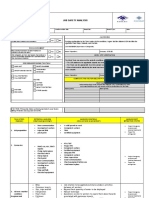
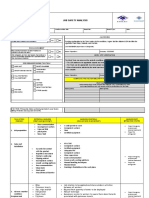
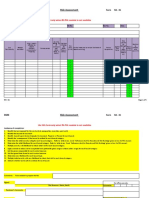
POINT OF WORK
RISK ASSESSMENT
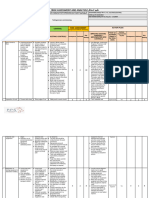
Job Task / Activity Location Date:
Additional Safety Assessment
.............................................. ....................................... .........................
Remaining risk (High,
BEFORE YOU START (tick appropriate box) Yes No N/A
HAZARD Control Measures / Precautions Medium, Low)
Part 1 - Stop
Do you have the right documentation for the job?
Part 3 - Assessment
Do you have the right PPE for the job?
Are power tools and leads PAT tested?
Visual inspection of slings carried out?
Slings suitable for task (safe working load?)
If you have answered ' No' to any of the above, take the required action or report to the
nominated person.
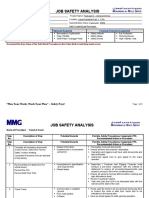
Safety Assessment -
If the HAZARD is present, tick the box
Slips Thermal Comfort
Trips Energy Release
Falls Electrical DECLARATION: Signature - all Team
Heights Chemical Print Name - all Team Members Members
I am satisfied that the level
Part 4 - Declaration
Falling Objects Fire of risk to the working party,
Entanglement Confined Spaces to others & to the
Drawing-in Glass environment, is as low as is
Part 2 - Think
Trapping (crush, shear) Unauthorised Access reasonably practicable &
that adequate controls are
Impact (moving object) Access / Egress
in place.
Impact (stationary object) Water Ingress
Contact (Cut/friction/abrasion) LPG
Contact (Stabbing/Puncture) Noise
Ejection Vibration End of Job Review
Equipment Stability Manual Handling Are there any lessons for next time? YES NO
Part 5 - Review
Burns (Hot, Cold) Upper Limb Disorder Has the work created any new Hazards? YES NO
Burns (Chemical) Vehicle / Pedestrian segregation If you have answered YES to either of these questions, tell your Line Manager
If other, (specify)
Circle any ticks for hazards that are significant and for which there are no (or inadequate) controls. If you Signature: ...............................................................
have circled any hazards, Part 3 needs to be completed and additional control measures put in place before
work commences.
You might also like
- Air Conditioner InstallationDocument3 pagesAir Conditioner InstallationWalid KhelfaNo ratings yet
- Electrical InstallationDocument3 pagesElectrical InstallationWalid KhelfaNo ratings yet
- P111-Rsme-Tra-007 - Tra For Cold Tie inDocument5 pagesP111-Rsme-Tra-007 - Tra For Cold Tie inDarius DsouzaNo ratings yet
- JRA 10-005 Insttalation of New Dodo GateDocument9 pagesJRA 10-005 Insttalation of New Dodo GateAijaz AhmedNo ratings yet
- Backfilling, Leveling RISK ASSESSMENTDocument6 pagesBackfilling, Leveling RISK ASSESSMENTVimal ViswanathNo ratings yet
- Tra 002Document6 pagesTra 002Bilal0% (1)
- Biopolis TBM 17 Feb 2024Document3 pagesBiopolis TBM 17 Feb 2024SelvamNo ratings yet
- Connexion de Cable MT Avec Boite JonctionDocument3 pagesConnexion de Cable MT Avec Boite JonctionWalid KhelfaNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- Daily plant inspectionDocument5 pagesDaily plant inspectionSteve O'DonoghueNo ratings yet
- TRA SS ChannelDocument5 pagesTRA SS ChannelBilalNo ratings yet
- STARRT CardDocument2 pagesSTARRT Cardsanny100% (1)
- Topography SurveyDocument2 pagesTopography SurveyAMIN100% (2)
- JSA G20 Scaffolding Erection DismantlingDocument4 pagesJSA G20 Scaffolding Erection DismantlingemmyNo ratings yet
- Pyramid Drilling S.A.E: Manual Title: Form Name: Issue Date Revision No. Revision Date Prepared by Approved by Level NoDocument2 pagesPyramid Drilling S.A.E: Manual Title: Form Name: Issue Date Revision No. Revision Date Prepared by Approved by Level NoLenaj EbronNo ratings yet
- Task Risk Assessment for Excavation, Backfilling, Leveling and CompactionDocument7 pagesTask Risk Assessment for Excavation, Backfilling, Leveling and CompactionBilal50% (2)
- JSA ELETRICAL MaintenanceDocument17 pagesJSA ELETRICAL MaintenanceWeru MorrisNo ratings yet
- Packing Pumps New - FO-GL-HAL-HSE-0103FDocument4 pagesPacking Pumps New - FO-GL-HAL-HSE-0103FMohamed El-SawahNo ratings yet
- JSA G17 Lift Container With CraneDocument4 pagesJSA G17 Lift Container With Cranesetiawanaji407No ratings yet
- Crane Safety TipsDocument4 pagesCrane Safety Tipssetiawanaji407100% (1)
- Gangway Installation JHADocument3 pagesGangway Installation JHAazrul100% (1)
- JSA (Rev1 6.4.13) Set-Up Safe House Habitat.Document4 pagesJSA (Rev1 6.4.13) Set-Up Safe House Habitat.Danial AfandiNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewWalid KhelfaNo ratings yet
- FACADE Maintenance Risk AssessmentDocument2 pagesFACADE Maintenance Risk Assessmentطارق رضوانNo ratings yet
- Construction Risk AssessmentDocument19 pagesConstruction Risk AssessmentMuhammad Shahid Iqbal100% (3)
- JRA 10-009 Concrete of Foundation FEC Switch RoomDocument5 pagesJRA 10-009 Concrete of Foundation FEC Switch RoomAijaz AhmedNo ratings yet
- JSA Template for FRP Piping InstallationDocument6 pagesJSA Template for FRP Piping InstallationDanial AfandiNo ratings yet
- JRA No 11-195 Field Calibration For Valves & Transmitters at FEC AreaDocument5 pagesJRA No 11-195 Field Calibration For Valves & Transmitters at FEC AreaAijaz AhmedNo ratings yet
- Risk Assessment Carpentry Works For Dismantling Wooden BoxesDocument10 pagesRisk Assessment Carpentry Works For Dismantling Wooden BoxesSinaNo ratings yet
- JRA No 11-192 Manual Excavation For Construction of New FoundationsDocument4 pagesJRA No 11-192 Manual Excavation For Construction of New FoundationsAijaz AhmedNo ratings yet
- Pps - Risk AssessmentDocument18 pagesPps - Risk AssessmentIsmail KamelNo ratings yet
- PCSB JHA Troubleshooting SMRGDocument4 pagesPCSB JHA Troubleshooting SMRGMohamad JazlanNo ratings yet
- Jsa Breaking Down Bop Into Handling SkidDocument4 pagesJsa Breaking Down Bop Into Handling SkidPaulNo ratings yet
- RA Jetty 2 ExpansionDocument4 pagesRA Jetty 2 ExpansionpsarewoloNo ratings yet
- JSA PANEL SULLAYILDocument6 pagesJSA PANEL SULLAYILthennarasuNo ratings yet
- W Nit-466 4 2Document3 pagesW Nit-466 4 2A ReddyNo ratings yet
- JRA No 11-194 Repairing of Water Spouts With The Help of Cherry Picker & Scaffolding Platform at FEC Switch RoomDocument5 pagesJRA No 11-194 Repairing of Water Spouts With The Help of Cherry Picker & Scaffolding Platform at FEC Switch RoomAijaz AhmedNo ratings yet
- Risk Assessment Construction of Lighting Pole at Site OfficeDocument9 pagesRisk Assessment Construction of Lighting Pole at Site OfficeSinaNo ratings yet
- Hazard Identification, Risk Assessment & Risk Control (Hirarc)Document6 pagesHazard Identification, Risk Assessment & Risk Control (Hirarc)sopiNo ratings yet
- CSCEC HSE-F-01 Risk Assessment Form - Excavation& Backfilling - RA-02Document12 pagesCSCEC HSE-F-01 Risk Assessment Form - Excavation& Backfilling - RA-02Dan SarmientoNo ratings yet
- Risk Assessment For Dismantling of Temporary ServicesDocument17 pagesRisk Assessment For Dismantling of Temporary ServicesAnandu AshokanNo ratings yet
- STA ElectricalDocument3 pagesSTA ElectricalimranNo ratings yet
- Construction Risk AssessmentDocument21 pagesConstruction Risk AssessmentMuhammad Shahid Iqbal0% (1)
- PEDSB JHA - Take PictureDocument1 pagePEDSB JHA - Take PictureChe Wan ErliyasNo ratings yet
- Job Safety Analysis: Required References Jsa ReviewDocument3 pagesJob Safety Analysis: Required References Jsa ReviewMoaatazz Nouisri100% (1)
- 2.5 Hot WorkDocument5 pages2.5 Hot Workamdarrif3723No ratings yet
- Lifting and Removing Using The Forklift or Telescopic Loader in SiteDocument3 pagesLifting and Removing Using The Forklift or Telescopic Loader in SiteAMINNo ratings yet
- JRA No 11-194 Repairing of Water Spouts With The Help of Cherry Picker & Scaffolding Platform at FEC Switch RoomDocument5 pagesJRA No 11-194 Repairing of Water Spouts With The Help of Cherry Picker & Scaffolding Platform at FEC Switch RoomAijaz AhmedNo ratings yet
- Battery Room HVAC Safety AnalysisDocument3 pagesBattery Room HVAC Safety AnalysisMajdiSahnounNo ratings yet
- Chop Saw PDFDocument3 pagesChop Saw PDFAnonymous YrCsoYgNo ratings yet
- Block Work (Unit Masonary) RISK ASSESSMENTDocument8 pagesBlock Work (Unit Masonary) RISK ASSESSMENTVimal ViswanathNo ratings yet
- Jha New Format-Painting Revision)Document8 pagesJha New Format-Painting Revision)Kenny Hassan100% (1)
- JRA 10-001 Devlopment of Barrow AreaDocument5 pagesJRA 10-001 Devlopment of Barrow AreaAijaz AhmedNo ratings yet
- JSA - Scissor - Lift 2023Document4 pagesJSA - Scissor - Lift 2023syed khaja misbhuddinNo ratings yet
- Risk Assessment RevisionDocument6 pagesRisk Assessment RevisionAneesh100% (1)
- Water Testin TRADocument4 pagesWater Testin TRAabdulhanansamo65No ratings yet
- Pre-Job Hazard AnalysisDocument5 pagesPre-Job Hazard AnalysisFiras HamanNo ratings yet
- Grenfell Tower Rydon Construction Phase Plan (2016)Document31 pagesGrenfell Tower Rydon Construction Phase Plan (2016)BryanNo ratings yet
- RQL Head Office Safety Statement Sept 2017 Rev 16 RQL SS 01Document89 pagesRQL Head Office Safety Statement Sept 2017 Rev 16 RQL SS 01BryanNo ratings yet
- CIF Safety Health Wellbeing Calendar 2022 - V4Document1 pageCIF Safety Health Wellbeing Calendar 2022 - V4BryanNo ratings yet
- Road Haulage of Round Timber Code of PracticeDocument13 pagesRoad Haulage of Round Timber Code of PracticeBryanNo ratings yet
- Event Management PlanDocument61 pagesEvent Management PlanBryanNo ratings yet
- Eliminating Silica Dust RisksDocument3 pagesEliminating Silica Dust RisksBryanNo ratings yet
- NDADocument3 pagesNDABryanNo ratings yet
- Alcumus Isoqar Iso 45001 Gap Analysis PDFDocument15 pagesAlcumus Isoqar Iso 45001 Gap Analysis PDFBryanNo ratings yet
- 2021 Candidates Assessment Sheets EMTDocument27 pages2021 Candidates Assessment Sheets EMTBryanNo ratings yet
- BusinessContinuityPlan PDFDocument4 pagesBusinessContinuityPlan PDFBryanNo ratings yet
- IFI Safety Statement August 2017Document527 pagesIFI Safety Statement August 2017BryanNo ratings yet
- GuidanceDocument64 pagesGuidanceПавел АнгеловNo ratings yet
- 9 MICRisk AssessmentforPregnantEmployeesv1Document5 pages9 MICRisk AssessmentforPregnantEmployeesv1BryanNo ratings yet
- EFQM Excellence PDFDocument12 pagesEFQM Excellence PDFamaneuyNo ratings yet
- 20170719103700-DILLINGER Integrated Management Manual Rev4Document77 pages20170719103700-DILLINGER Integrated Management Manual Rev4BryanNo ratings yet
- QMS Audit - Checklist - IsO 9001 - 2008Document27 pagesQMS Audit - Checklist - IsO 9001 - 2008Rizaldi DjamilNo ratings yet
- Pas 99 Integrated Management System PDFDocument24 pagesPas 99 Integrated Management System PDFBryanNo ratings yet
- PIDChecklist PDFDocument2 pagesPIDChecklist PDFBryanNo ratings yet
- Registration as an ECITB Approved TrainerDocument2 pagesRegistration as an ECITB Approved TrainerBryanNo ratings yet
- Workplace Safety and Health ManagementDocument56 pagesWorkplace Safety and Health ManagementRebecca WilliamsNo ratings yet
- Water UK Classifications PDFDocument33 pagesWater UK Classifications PDFBryanNo ratings yet
- Nebosh Diploma Unit A1Document1 pageNebosh Diploma Unit A1SeleniNo ratings yet
- Rotary Equality and DiversityDocument16 pagesRotary Equality and DiversityBryanNo ratings yet
- Epa Water Treatment Manual Filtration 1Document80 pagesEpa Water Treatment Manual Filtration 1alkemeya100% (1)
- ##Not Translate.14-Msds-For Acrylic Levelling Agent (Liquid)Document9 pages##Not Translate.14-Msds-For Acrylic Levelling Agent (Liquid)saddamNo ratings yet
- Terex RT230Document18 pagesTerex RT230ebonilla880% (1)
- Work Instruction for Paint Shop ExtensionDocument15 pagesWork Instruction for Paint Shop ExtensionAli WaqasNo ratings yet
- Spare Parts List: R902451550 R902427801 Drawing: Material NumberDocument26 pagesSpare Parts List: R902451550 R902427801 Drawing: Material NumberAdrian MartinNo ratings yet
- SDS For 46SJDocument19 pagesSDS For 46SJemusimaNo ratings yet
- SOP for Cyclone blockage removalDocument3 pagesSOP for Cyclone blockage removalVisnu SankarNo ratings yet
- MSDS EonDocument5 pagesMSDS EonIndieNo ratings yet
- DRRM ReportDocument8 pagesDRRM ReportCortez del Airam0% (1)
- Information Required For Preparation of Offers For Safety Consultancy AssignmentsDocument3 pagesInformation Required For Preparation of Offers For Safety Consultancy AssignmentsAnamika TiwaryNo ratings yet
- Safe ReinstatementDocument9 pagesSafe ReinstatementAntonyFrancis AshokNo ratings yet
- Process Safety Management of Highly Hazardous Chemicals: Nancy J BetheaDocument55 pagesProcess Safety Management of Highly Hazardous Chemicals: Nancy J BetheaZeshanNo ratings yet
- PT Pertamina (Persero) : Lembar Data KeselamatanDocument11 pagesPT Pertamina (Persero) : Lembar Data KeselamatanPanjiNo ratings yet
- RA 01 Risk Assessment FormDocument5 pagesRA 01 Risk Assessment FormAlfa RidziNo ratings yet
- Testing and Commissioning Procedure For SCAR and SRCUDocument80 pagesTesting and Commissioning Procedure For SCAR and SRCUWinNo ratings yet
- FM Approval of Firestop ContractorsDocument16 pagesFM Approval of Firestop ContractorsMohamed Rafi MNo ratings yet
- Internal Audit Report Format For Health & SafetyDocument24 pagesInternal Audit Report Format For Health & SafetyansariNo ratings yet
- ISS-1001-TMP-00018 Site Mobile Tower Daily ChecklistDocument2 pagesISS-1001-TMP-00018 Site Mobile Tower Daily Checklistbubbles82No ratings yet
- TCCA TP 12295e - Flight Attendant Manual Standard PDFDocument68 pagesTCCA TP 12295e - Flight Attendant Manual Standard PDFPavithran DNo ratings yet
- Drum Explosions School Safety AlertDocument1 pageDrum Explosions School Safety AlertRinzin DorjiNo ratings yet
- DRRR - Module 11Document27 pagesDRRR - Module 11RHANDY EVANGELISTA80% (5)
- Fire Appendix2Document8 pagesFire Appendix2Hyeong-Ho KimNo ratings yet
- User Instructions: ERPN Centrifugal PumpsDocument39 pagesUser Instructions: ERPN Centrifugal PumpsYerko NavarroNo ratings yet
- DRRR M5Document22 pagesDRRR M5janlyn lumainoNo ratings yet
- Fy11 SH 22300 11 OSHAOrientationDocument31 pagesFy11 SH 22300 11 OSHAOrientationferoz khanNo ratings yet
- G2100 MSDSDocument5 pagesG2100 MSDSMohamed MahadeerNo ratings yet
- Stromatolyser-FB F-7052AS (3-2016)Document9 pagesStromatolyser-FB F-7052AS (3-2016)anggita windaNo ratings yet
- Ansi+asse+z359 15-2014Document48 pagesAnsi+asse+z359 15-2014Oscar CassoNo ratings yet
- Crane Travel Safety AnalysisDocument3 pagesCrane Travel Safety AnalysisDelta akathehuskyNo ratings yet
- Pre-Test-Questionnaire (Blended)Document2 pagesPre-Test-Questionnaire (Blended)al.gibranNo ratings yet