings yet
- Logo) : Cross Section of The Lower TrunkDocument4 pagesLogo) : Cross Section of The Lower TrunkJohn DoeNo ratings yet
- Central Nervous System Examination: Overview & PurposeDocument5 pagesCentral Nervous System Examination: Overview & PurposebismahNo ratings yet
- 15 Neonatal Reflexes, Stimulus, Response and ImplicationsDocument6 pages15 Neonatal Reflexes, Stimulus, Response and Implicationsfaith eliotNo ratings yet
- Large Pupil Small Pupil Cranial Nerve V - Trigeminal Nerve MotorDocument3 pagesLarge Pupil Small Pupil Cranial Nerve V - Trigeminal Nerve MotorKhristine Andrea RabagoNo ratings yet
- Strabismus IntroDocument28 pagesStrabismus Introxakos16766No ratings yet
- Pedia 44 59Document3 pagesPedia 44 59Colleena CortesNo ratings yet
- Cranial Nerve Assessment SheetDocument1 pageCranial Nerve Assessment SheetirmakrsekNo ratings yet
- Week 8 - Assessment of The EarsDocument3 pagesWeek 8 - Assessment of The EarsJuan Miguel TevesNo ratings yet
- 14.understanding Primitive Reflexes and Their Role in Growth and DevelopmentDocument6 pages14.understanding Primitive Reflexes and Their Role in Growth and Developmenthadiatullah alifNo ratings yet
- NER4 and 5 NotesDocument11 pagesNER4 and 5 NotesjasminNo ratings yet
- Cranial NerveDocument1 pageCranial NerveramNo ratings yet
- LAB Reflex PhysiologyDocument4 pagesLAB Reflex PhysiologyCarl Cedrick FlojoNo ratings yet
- Unconsciousness - DR Astra Dea SPS: General ExaminationDocument3 pagesUnconsciousness - DR Astra Dea SPS: General ExaminationGabriella TjondroNo ratings yet
- HA RLE MidtermsDocument7 pagesHA RLE MidtermsKaela ChoiNo ratings yet
- Assessing Newborn Re Exes: Tonic Neck Re Ex (Fencing Re Ex)Document4 pagesAssessing Newborn Re Exes: Tonic Neck Re Ex (Fencing Re Ex)Mariah Blez BognotNo ratings yet
- (ANA) 1.04 The Forearm and The HandDocument7 pages(ANA) 1.04 The Forearm and The Handmonsa medNo ratings yet
- Superficialreflexes 150609023712 Lva1 App6891Document1 pageSuperficialreflexes 150609023712 Lva1 App6891Karthik TNo ratings yet
- 06 Bone and Soft TissueDocument22 pages06 Bone and Soft TissuecarlgangcaNo ratings yet
- 133 - Neurology Pathology - Midbrain Lesions Benedikt, Weber, Claude, Parinaud SyndromeDocument5 pages133 - Neurology Pathology - Midbrain Lesions Benedikt, Weber, Claude, Parinaud Syndromeice.bear.wolfoNo ratings yet
- General Assessment: Additional Notes: BlueDocument4 pagesGeneral Assessment: Additional Notes: BlueKaiken DukeNo ratings yet
- (ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Document11 pages(ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Noreen Hannah GabrielNo ratings yet
- ReflexesDocument37 pagesReflexesmishky19No ratings yet
- H.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceDocument4 pagesH.A. Lec (L7 B) - Assessing Head and Neck, Eyes and Visual Acuity, Ears and BalanceCastallia LascuñaNo ratings yet
- ANA.S4.CA22.Lower Extremity IDocument13 pagesANA.S4.CA22.Lower Extremity ICazz HeyNo ratings yet
- Deformities OF The Lower Limb: DR - Tehreem NasirDocument57 pagesDeformities OF The Lower Limb: DR - Tehreem NasirAhmed SaeedNo ratings yet
- 14.understanding Primitive Reflexes and Their Role in Growth and DevelopmentDocument6 pages14.understanding Primitive Reflexes and Their Role in Growth and DevelopmentGeotamNo ratings yet
- Newborn's ReflexesDocument3 pagesNewborn's ReflexesGeguirra, Michiko SarahNo ratings yet
- 2021 Neuropsychological DevelopmentDocument90 pages2021 Neuropsychological DevelopmentMahmoud SuleimanNo ratings yet
- All Clinical Examinations GuideDocument29 pagesAll Clinical Examinations Guideasalizwa ludlalaNo ratings yet
- Ana.1.ca1.scalp and SkullDocument3 pagesAna.1.ca1.scalp and SkullJohn DoeNo ratings yet
- Cranial NerveDocument3 pagesCranial NerveMatty JolbitadoNo ratings yet
- NCM107 Leopolds ManeuverDocument4 pagesNCM107 Leopolds Maneuverchloepaxton030No ratings yet
- Primitive-Reflexes, Neonatal Reflexes - Pediatric Physical TherapyDocument17 pagesPrimitive-Reflexes, Neonatal Reflexes - Pediatric Physical TherapyBisma MalikNo ratings yet
- 2021 Neuropsychological DevelopmentDocument90 pages2021 Neuropsychological DevelopmentMahmoud SuleimanNo ratings yet
- 2 THERA EX WK 2 Craniomandibular Joint and The SpineDocument5 pages2 THERA EX WK 2 Craniomandibular Joint and The SpinerkNo ratings yet
- Adult Reflexes Bicep ReflexDocument4 pagesAdult Reflexes Bicep ReflexChris Deinielle Marcoleta SumaoangNo ratings yet
- Physio Lec LT 2Document66 pagesPhysio Lec LT 2Macy MarianNo ratings yet
- 1.03 General Survey, Skin and Anthropometric AssessmentDocument14 pages1.03 General Survey, Skin and Anthropometric AssessmentKim DeeNo ratings yet
- ReflexesDocument1 pageReflexesBinal Joshi100% (1)
- Emailing SUPERFICIAL REFLEXES DR JAVERIA PDFDocument28 pagesEmailing SUPERFICIAL REFLEXES DR JAVERIA PDFNoor ZehraNo ratings yet
- Anatomy: Flexor Digitorum Profundus (FDP) : MusclesDocument8 pagesAnatomy: Flexor Digitorum Profundus (FDP) : MusclesmilananandNo ratings yet
- Understanding Primitive Reflexes and Their Role in Growth and Development: A ReviewDocument5 pagesUnderstanding Primitive Reflexes and Their Role in Growth and Development: A ReviewZuveria LatifNo ratings yet
- Cranial NervesDocument4 pagesCranial NervesDenis QosjaNo ratings yet
- ReflexesDocument22 pagesReflexesgmpcbpzdysNo ratings yet
- Temporomandibular JointDocument3 pagesTemporomandibular JointFatima JamalNo ratings yet
- Muscles EscanillaDocument9 pagesMuscles EscanillaESCANILLA CRISTINENo ratings yet
- Mdentom NotesDocument30 pagesMdentom NotesMacy MarianNo ratings yet
- Posture: Sign Neuro-Muscular Maturity Score Sign ScoreDocument14 pagesPosture: Sign Neuro-Muscular Maturity Score Sign ScoreerylekateNo ratings yet
- Beans and Other Legumes - Types and Cooking TipsDocument6 pagesBeans and Other Legumes - Types and Cooking TipsDisha TNo ratings yet
- Maternal and Child ReviewerDocument19 pagesMaternal and Child ReviewerMYKA ESPERILANo ratings yet
- Tickler PDFDocument177 pagesTickler PDFQueenie FarrahNo ratings yet
- Medical Case 3: Vincent Brody: Guided Reflection QuestionsDocument3 pagesMedical Case 3: Vincent Brody: Guided Reflection Questionsapi-546220765No ratings yet
- Visa Appointment of LetterDocument3 pagesVisa Appointment of LetterRaaz SharmaNo ratings yet
- Tankersley Memo Pretrial Rel Bail ReformDocument37 pagesTankersley Memo Pretrial Rel Bail ReformCLDC_GSNo ratings yet
- Hyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMODocument63 pagesHyperbaric Oxygen Therapy, HBOT: Mohammad Guritno SURYOKUSUMOAkbar AmirullahNo ratings yet
- Scale For Ranking Family Health Problems Accdg To PrioritiesDocument3 pagesScale For Ranking Family Health Problems Accdg To PrioritiesArthur Brian Panit100% (1)
- Normal Laboratory Values With Nursing Consideration - UsnganDocument8 pagesNormal Laboratory Values With Nursing Consideration - UsnganPrincess Nasima M. UsnganNo ratings yet
- Lesson 8&9 Eating Disorders G7Document19 pagesLesson 8&9 Eating Disorders G7ANACORITA O. SILAGANNo ratings yet
- Defining A High-Performance lCU System For The - , 21st Century: A Position PaperDocument11 pagesDefining A High-Performance lCU System For The - , 21st Century: A Position PaperRodrigoSachiFreitasNo ratings yet
- Ug Epidemiological Bulletin 2023Wk19Document8 pagesUg Epidemiological Bulletin 2023Wk19JACKLINE ONZIANo ratings yet
- Rationale and Evidence ICDAS II September 11-1 PDFDocument43 pagesRationale and Evidence ICDAS II September 11-1 PDFmahmoudNo ratings yet
- Realti Trapi IJCTRT XXXI No1Document187 pagesRealti Trapi IJCTRT XXXI No1Denny SyafixNo ratings yet
- Essentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankDocument25 pagesEssentials of Pharmacology For Health Professions 7th Edition Woodrow Test BankNormanDanielsyftz100% (54)
- Communicable Diseases Control: November 2019Document128 pagesCommunicable Diseases Control: November 2019Henok TamiruNo ratings yet
- Dr. Vivek Bindra Bada Business Pvt. LTD: Content Contained Within Is The Sole Proprietary ofDocument6 pagesDr. Vivek Bindra Bada Business Pvt. LTD: Content Contained Within Is The Sole Proprietary ofNISHANT395100% (1)
- Composite Vs Amalgam PowerpointDocument17 pagesComposite Vs Amalgam Powerpointapi-322463366100% (1)
- PURBANCHAL UNIVERSITY - ReportDocument29 pagesPURBANCHAL UNIVERSITY - ReportAsh-i ShNo ratings yet
- ActinomycetesDocument15 pagesActinomycetesBenson100% (3)
- Human Anatomy KROKDocument60 pagesHuman Anatomy KROKsushmitaNo ratings yet
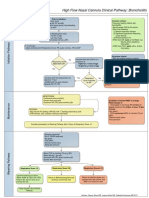
- High Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion CriteriaDocument1 pageHigh Flow Nasal Cannula Clinical Pathway: Bronchiolitis: Prior To Initiation: Inclusion Criteriad'Agung NugrohoNo ratings yet
- Southwestern University PHINMA School of Medicine Department of Medical Jurisprudence & Medical Ethics Medical Ethics and ProfessionalismDocument8 pagesSouthwestern University PHINMA School of Medicine Department of Medical Jurisprudence & Medical Ethics Medical Ethics and Professionalismthe urvashiNo ratings yet
- Acspc 046381Document44 pagesAcspc 046381Maria YounusNo ratings yet
- Case Presentation On Ischemic Cardiomyopathy & Ccf-1-1Document18 pagesCase Presentation On Ischemic Cardiomyopathy & Ccf-1-1Maliha aliNo ratings yet
- The Most Dangerous Places and Travel Destinations in The WorldDocument5 pagesThe Most Dangerous Places and Travel Destinations in The WorldAhmedNo ratings yet