You might also like
- Tohatsu 2 Stroke Service Manual 1992 2000Document329 pagesTohatsu 2 Stroke Service Manual 1992 2000Adi Peterfi97% (38)
- BDS Curriculum 2016, KuDocument242 pagesBDS Curriculum 2016, Kuanakinra well0% (1)
- Kdle TextDocument8 pagesKdle Textdrrajesh27100% (2)
- Contemporary Undergraduate Implant Dentistry Education A Systematic ReviewDocument13 pagesContemporary Undergraduate Implant Dentistry Education A Systematic ReviewfloraNo ratings yet
- BDS Curriculum 2016Document302 pagesBDS Curriculum 2016FireFrostNo ratings yet
- BDS Curriculum 2016Document242 pagesBDS Curriculum 2016BishowNo ratings yet
- Endodoncia Por EstudiantesDocument6 pagesEndodoncia Por EstudiantescarlosNo ratings yet
- Yiu 2011Document10 pagesYiu 2011Chris MartinNo ratings yet
- Accreditation of Postgraduate Speciality TrainingDocument13 pagesAccreditation of Postgraduate Speciality TrainingHari PriyaNo ratings yet
- Behavioural Sciences A Review of Teaching of BehavDocument6 pagesBehavioural Sciences A Review of Teaching of BehavZain HadiNo ratings yet
- Cópia de Artigo - Curriculo Europeu de CariologiaDocument9 pagesCópia de Artigo - Curriculo Europeu de Cariologiaigor otavioNo ratings yet
- Reforming Dental Health Professions EducationDocument25 pagesReforming Dental Health Professions EducationSanaFatimaNo ratings yet
- Eur J Dental Education - 2017 - Field - The Graduating European Dentist A New Undergraduate Curriculum FrameworkDocument9 pagesEur J Dental Education - 2017 - Field - The Graduating European Dentist A New Undergraduate Curriculum FrameworkHernández Becerra Ivanna PaolaNo ratings yet
- 112 - Profile and Competences For The European Dentist - Update 2008Document23 pages112 - Profile and Competences For The European Dentist - Update 2008miauNo ratings yet
- Ortho Re SprogDocument6 pagesOrtho Re Sprogupul85No ratings yet
- Journal of Dental Education - 2020 - Garcia - The American Dental Education Association ADEA and Association for DentalDocument3 pagesJournal of Dental Education - 2020 - Garcia - The American Dental Education Association ADEA and Association for Dentalpolicarp1aaNo ratings yet
- Dentistry Study Program 2014 - 2Document153 pagesDentistry Study Program 2014 - 2Saleh AlsadiNo ratings yet
- Dental Public HealthDocument4 pagesDental Public HealthTrio HAHAHANo ratings yet
- Diploma of Oral Surgery-RWTH Aachen UniversityDocument11 pagesDiploma of Oral Surgery-RWTH Aachen UniversitySjcjdjdjxNo ratings yet
- Improving Assessment in Dental Education Through A Paradigm of Comprehensive Care: A Case ReportDocument13 pagesImproving Assessment in Dental Education Through A Paradigm of Comprehensive Care: A Case ReportfidelbustamiNo ratings yet
- Education Dental PriemereDocument20 pagesEducation Dental Priemerengurah_wardanaNo ratings yet
- Int Endodontic J - 2023 - DuncanDocument58 pagesInt Endodontic J - 2023 - DuncanAli FaridiNo ratings yet
- Oral Health PromotionDocument29 pagesOral Health PromotionRob21aNo ratings yet
- GuidlinesDocument10 pagesGuidlinesbubuvulpeaNo ratings yet
- Simple Present Tanse: Name:Rahma Fuaddiah Bp:1611411007Document7 pagesSimple Present Tanse: Name:Rahma Fuaddiah Bp:1611411007rahmaNo ratings yet
- Problem-Based Learning: An Interdisciplinary Approach in Clinical TeachingDocument6 pagesProblem-Based Learning: An Interdisciplinary Approach in Clinical TeachingArdianNo ratings yet
- Continuing Dental EducationDocument4 pagesContinuing Dental EducationDoggo OggodNo ratings yet
- Dental TherapyDocument9 pagesDental TherapyKatey DavidsonNo ratings yet
- Ipd 12715Document10 pagesIpd 12715Ayu DamayNo ratings yet
- Badovinac 2013Document8 pagesBadovinac 2013Naji Z. ArandiNo ratings yet
- Scandinavian Fellowship For Oral Pathology and Oral Medicine Guidelines For Oral Pathology and Oral Medicine in The Dental Curriculum.Document8 pagesScandinavian Fellowship For Oral Pathology and Oral Medicine Guidelines For Oral Pathology and Oral Medicine in The Dental Curriculum.desantosalbaNo ratings yet
- bds2013 14Document135 pagesbds2013 14Mohammed ArshadNo ratings yet
- The Bachelor of Dental Surgery Prepares Students For PatientDocument3 pagesThe Bachelor of Dental Surgery Prepares Students For PatientAmrutha DasariNo ratings yet
- UK Dental CurriculumDocument70 pagesUK Dental CurriculumSuhesh HydrosNo ratings yet
- A Review of Continuing Professional Development For Dentists in EuropeDocument13 pagesA Review of Continuing Professional Development For Dentists in EuropeWulan Ambar WatyNo ratings yet
- Impact of Regular Professional Toothbrushing On Oral Health, Related Quality of Life, and Nutritional and Cognitive Status in Nursing Home ResidentsDocument13 pagesImpact of Regular Professional Toothbrushing On Oral Health, Related Quality of Life, and Nutritional and Cognitive Status in Nursing Home ResidentsMarco Antonio García LunaNo ratings yet
- University of Sheffield Bachelor of Dental Surgery BrochureDocument12 pagesUniversity of Sheffield Bachelor of Dental Surgery BrochureYoussef MaharemNo ratings yet
- Promoting Oral Health in Older PeopleDocument2 pagesPromoting Oral Health in Older PeopleatikramadhaniNo ratings yet
- Oral Health in KindergardenDocument8 pagesOral Health in KindergardensightpowerNo ratings yet
- Artículo RevisiónDocument12 pagesArtículo RevisiónDr. JharNo ratings yet
- Patel 2006Document7 pagesPatel 2006Chris MartinNo ratings yet
- Curriculum Mapping of Health Promotion Competencies in Dental and OralDocument16 pagesCurriculum Mapping of Health Promotion Competencies in Dental and OralAnna IttyerahNo ratings yet
- Dental Treatment Needs in Lithuanian AdplescentsDocument5 pagesDental Treatment Needs in Lithuanian AdplescentsKhairunnisa SihotangNo ratings yet
- CurriculumDocument5 pagesCurriculumapi-287317229No ratings yet
- BMC Oral Health: Pit and Fissure Sealants in Dental Public Health - Application Criteria and General Policy in FinlandDocument10 pagesBMC Oral Health: Pit and Fissure Sealants in Dental Public Health - Application Criteria and General Policy in FinlandIrfan Cahya PermanaNo ratings yet
- School Dental Health Programme Pedo 2Document25 pagesSchool Dental Health Programme Pedo 2misdduaaNo ratings yet
- M.implant Munster & GboiDocument7 pagesM.implant Munster & GboiHarry ArdiyantoNo ratings yet
- Dental status of South African children receiving school oral health servicesDocument7 pagesDental status of South African children receiving school oral health servicesTy WrNo ratings yet
- Caries Secundarias 2019Document9 pagesCaries Secundarias 2019CristobalVeraNo ratings yet
- Attitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional StudyDocument9 pagesAttitudes and Lifestyle Factors in Relation To Oral Health and Dental Care in Sweden A Cross Sectional Studyasem sardyNo ratings yet
- Clinically Oriented Complete Denture ProgramDocument8 pagesClinically Oriented Complete Denture ProgramBrijesh MaskeyNo ratings yet
- Dr. Aditya V S Dubagunta's CVDocument6 pagesDr. Aditya V S Dubagunta's CVdrrakeshkathiriya1No ratings yet
- PCL Dental Science, 2065Document85 pagesPCL Dental Science, 2065bibekghale8588No ratings yet
- Oral Health Education Improved Oral Health KnowledgeDocument11 pagesOral Health Education Improved Oral Health KnowledgeGita PratamaNo ratings yet
- Integrating Global Health Within Dental Education: Inter-University Collaboration For Scaling Up A Pilot CurriculumDocument7 pagesIntegrating Global Health Within Dental Education: Inter-University Collaboration For Scaling Up A Pilot CurriculumGloria HuamaníNo ratings yet
- DentalDocument2 pagesDentalntambik210% (1)
- documentDocument26 pagesdocumentnadiaNo ratings yet
- Research Article: Outcome of Chair-Side Dental Fear Treatment: Long-Term Follow-Up in Public Health SettingDocument7 pagesResearch Article: Outcome of Chair-Side Dental Fear Treatment: Long-Term Follow-Up in Public Health SettingAdriani PanjaitanNo ratings yet
- Research Article: Outcome of Chair-Side Dental Fear Treatment: Long-Term Follow-Up in Public Health SettingDocument7 pagesResearch Article: Outcome of Chair-Side Dental Fear Treatment: Long-Term Follow-Up in Public Health SettingAdriani PanjaitanNo ratings yet
- Molar Incisor Hypomineralization: A Clinical Guide to Diagnosis and TreatmentFrom EverandMolar Incisor Hypomineralization: A Clinical Guide to Diagnosis and TreatmentKatrin BekesNo ratings yet
- LCD LG (M17,1917S-BNN E)Document34 pagesLCD LG (M17,1917S-BNN E)Ion IonutNo ratings yet
- Domestic Water-Supply - TheoryDocument19 pagesDomestic Water-Supply - Theoryyarzar17No ratings yet
- SPE 63041 Design and Installation of Sand Separation and Handling SystemDocument10 pagesSPE 63041 Design and Installation of Sand Separation and Handling Systemalexalek2000No ratings yet
- Solid State Physics by Kettel Chapter 4Document17 pagesSolid State Physics by Kettel Chapter 4Taseer BalochNo ratings yet
- Ambiguity in Legal Translation: Salah Bouregbi Badji Mokhtar University Annaba - Algeria - Salihbourg@Document14 pagesAmbiguity in Legal Translation: Salah Bouregbi Badji Mokhtar University Annaba - Algeria - Salihbourg@MerHamNo ratings yet
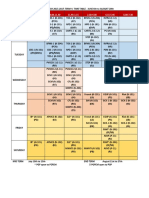
- Term 4 Time Table & Exam Schedule.Document4 pagesTerm 4 Time Table & Exam Schedule.Anonymous FD3MCd89ZNo ratings yet
- 2018 General Education Reviewer Part 10 - 50 Questions With Answers - LET EXAM - Questions & AnswersDocument10 pages2018 General Education Reviewer Part 10 - 50 Questions With Answers - LET EXAM - Questions & AnswersScribdNo ratings yet
- Study of NanofibresDocument237 pagesStudy of NanofibresGerardo ZambranoNo ratings yet
- Operation and Safety Manual: Ansi As/NzsDocument116 pagesOperation and Safety Manual: Ansi As/NzsMuhammad AwaisNo ratings yet
- Human Rights Law IntroductionDocument8 pagesHuman Rights Law IntroductionXander ZingapanNo ratings yet
- Container Generator Qac Qec Leaflet EnglishDocument8 pagesContainer Generator Qac Qec Leaflet EnglishGem RNo ratings yet
- Fibre OpticDocument16 pagesFibre OpticJoanna BaileyNo ratings yet
- Compendium 2004jan RadiographyDocument11 pagesCompendium 2004jan RadiographyAgus SusilaNo ratings yet
- Standards and Their ClassificationsDocument3 pagesStandards and Their ClassificationsJoecelle AbleginaNo ratings yet
- Bank Automation ProjectDocument75 pagesBank Automation Projectyathsih24885No ratings yet
- Manual of Establishment Sections 05ff58f7947ffb7 76283342Document271 pagesManual of Establishment Sections 05ff58f7947ffb7 76283342Vijaya KumariNo ratings yet
- Rubrics For Interd TaskDocument3 pagesRubrics For Interd Taskapi-265986384No ratings yet
- Film Crew: ProductionDocument15 pagesFilm Crew: ProductionDarkshine_THNo ratings yet
- School Bundle 05 SlidesManiaDocument19 pagesSchool Bundle 05 SlidesManiaRazeta Putri SaniNo ratings yet
- Sub Net Questions With AnsDocument5 pagesSub Net Questions With AnsSavior Wai Hung WongNo ratings yet
- DNSDocument23 pagesDNSkalugareniNo ratings yet
- Fault Code 498 Engine Oil Level Sensor Circuit - Voltage Above Normal, or Shorted To High SourceDocument13 pagesFault Code 498 Engine Oil Level Sensor Circuit - Voltage Above Normal, or Shorted To High SourceAhmedmah100% (1)
- Advances in Littorinid BiologyDocument193 pagesAdvances in Littorinid Biologyasaad lahmarNo ratings yet
- Process Validation - SDF - 1 - FDA PDFDocument111 pagesProcess Validation - SDF - 1 - FDA PDFdipakrussiaNo ratings yet
- MOB200 - Going Digital: SAP Mobile Technology Strategy and RoadmapDocument41 pagesMOB200 - Going Digital: SAP Mobile Technology Strategy and RoadmapRaviNo ratings yet
- Quality Assurance AnalystDocument2 pagesQuality Assurance AnalystMalikNo ratings yet
- Srikanth Aadhar Iti CollegeDocument1 pageSrikanth Aadhar Iti CollegeSlns AcptNo ratings yet
- 3G FactsDocument17 pages3G Factsainemoses5798No ratings yet
- TS4F01-1 Unit 4 - Document ControlDocument66 pagesTS4F01-1 Unit 4 - Document ControlLuki1233332No ratings yet