You might also like
- Adult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsFrom EverandAdult Infectious Diseases Over 200 Case Studies: Intended For: Medical Students, Ambulists, Hospitalists, Nurse Practitioners, Physician AssistantsRating: 4.5 out of 5 stars4.5/5 (7)
- MBL 1 Bacterial PneumoniaDocument5 pagesMBL 1 Bacterial PneumoniaFadhlina OmarNo ratings yet
- Microbiology - 16Document5 pagesMicrobiology - 16karmylle andradeNo ratings yet
- X0xheather - Pathophysiology of Bacterial Infections PDFDocument5 pagesX0xheather - Pathophysiology of Bacterial Infections PDFAbdul RaufNo ratings yet
- Pathophysiology of Bacterial Infections Cheat Sheet: by ViaDocument5 pagesPathophysiology of Bacterial Infections Cheat Sheet: by ViaJohann Sebastian CruzNo ratings yet
- General Pathology of Infectious DiseasesDocument42 pagesGeneral Pathology of Infectious Diseasesapi-19916399No ratings yet
- Enterococci: S. AureusDocument2 pagesEnterococci: S. AureusShift UallNo ratings yet
- Gram Positive and Negative BacteriaDocument2 pagesGram Positive and Negative BacteriaHashim Mushtasin RezaNo ratings yet
- Lec8 Infectious DiseasesDocument32 pagesLec8 Infectious DiseasesmanuelNo ratings yet
- Bacterial Classification and Disease: An Organ System ApproachDocument33 pagesBacterial Classification and Disease: An Organ System ApproachSyed ShahNo ratings yet
- The Lower Respiratory Tract InfectionsDocument19 pagesThe Lower Respiratory Tract Infectionshibasirag22No ratings yet
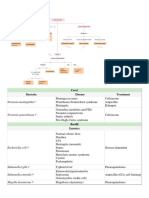
- Gram-Negative Bacteria Diseases and TreatmentsDocument4 pagesGram-Negative Bacteria Diseases and TreatmentswingNo ratings yet
- Causes and Classification of PneumoniaDocument1 pageCauses and Classification of PneumoniaAzirayah WoshiNo ratings yet
- Bacteria and Associated DiseasesDocument7 pagesBacteria and Associated DiseasesAhmed ALiNo ratings yet
- Chapter 8 - Infectious DiseasesDocument17 pagesChapter 8 - Infectious DiseasesAgnieszka WisniewskaNo ratings yet
- Gram Stain BacteriaDocument5 pagesGram Stain BacteriaMaya LaPradeNo ratings yet
- Microbiology PinkDocument3 pagesMicrobiology PinkBenjamin GaliaNo ratings yet
- Bergey'S Manual Classification of BacteriologyDocument7 pagesBergey'S Manual Classification of BacteriologyItsMeAffaNo ratings yet
- Bugs & Drugs!Document43 pagesBugs & Drugs!Safiyah Aliah Nor RosliNo ratings yet
- Tugas Mikrobiologiku Mendekati SeleseDocument5 pagesTugas Mikrobiologiku Mendekati SelesealdaNo ratings yet
- Pathology Week7 InfectionDocument18 pagesPathology Week7 InfectionSalifyanji SimpambaNo ratings yet
- 9.pneumonia 1 Nov '19Document62 pages9.pneumonia 1 Nov '19Arleen MatincaNo ratings yet
- Microbiology - 18Document7 pagesMicrobiology - 18karmylle andradeNo ratings yet
- Opportunistic Fungal Infection PDFDocument48 pagesOpportunistic Fungal Infection PDFMalvika BabuNo ratings yet
- General Pathology of Infectious DiseasesDocument47 pagesGeneral Pathology of Infectious DiseasesAbdullah EmadNo ratings yet
- Micorbiology Overview (Bacteria, Viruses, Laboratory Diagnosis)Document88 pagesMicorbiology Overview (Bacteria, Viruses, Laboratory Diagnosis)nikoleta.2604.zhekovaNo ratings yet
- 1 Urtd+eviDocument76 pages1 Urtd+eviIfabiyi OlaniyiNo ratings yet
- Pneumonia Microbiology GuideDocument15 pagesPneumonia Microbiology GuidepuniariNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument9 pagesMicrobial Diseases of The Respiratory SystemAnaNo ratings yet
- S. Aureus Pneumonia Often Complicates Illness Caused by Influenza VirusesDocument14 pagesS. Aureus Pneumonia Often Complicates Illness Caused by Influenza VirusesRia Dela CruzNo ratings yet
- List of BacteriaDocument2 pagesList of BacteriaImtiaz AhmedNo ratings yet
- M6 Bacteriology Pre Task - CaparasDocument1 pageM6 Bacteriology Pre Task - CaparasGretta CaparasNo ratings yet
- ncm112 FinalsDocument18 pagesncm112 FinalsAbegail MierNo ratings yet
- Summary of Infectious DiseasesDocument407 pagesSummary of Infectious DiseasesMh HmNo ratings yet
- Gram Staining:: Gram-Positive Bacteria Gram-Negative BacteriaDocument22 pagesGram Staining:: Gram-Positive Bacteria Gram-Negative BacteriaAziil LiizaNo ratings yet
- Major Viral, Bacterial, and Fungal DiseasesDocument75 pagesMajor Viral, Bacterial, and Fungal DiseasesMary LyonNo ratings yet
- 4e8ae48410.TERAPI ISPA DAN ISPBDocument56 pages4e8ae48410.TERAPI ISPA DAN ISPBAbd HarisNo ratings yet
- Nursing CS Common Bacteria by Body SystemDocument1 pageNursing CS Common Bacteria by Body SystemBai Jannah Sahida SilonganNo ratings yet
- Bacterial and Viral Infection MechanismsDocument24 pagesBacterial and Viral Infection MechanismsLinda NguyenNo ratings yet
- Tabel 1. Etiologi Infeksi Pada Faringitis Bakteri Virus Jamur Bakteri AtipikalDocument2 pagesTabel 1. Etiologi Infeksi Pada Faringitis Bakteri Virus Jamur Bakteri AtipikalMuhammad Harry Badrus SNo ratings yet
- Pertussis, Meningococcal meningitis, Strept pharyngitis, Diphtheria, Pulmonary TBDocument14 pagesPertussis, Meningococcal meningitis, Strept pharyngitis, Diphtheria, Pulmonary TBAhmed MansourNo ratings yet
- Infectious Diseases: Bacteria, Viruses, Mycetes & ParasitesDocument137 pagesInfectious Diseases: Bacteria, Viruses, Mycetes & ParasitesWendielynne MillomedaNo ratings yet
- Common Viral Infections CC Sarmiento DIdacticsDocument87 pagesCommon Viral Infections CC Sarmiento DIdacticsUthuriel27No ratings yet
- Bacteriology - Semifinals - Neisseria and MoraxellaDocument10 pagesBacteriology - Semifinals - Neisseria and MoraxellaUshuaia Ira Marie L. GallaronNo ratings yet
- 10.bakteri Penyebab IMSDocument68 pages10.bakteri Penyebab IMSnurrahayuningratNo ratings yet
- Infectious Diseases of the Nervous System and Respiratory TractDocument7 pagesInfectious Diseases of the Nervous System and Respiratory TractEdna ChanNo ratings yet
- MED-ORG-TOPIC-234Document9 pagesMED-ORG-TOPIC-234barbadillojames419No ratings yet
- Enterobacteriaceae Opportunistic PathogensDocument1 pageEnterobacteriaceae Opportunistic PathogensMiaoNo ratings yet
- Sexually Transmitted InfectionsDocument25 pagesSexually Transmitted InfectionsQasim HaleimiNo ratings yet
- Microbiology Assignment. ADocument26 pagesMicrobiology Assignment. ACynthia AbbangNo ratings yet
- All Details About Pneumocystis Carinii Pneumonia (PCP)Document7 pagesAll Details About Pneumocystis Carinii Pneumonia (PCP)NHZANo ratings yet
- Fungal Pneumonia Causes and Risk FactorsDocument3 pagesFungal Pneumonia Causes and Risk FactorsskNo ratings yet
- Objectives: Table 1. Selected Etiologies of Sore ThroatDocument12 pagesObjectives: Table 1. Selected Etiologies of Sore ThroatRANINo ratings yet
- Anaerobic CultureDocument34 pagesAnaerobic CultureHema DaheriyaNo ratings yet
- PyodermaDocument58 pagesPyodermaRizky Takdir RamadhanNo ratings yet
- (Important!) Microbiology Vocabulary ListDocument6 pages(Important!) Microbiology Vocabulary ListKelly LeeNo ratings yet
- Bacteriology Edited 1Document65 pagesBacteriology Edited 1Ali AhmedNo ratings yet
- Microbial Diseases of The Nervous SystemDocument7 pagesMicrobial Diseases of The Nervous SystemAnaNo ratings yet
- Summary of Infectious DiseasesDocument415 pagesSummary of Infectious DiseasesAlston Foods BVNo ratings yet
- English Task "Analytical Exposition": Smoking BansDocument7 pagesEnglish Task "Analytical Exposition": Smoking BansFirda RazaqNo ratings yet
- Jesus Uplifts The PoorDocument10 pagesJesus Uplifts The Poor명연우No ratings yet
- 2000-03 Taconic Running Life March 2000Document24 pages2000-03 Taconic Running Life March 2000TaconicArchiveNo ratings yet
- Sixth CommandmentDocument26 pagesSixth CommandmentJewel Anne RentumaNo ratings yet
- Clearing Clutter With Eft PDFDocument23 pagesClearing Clutter With Eft PDFIftikhar Hassun100% (2)
- DAVAO DOCTORS COLLEGE NURSING DRUG STUDYDocument3 pagesDAVAO DOCTORS COLLEGE NURSING DRUG STUDYJerremy LuqueNo ratings yet
- B2 LVDOCTOBER2007 SMDocument148 pagesB2 LVDOCTOBER2007 SMjason640100% (2)
- ReportDocument1 pageReportRanjan Mano100% (1)
- Xii Physical Education PracticalDocument3 pagesXii Physical Education PracticalAayush AdlakNo ratings yet
- 13th Month Pay Law and JurisprudenceDocument2 pages13th Month Pay Law and JurisprudenceJennylyn Biltz AlbanoNo ratings yet
- GatesDocument188 pagesGatesMilos LIcko Bash RandjelovicNo ratings yet
- Spain-Final ProjectDocument29 pagesSpain-Final Projectapi-264431075No ratings yet
- Oil Keeper Job at PacrimDocument2 pagesOil Keeper Job at Pacrimwinda chairunissaNo ratings yet
- Observation of Unknown SpectrumDocument3 pagesObservation of Unknown SpectrumOmar HusseinNo ratings yet
- Practice questions on oxidation and reduction reactionsDocument7 pagesPractice questions on oxidation and reduction reactionsLeAqwaNo ratings yet
- Water Hardness Case StudyDocument15 pagesWater Hardness Case StudyTaima GhNo ratings yet
- Comparative Study of Soaps of Hul P Amp G Godrej Nirma and Johnson Amp Johnson 130410234307 Phpapp01 PDFDocument71 pagesComparative Study of Soaps of Hul P Amp G Godrej Nirma and Johnson Amp Johnson 130410234307 Phpapp01 PDFdheeraj agarwalNo ratings yet
- Market Sorvey On PlywoodDocument19 pagesMarket Sorvey On PlywoodEduardo MafraNo ratings yet
- Año del Fortalecimiento de la Soberanía NacionalDocument4 pagesAño del Fortalecimiento de la Soberanía NacionalRYAN 28SKNo ratings yet
- BASF Puristar R3-12 - BF-9220 - PuriStar - R3-12 - PDS - Rev.2020-12 Spec SheetDocument2 pagesBASF Puristar R3-12 - BF-9220 - PuriStar - R3-12 - PDS - Rev.2020-12 Spec SheetAlNo ratings yet
- Klee N Rite 50100Document24 pagesKlee N Rite 50100Nestor Marquez-DiazNo ratings yet
- Presentation 1Document20 pagesPresentation 1anon_658550121No ratings yet
- A Study On Employee Absenteeism at TVS Sundaram Fasteners Limited, Chennai, TamilnaduDocument7 pagesA Study On Employee Absenteeism at TVS Sundaram Fasteners Limited, Chennai, TamilnaduIJRASETPublicationsNo ratings yet
- Moderate and Extreme HypofractionationDocument32 pagesModerate and Extreme HypofractionationsamuelfsjNo ratings yet
- 1st SemesterDocument28 pages1st SemesterSathiya SarangapaniNo ratings yet
- Standard Operating Procedure: Validation of Heating Ventilation and Air Conditioning (Hvac) SystemDocument20 pagesStandard Operating Procedure: Validation of Heating Ventilation and Air Conditioning (Hvac) SystemMaryanthony Namyalo100% (3)
- General Catalogue 2019: UNIOR D.DDocument401 pagesGeneral Catalogue 2019: UNIOR D.DjinpoeNo ratings yet
- Calcium chloride MSDSDocument5 pagesCalcium chloride MSDSDarshilNo ratings yet
- CIE IGCSE BiologyDocument25 pagesCIE IGCSE Biologytgdzbspikio.comNo ratings yet
- Surgery Hazel Final1Document21 pagesSurgery Hazel Final1Sittie RamosNo ratings yet