You might also like
- EXTENDED PROJECT-Shoe - SalesDocument28 pagesEXTENDED PROJECT-Shoe - Salesrhea100% (5)
- 500 Logo Design Inspirations Download #1 (E-Book)Document52 pages500 Logo Design Inspirations Download #1 (E-Book)Detak Studio DesainNo ratings yet
- Netra Case Study For EndtermDocument9 pagesNetra Case Study For EndtermGarima GeetikaNo ratings yet
- Missouri Courts Appellate PracticeDocument27 pagesMissouri Courts Appellate PracticeGeneNo ratings yet
- Intermediate Accounting (15th Edition) by Donald E. Kieso & Others - 2Document11 pagesIntermediate Accounting (15th Edition) by Donald E. Kieso & Others - 2Jericho PedragosaNo ratings yet
- The Internal Environment: Resources, Capabilities, Competencies, and Competitive AdvantageDocument5 pagesThe Internal Environment: Resources, Capabilities, Competencies, and Competitive AdvantageHenny ZahranyNo ratings yet
- ScriptDocument3 pagesScriptKaren Joy DelayNo ratings yet
- CV April 2020 PDFDocument4 pagesCV April 2020 PDFUmer KhanNo ratings yet
- Personal Profile: Dr. Said UmerDocument5 pagesPersonal Profile: Dr. Said UmerUmer KhanNo ratings yet
- Shortages of Medical Doctors in Indonesia Is It TRDocument2 pagesShortages of Medical Doctors in Indonesia Is It TRSilvanNo ratings yet
- Clinical G. I. Surgery: Book ReviewDocument2 pagesClinical G. I. Surgery: Book Reviewyacine tarikNo ratings yet
- Group4 NewService Healthcare 1Document18 pagesGroup4 NewService Healthcare 1Siddhartha LodhaNo ratings yet
- Rural HealthcareDocument13 pagesRural HealthcareIndia Heals-2020No ratings yet
- Xavier School of Rural ManagementDocument23 pagesXavier School of Rural ManagementAmulya Kumar SahooNo ratings yet
- All Aha BadDocument29 pagesAll Aha BadIrfan Ahmad KhanNo ratings yet
- 3drseetharaman Full Text With Cover Page v2Document9 pages3drseetharaman Full Text With Cover Page v2pushpal1966No ratings yet
- Final Report PDFDocument47 pagesFinal Report PDFAsad HayatNo ratings yet
- Fellowship in OncotherapeutDocument3 pagesFellowship in OncotherapeutNayan ChaudhariNo ratings yet
- 920 2859 2 PBDocument2 pages920 2859 2 PBMarcelina FAINo ratings yet
- Urology in India Numbers and PracticeDocument3 pagesUrology in India Numbers and PracticebrightozhrNo ratings yet
- Marpat 112Document23 pagesMarpat 112vision xeroxNo ratings yet
- Gaps in Health Human ResourceDocument37 pagesGaps in Health Human ResourceGeeta BhagchandaniNo ratings yet
- Human Resources For HealthDocument9 pagesHuman Resources For Healthshouka.inNo ratings yet
- Creating A Sustainable Rural General Surgery WorkforceDocument13 pagesCreating A Sustainable Rural General Surgery WorkforceJeff CrocombeNo ratings yet
- Kendhujhar Revised MSPLDocument58 pagesKendhujhar Revised MSPLRakesh MitraNo ratings yet
- Indian Rural SectorDocument8 pagesIndian Rural SectorSrikara SimhaNo ratings yet
- The Other Half From Equality To EquityDocument7 pagesThe Other Half From Equality To EquityVinay KrishnaNo ratings yet
- Abstract For ADVANCE Nurse PracticeDocument3 pagesAbstract For ADVANCE Nurse PracticeDr-Marudhar MarudharNo ratings yet
- Group1 - Section A - Aravind Eye CareDocument6 pagesGroup1 - Section A - Aravind Eye CareGopichand AthukuriNo ratings yet
- Opinion - Shall We Stop This BleedingDocument5 pagesOpinion - Shall We Stop This BleedingChandrashekhar SohoniNo ratings yet
- FUTURISTIC NURSING KitilaDocument7 pagesFUTURISTIC NURSING KitilaNoonu ChettriNo ratings yet
- Telemedicine StudyDocument7 pagesTelemedicine Studyvijju006No ratings yet
- Asm Charitable Super Specialty Hospital and Medical CollegeDocument20 pagesAsm Charitable Super Specialty Hospital and Medical CollegeTripurari KumarNo ratings yet
- Unqualified Health Care Providers and Rural Public Health in RajasthanDocument5 pagesUnqualified Health Care Providers and Rural Public Health in RajasthanIJAR JOURNALNo ratings yet
- Standard Treatment GuidelineDocument261 pagesStandard Treatment GuidelineEmaNo ratings yet
- Resolving The Paramedical Staff Shortage in India - What Are The Options - Healthcare ExecutiveDocument10 pagesResolving The Paramedical Staff Shortage in India - What Are The Options - Healthcare ExecutiveGovindNo ratings yet
- Ndizeye 2018Document8 pagesNdizeye 2018Ajup SafarudinNo ratings yet
- Human Resources For Public Health in India - Issues and ChallengesDocument13 pagesHuman Resources For Public Health in India - Issues and ChallengesHarikeshYadavNo ratings yet
- Health Care System in Pakistan .Document11 pagesHealth Care System in Pakistan .Shimmering MoonNo ratings yet
- Tele-Sehat: A Telemedicine Startup SynopsisDocument1 pageTele-Sehat: A Telemedicine Startup SynopsisRohail SiddiqueNo ratings yet
- Statement of The ProblemDocument2 pagesStatement of The ProblemCHARLESNo ratings yet
- Case Solution: Presented By: Group No.:-05 Group MembersDocument24 pagesCase Solution: Presented By: Group No.:-05 Group Memberssi ranNo ratings yet
- So Many, Yet Few: Human Resources For Health in India: Research Open AccessDocument9 pagesSo Many, Yet Few: Human Resources For Health in India: Research Open Accessshouka.inNo ratings yet
- Prevalence of Musculoskeletal Disorder and Alternative Medicine Therapies Among Dentists of North India: A Descriptive StudyDocument6 pagesPrevalence of Musculoskeletal Disorder and Alternative Medicine Therapies Among Dentists of North India: A Descriptive Studyjosselyn ayalaNo ratings yet
- Samj137inpractice WebDocument6 pagesSamj137inpractice Webabdourahmane ndongNo ratings yet
- Sop NursingDocument78 pagesSop NursingayamqNo ratings yet
- Health ManpowerDocument12 pagesHealth Manpowerswethashaki100% (1)
- How Do Rural Placements AffectDocument7 pagesHow Do Rural Placements AffectNehaNo ratings yet
- Kesiapan Perawat Indonesia Dalam Menghadapi Mea (Peluan Dan Tantangan)Document83 pagesKesiapan Perawat Indonesia Dalam Menghadapi Mea (Peluan Dan Tantangan)Mukhtar Luthfi AnshariNo ratings yet
- General Information - Health Workers - Study Endorses Introduction of Rural Health Care Workers (The Hindu-21 June 2010)Document2 pagesGeneral Information - Health Workers - Study Endorses Introduction of Rural Health Care Workers (The Hindu-21 June 2010)National Child Health Resource Centre (NCHRC)No ratings yet
- Patan Janta HospitalDocument7 pagesPatan Janta HospitaludaybhansinhjiNo ratings yet
- Narayana Hrudayalaya - Section C - Group 5Document22 pagesNarayana Hrudayalaya - Section C - Group 5raushanrahulNo ratings yet
- Ablsaka PDFDocument8 pagesAblsaka PDFSriatiNo ratings yet
- Integrated Hospital Management SystemDocument12 pagesIntegrated Hospital Management SystemPayal ThakkerNo ratings yet
- Choosing Paramedical Sciences Course As A CareerDocument3 pagesChoosing Paramedical Sciences Course As A CareerAcharya CollegeNo ratings yet
- Service Quality: An Empirical Study of Private Hospitals in Dhaka CityDocument13 pagesService Quality: An Empirical Study of Private Hospitals in Dhaka Citygubbare86No ratings yet
- Physiotherapy Awareness Among Clinical Doctors in NepalDocument15 pagesPhysiotherapy Awareness Among Clinical Doctors in NepalValentina Dela Fuente GarroneNo ratings yet
- Fit For The Future A Vision For General Prac Ce : #FuturevisiongpDocument53 pagesFit For The Future A Vision For General Prac Ce : #FuturevisiongpJohn SMithNo ratings yet
- Oncology NurseDocument4 pagesOncology NurseroesitaNo ratings yet
- Bentuk Perawat Tangguh Dan Mandiri DLM Menghadapi Mea: OlehDocument86 pagesBentuk Perawat Tangguh Dan Mandiri DLM Menghadapi Mea: OlehauliyaNo ratings yet
- Health Manpower PlanningDocument6 pagesHealth Manpower PlanningDr.K PaikNo ratings yet
- Basics of Hepatobiliary InterventionsFrom EverandBasics of Hepatobiliary InterventionsAmar MukundNo ratings yet
- Tutorials in Suturing Techniques for OrthopedicsFrom EverandTutorials in Suturing Techniques for OrthopedicsPeifu TangNo ratings yet
- Diagnostic Problems in Tumors of Central Nervous System: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Central Nervous System: Selected TopicsNo ratings yet
- Clinical Nurse Specialist Role and Practice: An International PerspectiveFrom EverandClinical Nurse Specialist Role and Practice: An International PerspectiveJanet S. FultonNo ratings yet
- BASUG School Fees For Indigene1Document3 pagesBASUG School Fees For Indigene1Ibrahim Aliyu GumelNo ratings yet
- Tanzania Finance Act 2008Document25 pagesTanzania Finance Act 2008Andrey PavlovskiyNo ratings yet
- Guide For Overseas Applicants IRELAND PDFDocument29 pagesGuide For Overseas Applicants IRELAND PDFJasonLeeNo ratings yet
- Historical Development of AccountingDocument25 pagesHistorical Development of AccountingstrifehartNo ratings yet
- Dike Calculation Sheet eDocument2 pagesDike Calculation Sheet eSaravanan Ganesan100% (1)
- Underwater Wellhead Casing Patch: Instruction Manual 6480Document8 pagesUnderwater Wellhead Casing Patch: Instruction Manual 6480Ragui StephanosNo ratings yet
- A320 TakeoffDocument17 pagesA320 Takeoffpp100% (1)
- BMA Recital Hall Booking FormDocument2 pagesBMA Recital Hall Booking FormPaul Michael BakerNo ratings yet
- POST TEST 3 and POST 4, in ModuleDocument12 pagesPOST TEST 3 and POST 4, in ModuleReggie Alis100% (1)
- Basic DfwmacDocument6 pagesBasic DfwmacDinesh Kumar PNo ratings yet
- ARUP Project UpdateDocument5 pagesARUP Project UpdateMark Erwin SalduaNo ratings yet
- MRT Mrte MRTFDocument24 pagesMRT Mrte MRTFJonathan MoraNo ratings yet
- SBL - The Event - QuestionDocument9 pagesSBL - The Event - QuestionLucio Indiana WalazaNo ratings yet
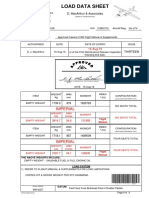
- Load Data Sheet: ImperialDocument3 pagesLoad Data Sheet: ImperialLaurean Cub BlankNo ratings yet
- Catalogo AWSDocument46 pagesCatalogo AWScesarNo ratings yet
- CodebreakerDocument3 pagesCodebreakerwarrenNo ratings yet
- Resume Jameel 22Document3 pagesResume Jameel 22sandeep sandyNo ratings yet
- CS321 Computer ArchitectureDocument160 pagesCS321 Computer ArchitectureAnurag kumarNo ratings yet
- Sourcing Decisions in A Supply Chain: Powerpoint Presentation To Accompany Powerpoint Presentation To AccompanyDocument58 pagesSourcing Decisions in A Supply Chain: Powerpoint Presentation To Accompany Powerpoint Presentation To AccompanyAlaa Al HarbiNo ratings yet
- Lockbox Br100 v1.22Document36 pagesLockbox Br100 v1.22Manoj BhogaleNo ratings yet
- Difference Between Mountain Bike and BMXDocument3 pagesDifference Between Mountain Bike and BMXShakirNo ratings yet
- Ingles Avanzado 1 Trabajo FinalDocument4 pagesIngles Avanzado 1 Trabajo FinalFrancis GarciaNo ratings yet
- Ajp Project (1) MergedDocument22 pagesAjp Project (1) MergedRohit GhoshtekarNo ratings yet
- Data Sheet WD Blue PC Hard DrivesDocument2 pagesData Sheet WD Blue PC Hard DrivesRodrigo TorresNo ratings yet
- Portrait of An INTJDocument2 pagesPortrait of An INTJDelia VlasceanuNo ratings yet